Purpose This study aimed to evaluate whether percutaneous vertebroplasty (PVP) contributes to vertebral height restoration and sagittal alignment correction in osteoporotic vertebral compression fractures (OVCF), focusing on thoracolumbar junction fractures.
Methods A retrospective review of 40 patients with single-level OVCF at T10–L2 treated with PVP was performed. Vertebral heights (anterior, middle, and posterior) and sagittal alignment (thoracic kyphosis, lumbar lordosis, sagittal vertical axis, and segmental Cobb's angle) were measured preoperatively, at 3 months, and at 6 months. Clinical outcomes included visual analog scale and EuroQol-5 Dimensions.
Results Significant pain relief and improvement in quality of life were observed at 6 months postoperatively. Vertebral height restoration, particularly in the anterior and middle portions, was noted at 3 months; however, partial loss of the restored height occurred by 6 months. Most sagittal alignment parameters showed no significant postoperative change, although lumbar lordosis significantly increased, resulting in a reduced pelvic incidence–lumbar lordosis mismatch.
Conclusion PVP provides meaningful clinical improvement in thoracolumbar OVCFs and offers early vertebral height restoration; however, this radiologic benefit is not sustained over time. While limited improvement in lumbar lordosis was observed, PVP does not substantially correct global sagittal alignment. These findings suggest that PVP should be considered primarily a pain-relieving and stabilizing procedure rather than a deformity-correcting intervention.
Study Design The study was designed as a retrospective clinical study.
Purpose This study aimed to demonstrate that solid fusion and favorable outcomes can be achieved even without fusion extension through the application of an allograft bone chip insertion technique.
Overview of Literature: Screw loosening and nonunion are common complications following lumbar posterior fixation, often resulting from fusion failure. The optimal surgical strategy remains controversial, and most surgeons prefer extending fusion levels above or below the affected segment.
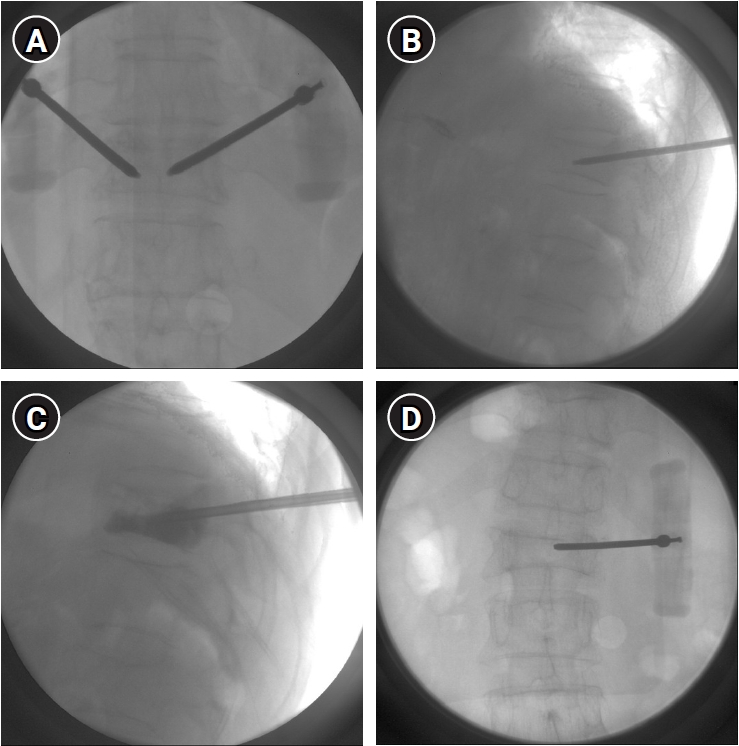
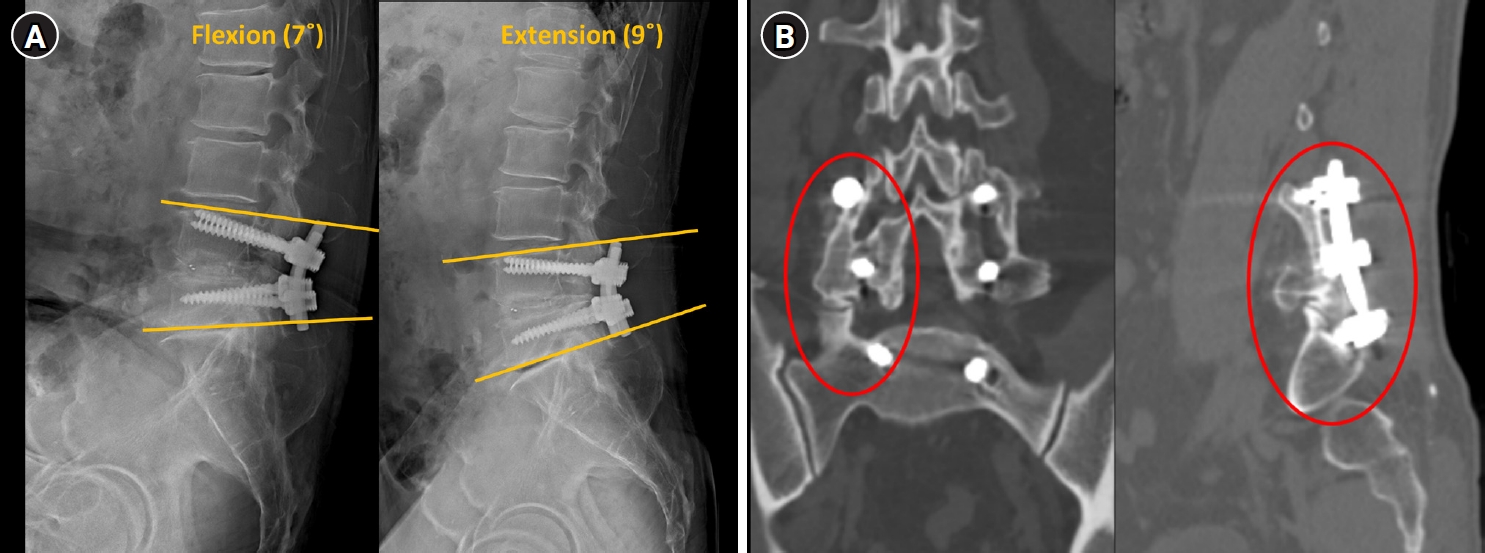
