
| Sang-Min Park | 5 Articles |
Purpose
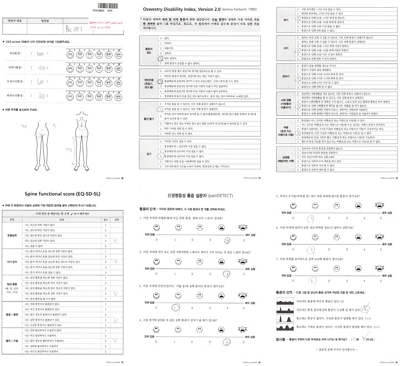
This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness. Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations. Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review. Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
Background
This study aims to assess the clinical and radiographic outcomes of biportal endoscopic lumbar discectomy compared to microscopic lumbar discectomy in obese patients with lumbar herniated discs. Previous research has established a positive correlation between operation time and estimated blood loss in obese patients undergoing microscopic lumbar discectomy, based on an increase in body mass index. However, no studies have specifically examined the outcomes of biportal endoscopic lumbar discectomy in this patient population. Therefore, this study seeks to fill this research gap and provide valuable insights into the effectiveness of these two surgical approaches for obese patients with lumbar herniated discs. Methods This retrospective multicenter study analyzed and compared clinical and radiological data from 48 obese patients with a body mass index (BMI) greater than 30 kg/m2 who underwent either microscopic or biportal endoscopic lumbar discectomy. The study assessed clinical outcomes using the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores. Radiological data were obtained through magnetic resonance imaging (MRI) scans. Results The study included a total of 48 patients, with 31 patients undergoing microscopic discectomy and 17 patients undergoing biportal endoscopic discectomy. Both groups showed improvements in VAS, ODI, and EQ-5D scores following surgery compared to preoperative scores. However, there was no significant difference in these outcome measures between the two surgical techniques. Although there was a no significant difference in the occurrence of recurrent disc herniation confirmed by postoperative MRI, there was significant difference in the number of patients requiring additional surgery between the two groups. Conclusions For obese patients with lumbar disc herniation that did not respond to conservative treatment, this study found no significant differences in clinical or radiological outcomes between microscopic and biportal endoscopic surgery methods. However, it is worth noting that the biportal group had a lower incidence of reoperation compared to the microscopic group.
Background
When obese patients underwent lumbar discectomy using a microscope, a correlation was found between the operation time and an increase in estimated blood loss according to the increase in body mass index. However, except for minor complications, there was no difference in postoperative outcomes between obese and normal-weight patients. These are the results of microscopic lumbar discectomy in obese patients, but there are no studies on biportal endoscopic lumbar discectomy. The aim of this study was to compare the clinical and radiographic outcomes of microscopic and endoscopic discectomy in obese patients. Methods Clinical and radiological data were compared and analyzed in 23 obese patients with a body mass index of >30 kg/m2 who underwent microscopic and biportal endoscopic lumbar discectomy. Clinical data on the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores were measured, and radiological data were measured using magnetic resonance imaging (MRI). Results In total, 13 patients who underwent microscopic discectomy and 10 who underwent biportal endoscopic discectomy were enrolled in this study. The VAS, ODI, and EQ-5D scores in both groups improved after surgery compared with those before surgery, although there was no difference between the two groups. Although there was a difference in the incidence of recurrent disc herniation confirmed by MRI after surgery, there was no difference in the number of patients requiring surgery between the two groups. Conclusions There were no significant clinical or radiological differences in outcomes between microscopic and biportal endoscopic surgery methods.
Objectives
The primary surgical goals when treating a spinal metastasis are usually pain relief and preservation of ambulatory function. Minimally invasive techniques have become popular, being associated with less morbidity and mortality than conventional open surgeries. Materials and Methods Between April 2012 and September 2016, 15 consecutive patients underwent percutaneous pedicle screw fixation (PPSF) to treat spinal metastases. We retrospectively analyzed prospectively collected data, including visual analog scale (VAS) pain scores, Frankel scale scores, and complications. Results Fifteen patients (8 males, 7 females; mean age 61 years) underwent surgery under general anesthesia. PPSF was performed on all patients, and two with poor bone quality underwent cement augmentation of the manipulated vertebra(e) just prior to pedicle screw insertion. Seven patients underwent fixation plus distraction (indirect decompression via ligamentotaxis) and two laminectomies (direct decompression) of the spinal cord. Two patients developed screw pullout requiring revision surgery. One patient died 7 days after surgery from liver cirrhosis and sepsis. All patients reported that pain was reduced after surgery. After surgery, 12 patients regained ambulatory capacity. Nine patients died during follow-up; the mean overall survival time was 14.1 months. Conclusions PPSF is a safe and minimally invasive palliative surgery option for patients with spinal metastases.
Purpose
To compare the difference of cervical alignment between cervical lateral radiograph and whole-spine lateral radiograph by the effects of radiographic position and to assess the effect of the shoulder flexed position to cervical lordotic curvature and head position. Materials and Methods We retrospectively evaluated 43 asymptomatic adult patients who were taken horizontal gazing standing cervical and whole-spine lateral radiograph simultaneously from Sep. 2008 to Dec. 2009. Cervical lateral radiograph was taken with the arms extended and hand gently clasped on both side and whole-spine lateral radiograph was taken in the position that subject were relaxed standing with fists-on-clavicles position. Cervical sagittal alignment were analyzed the following parameters. (1) Gore angle (GA, C2-7 angle); (2) Cobb angle (CA, C2-7 angle); (3) translation distance (TD, distance of C2 compared with vertical line through the posterior-inferior body of C7); (4) McGregor angle (MA, angle between McGregor line and horizontal line). Results The mean of GA and CA in cervical radiograph were -12.64° and -9.96°, whereas -7.12° and -4.98° in wholespine radiograph. The mean TD and MA were in cervical radiograph were 16.95mm and 7.15°, whereas, 14.97mm and 6.54° respectively in whole-spine radiograph. Conclusion Our study showed the significant differences of cervical alignment and head position between standing cervical lateral and whole-spine lateral radiograph. The radiographic posture of whole-spine lateral radiograph with horizontal gazing and fists-on-clavicles position make cervical alignment and head position less lordotic and posterior translation compared to cervical radiograph.
|
|
