Purpose To develop and validate a deep learning–based artificial intelligence (AI) model for automated measurement of lumbar lordosis (LL) angles from whole spine lateral radiographs.
Materials and Methods A total of 888 lateral spine X-rays (2019–2021) were retrospectively collected and annotated with four anatomical keypoints (L1 and S1 vertebral landmarks). An AI model using Detectron2 with a Keypoint R-CNN and ResNeXt-101 backbone was trained with data augmentation. Performance was evaluated on 50 test images, comparing AI results to manual annotations by two orthopedic surgeons using intraclass correlation coefficient (ICC), Pearson’s correlation, and Bland–Altman analysis.
Results The model achieved an average precision of 71.63 for bounding boxes and 86.61 for keypoints. ICCs between AI and human raters ranged from 0.918 to 0.962. Pearson correlation coefficients were r=0.849 and r=0.903. Bland–Altman analysis showed minor underestimation biases (–3.42° and –4.28°) with acceptable agreement.
Conclusions The AI model showed excellent agreement with expert measurements and high reliability in LL angle assessment. Despite a slight underestimation, it offers a scalable, consistent tool for clinical use. Further studies should evaluate generalizability and interpretability in broader settings.
Citations
Citations to this article as recorded by
Deep Learning–based AI Analysis of the Correlation Between Lumbar Lordosis and Age Soo-Bin Lee, Ja-Yeong Yoon, Dong-Sik Chae, Sang-Bum Kim, Young-Seo Park, Kyung-Yil Kang, Min-Kyu Lee Journal of Advanced Spine Surgery.2025; 15(2): 78. CrossRef
Efficacy of Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Meta-Analysis With Single-Arm Analysis and Comparative Analysis With Microscopic Decompression and Uniportal Endoscopic Decompression Shuangwen Lv, Haiwen Lv, Yupeng He, Xiansheng Xia Operative Neurosurgery.2024; 27(2): 158. CrossRef
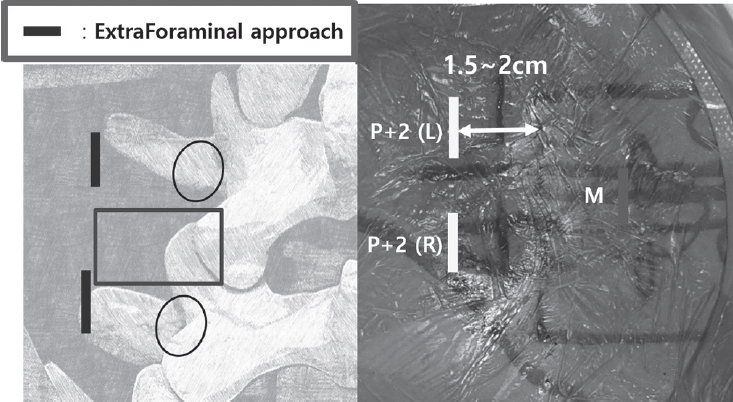
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Purpose This study aimed to compare the clinical effectiveness and potential benefits of ultrasound (US)-guided versus fluoroscopy (FL)-guided cervical retrolaminar block (RLB) in patients with cervical facet joint pain.
Materials and Methods A total of 27 patients aged 40 years or older who were diagnosed with cervical facet joint syndrome based on physical examination and imaging modalities were included. 12 patients of group I treated with US-guided RLB and 15 patients of group II treated with FL-guided RLB. The position of the needle and the distribution of contrast agent were confirmed using fluoroscopic images, and the changes in numeric rating scale (NRS) and neck disability index (NDI) before and 2 weeks after the procedure were compared in the two groups.
Results Radiologically, the target agreement of needle placement in group I was 75%. There was no difference in contrast medium spread between the two groups. Clinically, the mean NRS improved from 7.08±0.52 to 3.08±0.90 in group I (p=0.01) and from 7.20±0.56 to 3.33±0.72 in group II (p=0.01). The mean NDI decreased from 41.67±2.27 before the procedure to 20.83±2.33 after the procedure in group I (p=0.01), and from 40.87±2.61 before the procedure to 21.67±2.02 after the procedure in group II (p=0.01), with no difference between the two groups.