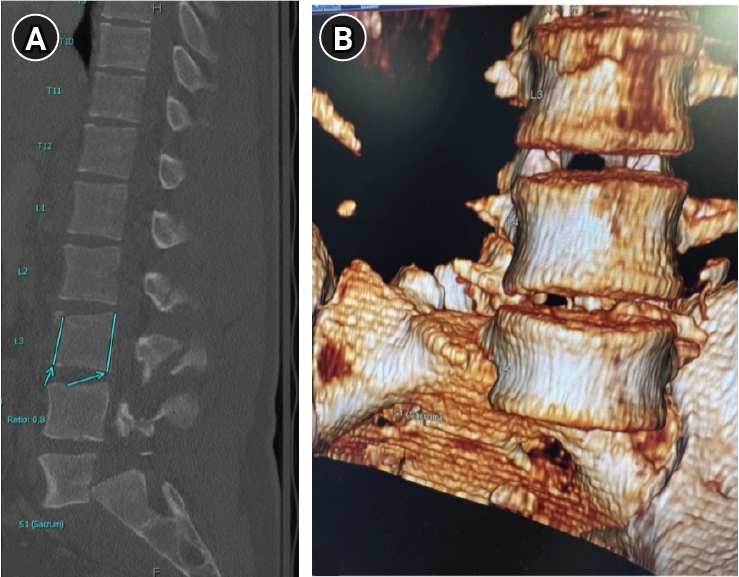
Methods Twelve patients who underwent revision surgery for screw loosening and nonunion by a single surgeon were retrospectively analyzed. Allograft bone chips were inserted into loosened screw holes to enhance fixation and promote fusion. Radiologic outcomes were evaluated at 1 year using dynamic flexion–extension X-ray and computed tomography (CT). Solid fusion was defined as ≤3° of motion on X-ray and, in eight patients with CT, as a continuous trabecular bone bridge. Clinical outcomes were assessed using the numerical rating scale (NRS) for back and leg pain and the Oswestry Disability Index (ODI).
Results From January 2020 to February 2022, 12 patients (7 men, 5 women; mean age, 65.8 years) underwent surgery. Eight were treated without fusion extension, three required one-level extension for adjacent segmental disease, and one for deformity correction. At 1 year, all patients achieved solid fusion with ≤3° motion, and CT confirmed a trabecular bone bridge in eight cases. Mean NRS scores for back and leg pain improved by 6.9 and 5.1 points, respectively, and ODI showed marked functional recovery.
Conclusion The allograft bone chip insertion technique appears to be a practical revision option for managing screw loosening and nonunion in selected patients. It can achieve solid fusion and favorable outcomes without fusion extension, thereby minimizing surgical morbidity and preserving motion segments.
Study Design A retrospective diagnostic accuracy study was conducted using internal training and temporal validation cohorts.
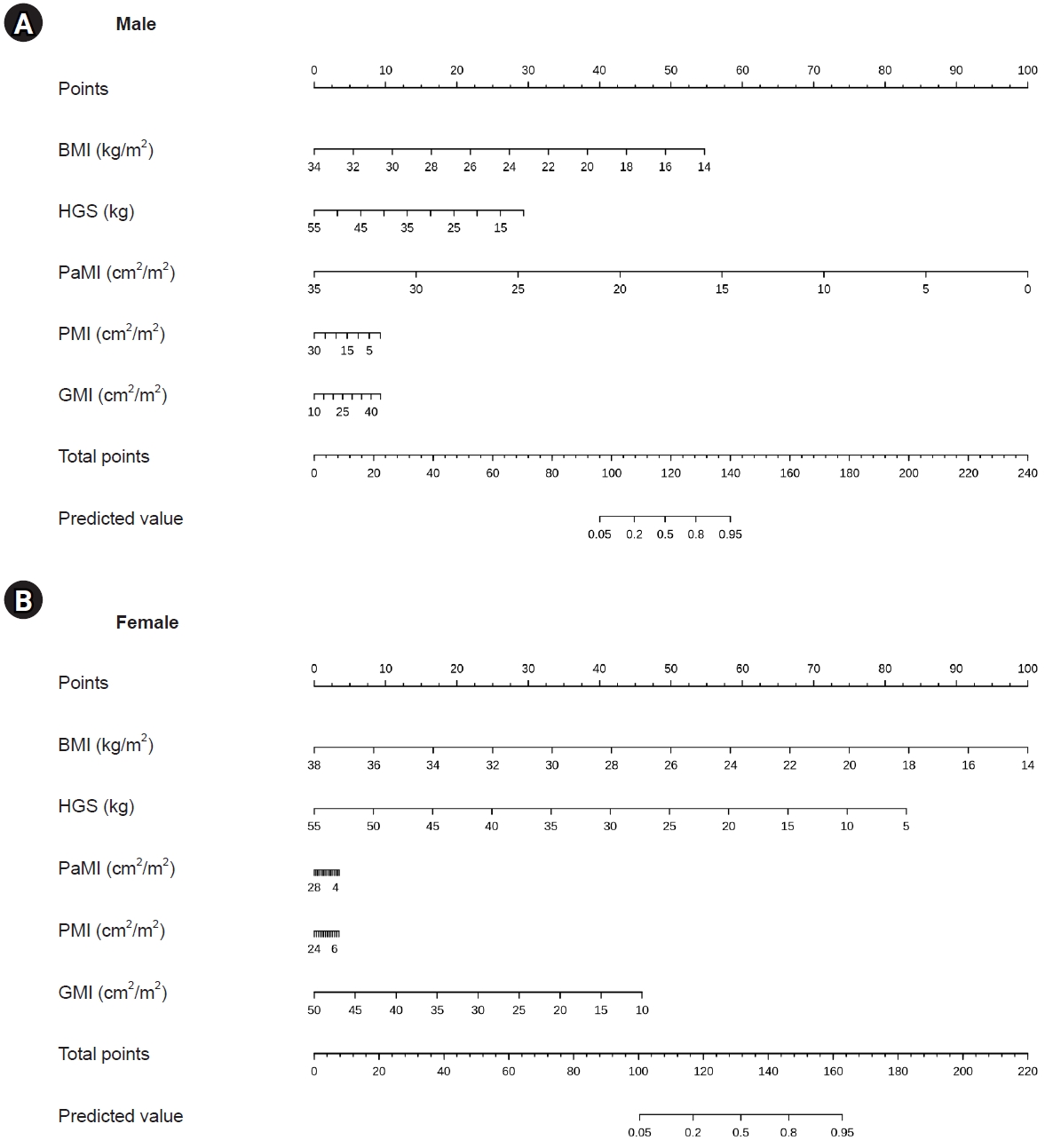
Purpose This study aimed to develop and validate sex-specific diagnostic nomograms for sarcopenia in patients with degenerative lumbar disease (DLD), based on body mass index (BMI), hand-grip strength (HGS), and computed tomography (CT)–derived lumbar muscle indices.
Overview of Literature: The Asian Working Group for Sarcopenia (AWGS) 2019 algorithm requires appendicular skeletal muscle mass (ASM) measurement by dual-energy X-ray absorptiometry or bioimpedance analysis together with HGS and a physical performance test. These measurements are not always feasible in spine clinics, although a preoperative lumbar CT is routinely available.
Methods A training set of 196 patients scheduled for lumbar surgery and a temporal validation set of 150 patients with DLD were analyzed. Sarcopenia was diagnosed according to the AWGS 2019 criteria. Sex-specific multivariable logistic regression was performed using BMI, HGS, psoas muscle index, paraspinal muscle index (PaMI), and gluteal muscle index (GMI), and the resulting models were translated into nomograms. Discrimination was assessed by the area under the receiver operating characteristic curve (AUC), calibration by calibration plots and mean absolute error (MAE), and the optimal cut-off was identified using the Youden index.
Results The prevalence of sarcopenia was 62.2% (122/196) in the training set and 58.0% (87/150) in the validation set. In the training set, sarcopenic patients had significantly lower BMI (23.7±3.7 vs. 27.0±3.3 kg/m2), HGS (20.3±8.0 vs. 29.2±30.5 kg), PaMI (8.7±5.4 vs. 13.9±8.0), and GMI (26.1±5.7 vs. 30.9±6.2) than non-sarcopenic patients (all p<0.05). On validation, the male nomogram achieved an AUC of 0.958 with an MAE of 0.040, and the female nomogram achieved an AUC of 0.830 with an MAE of 0.021. The Youden index was 0.78 for males and 0.59 for females.
Conclusion Sex-specific nomograms based on BMI, HGS, and CT-derived lumbar muscle indices provided accurate diagnosis of sarcopenia in patients with DLD without requiring whole-body ASM measurement or a physical performance test, offering a practical screening tool in the spine clinic.
Purpose This retrospective study investigated the distinct clinical and radiographic drivers of early- versus late-onset proximal junctional kyphosis (PJK) following multilevel thoracolumbar (TL) fusion.
Methods After applying the exclusion criteria (spinal infection, neuromuscular disease, age <50 years), the analysis included 136 patients who underwent ≥4-level TL fusion and were followed up for a minimum of 2 years. PJK was classified as early (≤6 months) or late (>6 months) onset. Patient-related factors, surgical variables, sagittal spinopelvic parameters, and preoperative magnetic resonance imaging findings were analyzed using multivariate logistic regression to identify independent predictors of early PJK.