Conclusions US-guided cervical RLB is an effective, radiation-free alternative to FL-guided RLB for managing cervical facet joint pain, offering comparable pain relief and functional improvement.
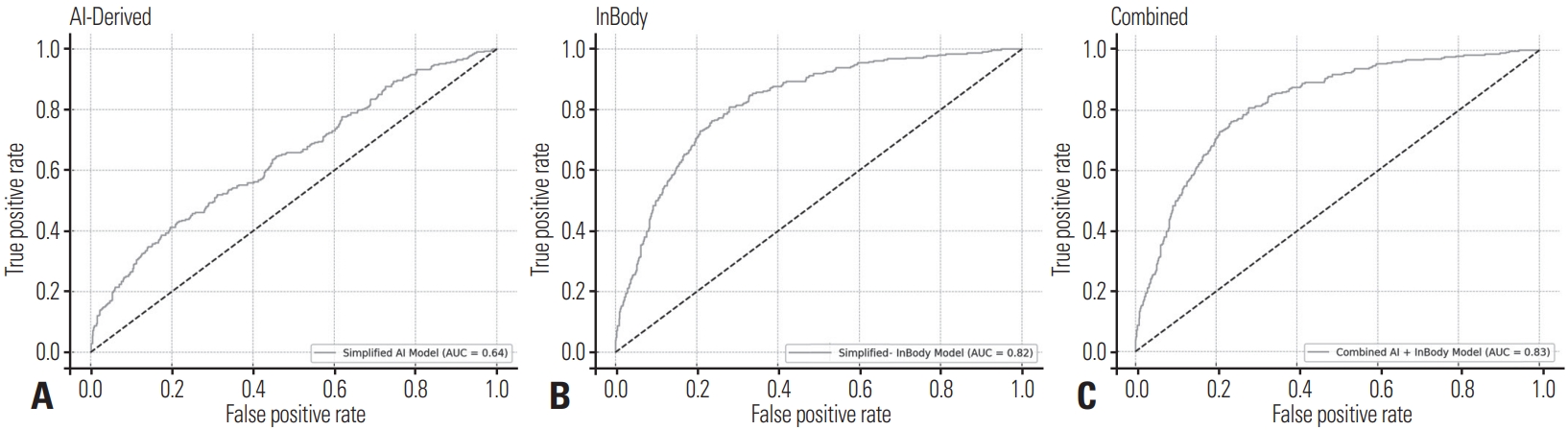
Purpose Metabolic syndrome is a multifactorial condition associated with increased risks of cardiovascular disease and type 2 diabetes. This study aims to evaluate whether combining AI-based abdominal CT metrics with traditional InBody analysis enhances the prediction of metabolic syndrome.
Materials and Methods This retrospective study included 977 adults who underwent both abdominal CT and InBody assessments. AI-derived measurements were obtained using a deep-learning V-Net model trained to segment seven body tissue types. InBody measurements included BMI, body fat percentage, fat mass, and waist-hip ratio. Metabolic syndrome was defined by NCEP-ATP III criteria. Logistic regression and ROC analyses were used to evaluate the predictive performance of AI-derived metrics, InBody metrics, and their combination.
Results Body fat percentage and waist-hip ratio from InBody analysis were strong predictors of metabolic syndrome (AUC 0.82). AI-derived visceral fat was also significantly associated with metabolic syndrome (AUC 0.61). Combining both AI and InBody metrics slightly improved predictive performance (AUC 0.83), indicating a complementary diagnostic value.
Conclusions While InBody metrics remain superior in predicting metabolic syndrome due to their close association with metabolic processes, AI-derived body composition metrics, particularly visceral fat, offer structural insights. The modest improvement in prediction when combined suggests the potential of an integrated diagnostic model in clinical practice.