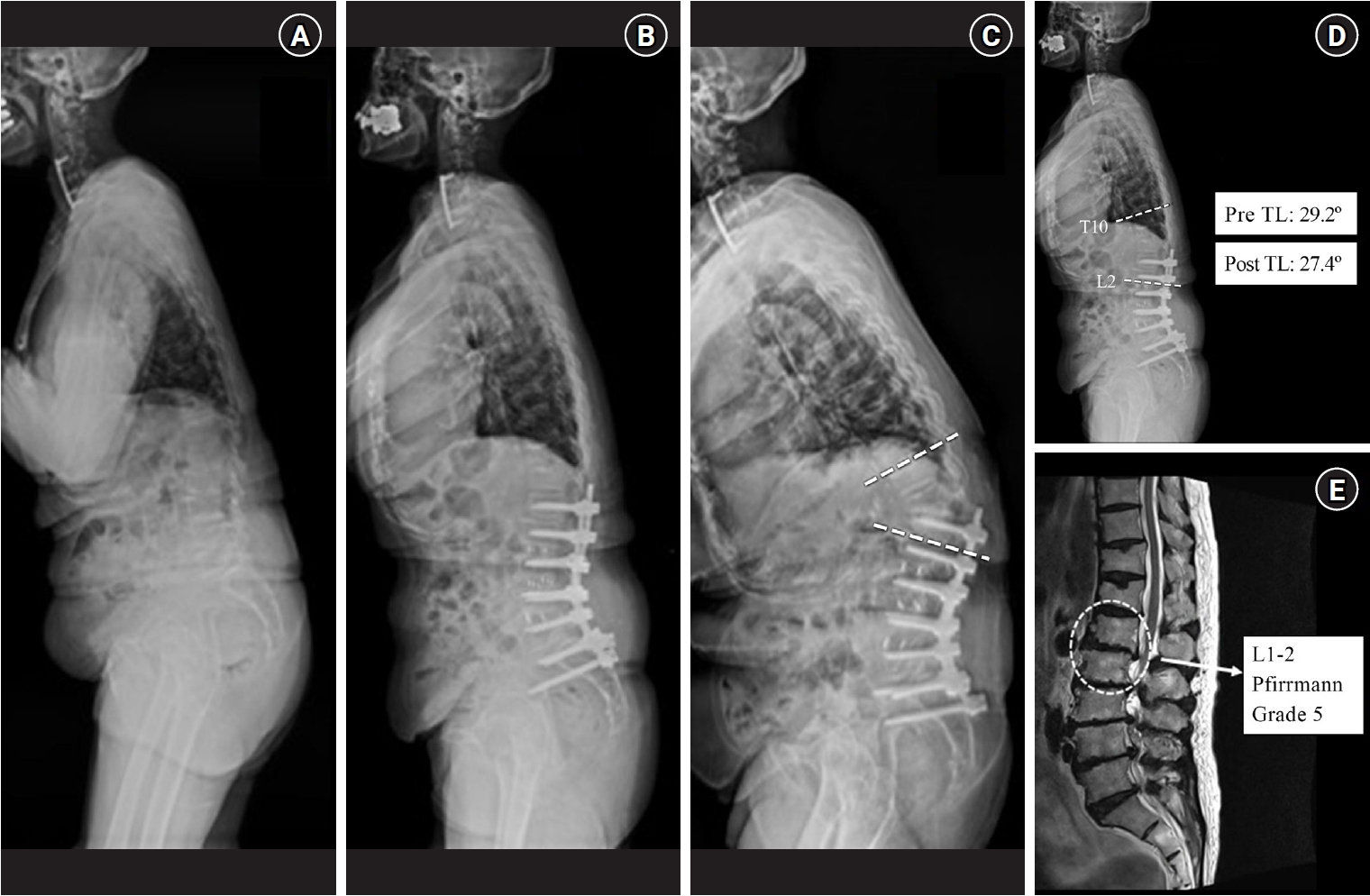
Results Among 24 patients (17.6%) who developed PJK, the early and late-onset groups included 13 and 11 patients, respectively. The early PJK group exhibited significantly greater preoperative and postoperative TL angles compared with the late group (preoperative: 23.03±13.83° vs. 9.67±9.67°, p=0.024; postoperative: 19.6±6.95° vs. 6.95±6.35°, p<0.001). The Pfirrmann grade of the L1–2 intervertebral disc was significantly higher in the early PJK group (3.92±0.95 vs. 2.81±0.60, p=0.006). No surgical variables differed significantly between the groups. Multivariate analysis confirmed greater postoperative TL angle and more advanced L1–2 disc degeneration as independent predictors of early PJK.
Conclusion Early-onset PJK following multilevel TL fusion is primarily driven by regional biomechanical vulnerabilities, specifically residual postoperative TL kyphosis and advanced adjacent L1–2 disc degeneration, rather than by surgical variables. Meticulous evaluation of regional TL alignment and adjacent disc health during surgical planning is critical for risk stratification and prevention of early junctional failure.
Study Design This study was a retrospective single-center cohort study.
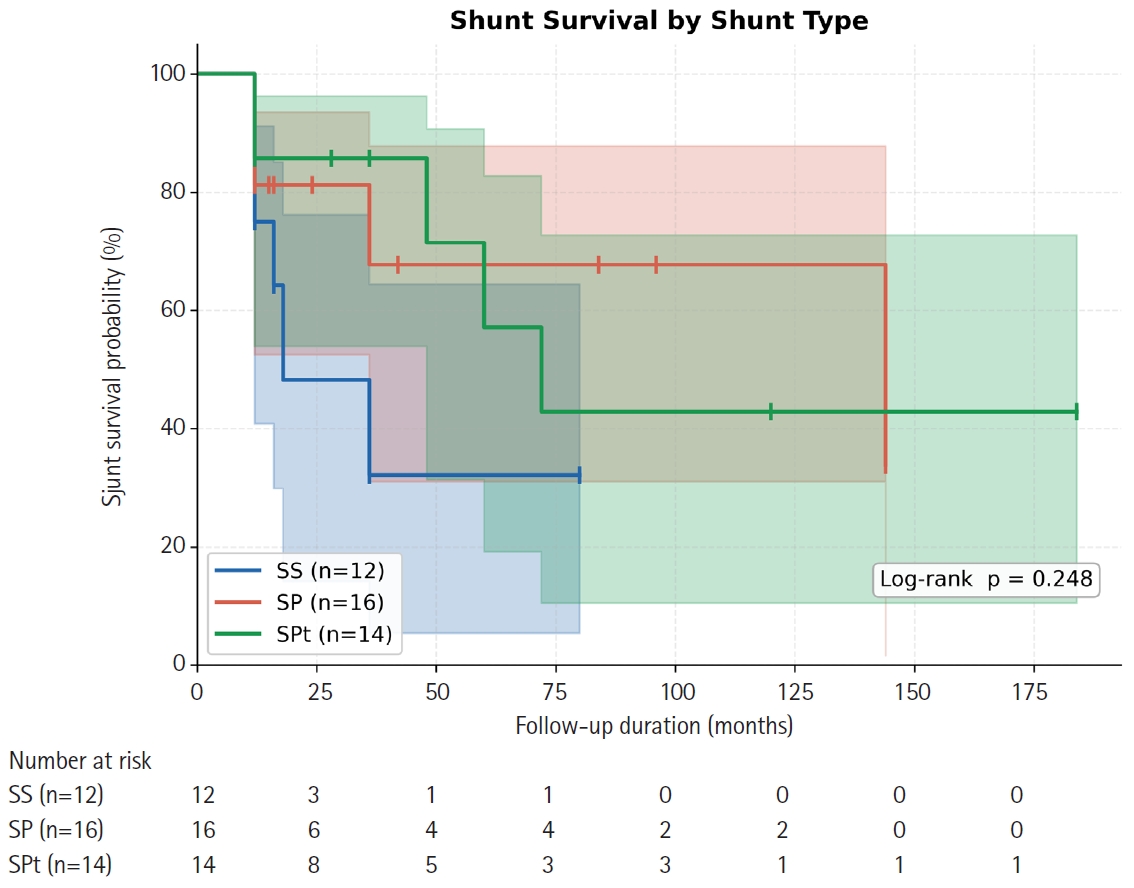
Purpose This study aimed to compare long-term shunt patency by shunt type (syringo-subarachnoid [SS], syringo-pleural [SP], syringo-peritoneal [SPt]) and disease etiology (post-traumatic, post-infectious, idiopathic) in patients surgically treated for syringomyelia, using Kaplan-Meier survival methodology.
Overview of Literature: Syringomyelia shunting carries a well-documented revision burden, but direct comparative survival data across shunt modalities and etiologic subgroups are scarce, particularly from East Asian centers.
Methods We retrospectively analyzed 42 patients (mean age, 47.6±11.8 years; 57.1% male) who underwent syringomyelia shunting at a tertiary neurosurgical center (January 2000–December 2020) with ≥12 months follow-up. Shunt type was classified as SS (n=12), SP (n=16), or SPt (n=14); etiology as post-traumatic (n=24), post-infectious (n=10), idiopathic (n=6), or hemorrhage/tumor-related (n=2). The primary endpoint was shunt revision surgery. Kaplan-Meier analysis, log-rank testing, and Cox proportional hazards regression were performed.
Results Over a median follow-up of 15 months (range, 12 to 184 months), 16 patients (38.1%) underwent shunt revision. Overall 12- and 24-month patency rates were 79.6% and 72.5%, respectively (median shunt survival 72 months). By shunt type, 12-month patency was 75.0% (SS), 81.3% (SP), and 85.7% (SPt); 24-month patency declined to 48.2% for SS while SP and SPt remained at 81.3% and 85.7% (log-rank p=0.248). Post-infectious syringomyelia showed the shortest median shunt survival (36 months) compared with post-traumatic (not reached) and idiopathic (not reached) groups (log-rank p=0.232). No independent predictor of shunt failure was identified on multivariate Cox regression.
Conclusion All three shunting techniques achieve approximately 80% one-year patency. SS may carry a higher long-term occlusion risk. Post-infectious syringomyelia requires closer postoperative surveillance. Larger prospective studies are needed to establish definitive shunt selection criteria.
Traumatic lumbar spondyloptosis is a rare entity associated with high-velocity mechanisms and is the most severe form of lumbar spondylolisthesis. Operative management is often required; however, the relative merits of reduction versus in situ fusion remain debated, largely owing to the technical difficulty of attaining satisfactory fracture reduction. In this report, we describe external femoral traction as a novel technique for closed reduction of traumatic lumbar spondyloptosis. A 27-year-old man presented after a tree he was cutting fell on him and was found to have T3–7 AO Spine (AOS) A1 fracture, L3 AOS B2 fracture, and L5 AOS C fracture. Neurologic exam was consistent with multilevel nerve root injury. Definitive treatment included bilateral femoral traction, open reduction, and combined anterior/posterior fixation. A multidisciplinary team including orthopedic surgery, plastic surgery, vascular surgery, and neurosurgery were involved. Complete reduction was obtained, and the patient experienced near-complete resolution of neurologic symptoms. This technique offers a unique solution to the challenge of traumatic lumbar spondyloptosis. Further study and follow-up are needed to confirm the utility and durability of this technique and the cranial extent of injury for which this technique might be applied.
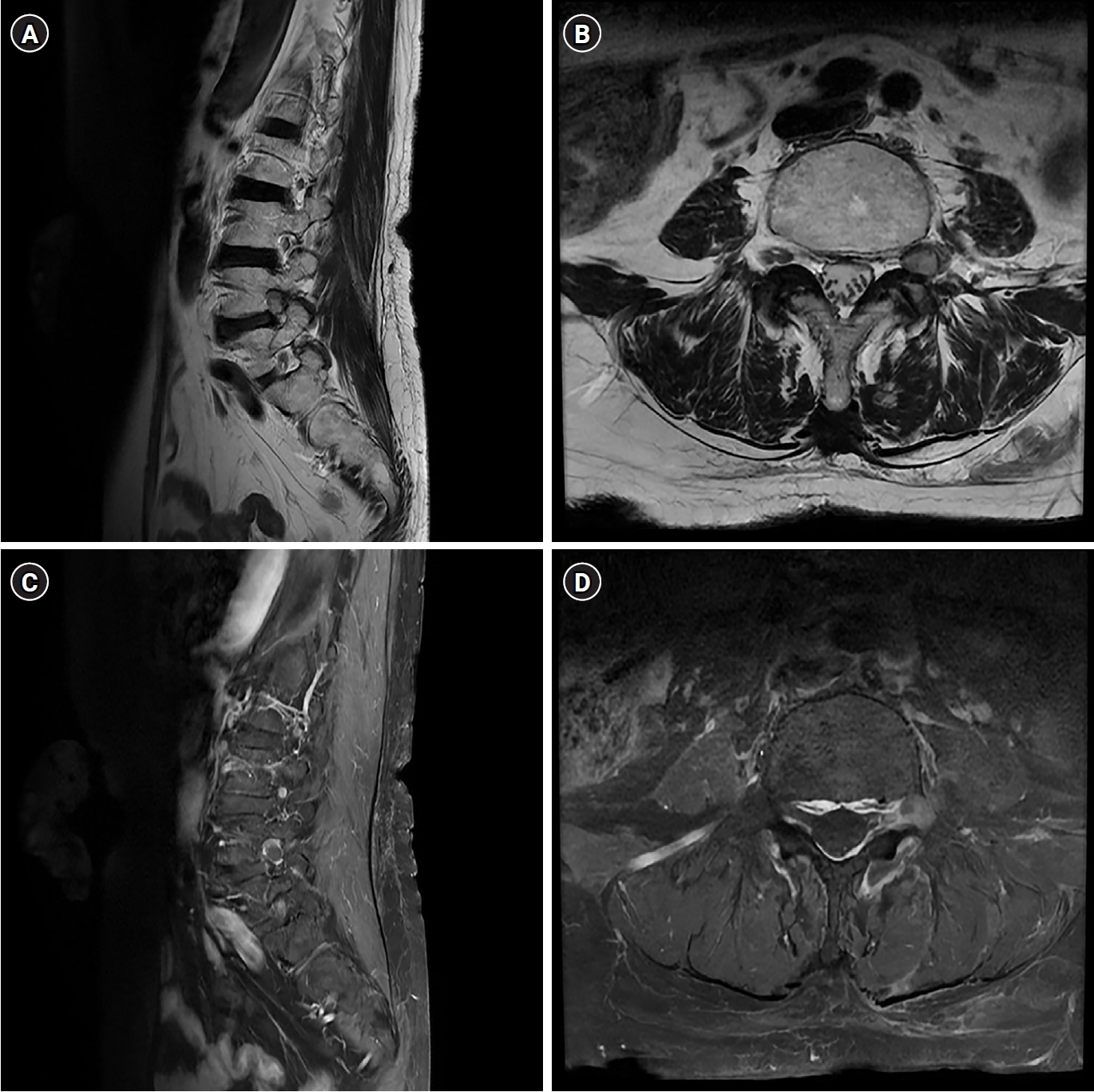
Chondroma is a benign cartilaginous neoplasm, rarely encountered in the lumbar spine. We report a case involving a 70-year-old female who presented with lower limb radiating pain that started four years ago. Although no pronounced muscle weakness was noted, the patient experienced progressively worsening radiating pain in the L4 dermatome. Initial evaluation, including magnetic resonance imaging (MRI) performed at another medical facility, suggested a potential lesion associated with left L4–5 lumbar disc herniation. Despite non-surgical interventions, the patient experienced limited symptomatic relief, prompting her to seek further care at our clinic. Subsequent contrast-enhanced MRI conducted at our facility revealed a mass exhibiting peripheral rim enhancement surrounding the L4 nerve root. Suspecting a neurogenic tumor, we decided to perform surgical excision of the mass. Postsurgery, histopathological analysis confirmed the presence of hyaline cartilage with lobular architecture and chondrocytes in lacunae, leading to the conclusive diagnosis of chondroma. Following the surgical procedure, the previously reported radiating pain exhibited notable improvement.
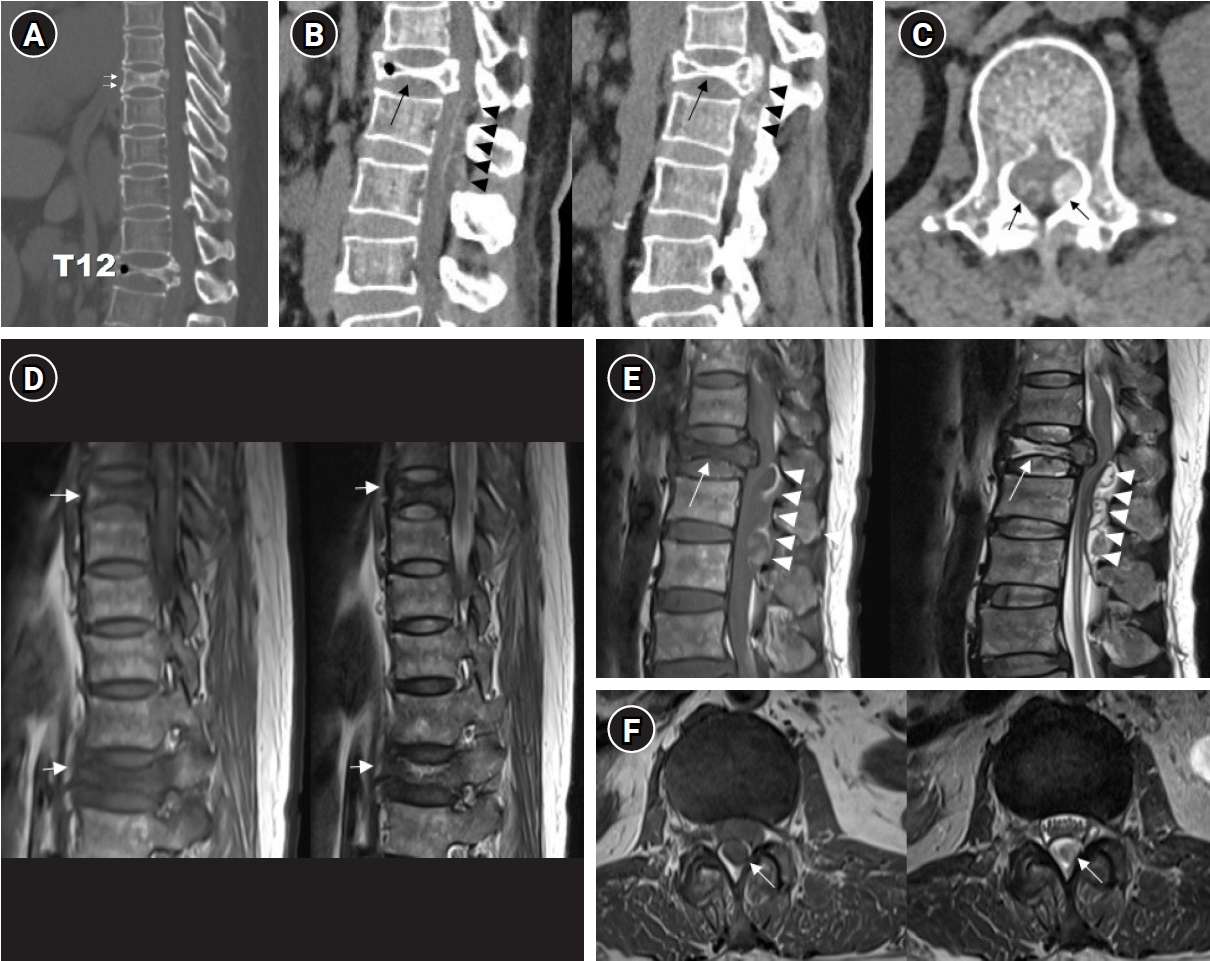
The incidence of compression fractures is increasing in aging populations. Differentiating pathological fracture types is complex and requires careful consideration during diagnosis. This case report describes the clinical course of a 54-year-old female patient presenting with progressive paraplegia after a back injury sustained while lifting a heavy object. Initial imaging revealed a burst fracture at T12 and severe spinal cord compression due to an epidural mass extending from T12 to L2. Clinical assessment raised suspicions of a hematologic malignancy or pathological fractures. Laminectomy and spinal fusion, along with mass removal, resulted in partial improvement in motor function and patient-reported pain levels. However, further evaluation and biopsy revealed chronic inflammation with fibrosis consistent with an unresolved hematoma. This case underscores the importance of a comprehensive differential diagnosis and multidisciplinary collaboration, integrating radiologic, surgical, and pathologic correlation, in the management of complex spinal pathologies.
Postoperative radicular pain may persist after lumbar spine surgery despite adequate decompression and the absence of a definite compressive lesion on imaging. Management of such cases remains challenging. This study aimed to report the clinical outcomes of combined pulsed radiofrequency (PRF) and low-temperature thermal radiofrequency. We retrospectively reviewed two patients with postoperative radicular pain without evidence of a high-grade compressive lesion. Both patients showed temporary relief after selective nerve root block. PRF (42°C, 120 seconds), followed by low-temperature thermal radiofrequency (55°C, 60 seconds), was applied under fluoroscopic guidance. Both patients demonstrated significant pain reduction without neurological complications, and symptom improvement was maintained for at least 12 months. The combination of PRF and low-temperature thermal radiofrequency may represent a feasible minimally invasive treatment option. Further studies are required to clarify its effectiveness and indications.
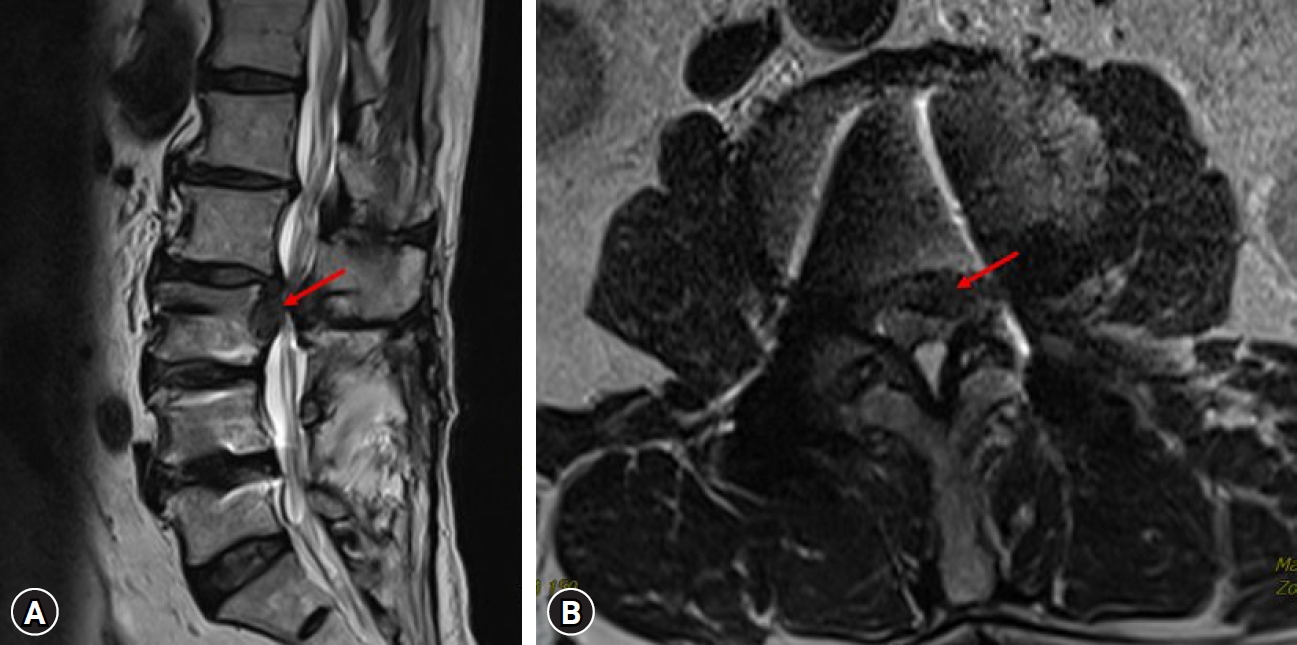
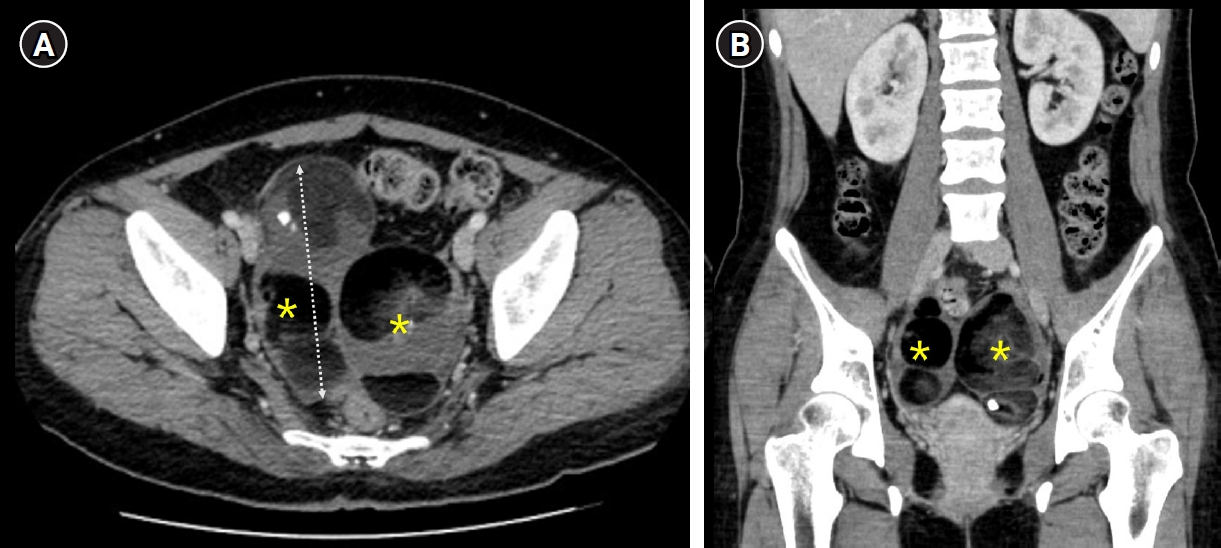
Dysplastic spondylolisthesis is a developmental subtype characterized by congenital lumbosacral abnormalities and progressive instability. Primary presentation with cauda equina syndrome (CES) has rarely been reported. We report a rare case of CES associated with highgrade dysplastic spondylolisthesis in a patient with concurrent giant ovarian teratomas, which contributed to delayed diagnosis and treatment because of overlapping pelvic symptoms. The patient presented with progressive urinary dysfunction, saddle anesthesia, and lower- extremity symptoms. Radiographic evaluation demonstrated high-grade L5–S1 dysplastic spondylolisthesis with severe canal compromise and lumbosacral deformity. Surgical treatment involved neural decompression and controlled deformity correction with sacral dome osteotomy and interbody fusion performed under provisional stabilization. Postoperatively, the patient demonstrated meaningful neurological recovery with improvement of urinary symptoms and restoration of lumbosacral alignment. This case highlights that CES can occur as an initial manifestation of dysplastic spondylolisthesis and underscores the importance of early spinal evaluation and timely surgical treatment with appropriate reduction techniques to prevent further neurological deterioration in patients with persistent neurological symptoms.



 First
First Prev
Prev