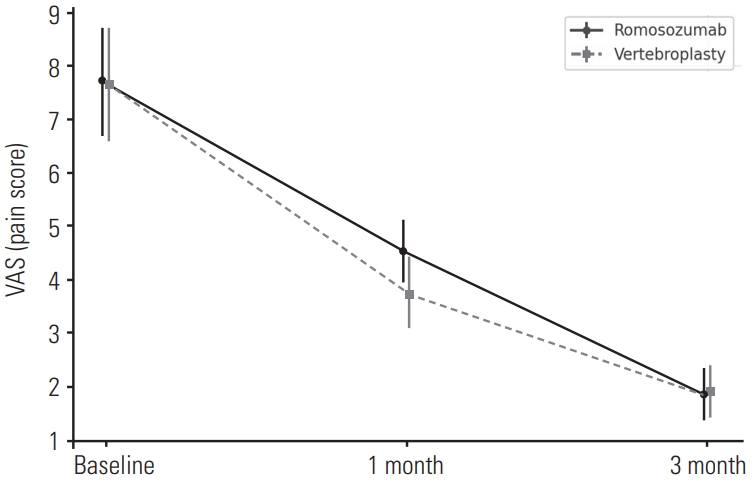
Purpose To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
Material and Methods: This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
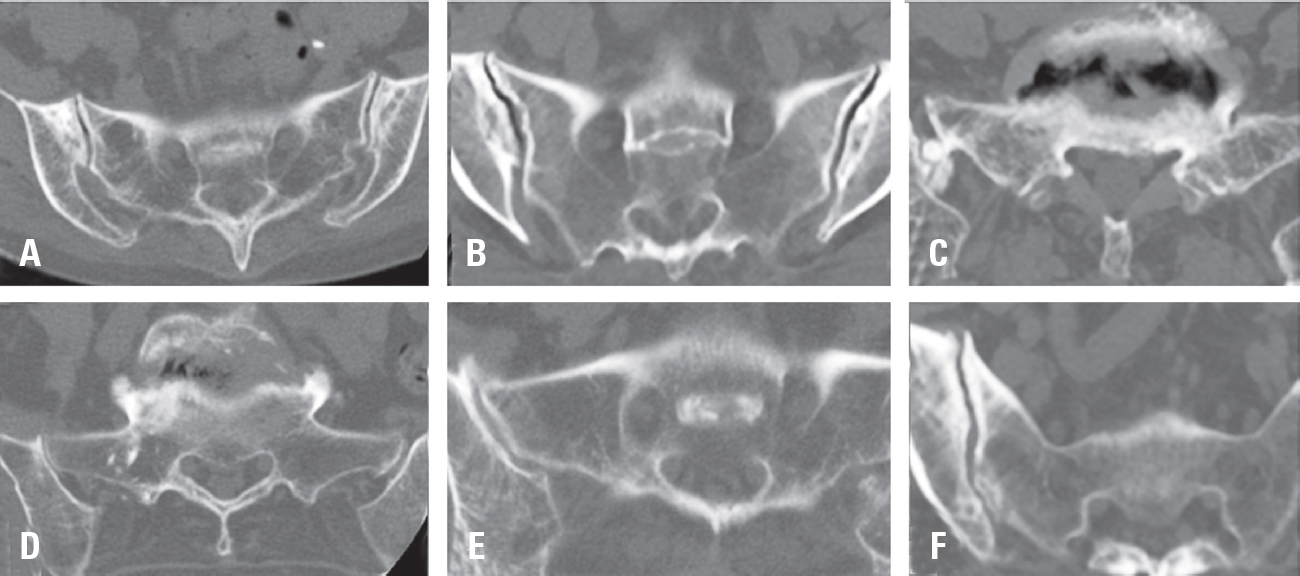
Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
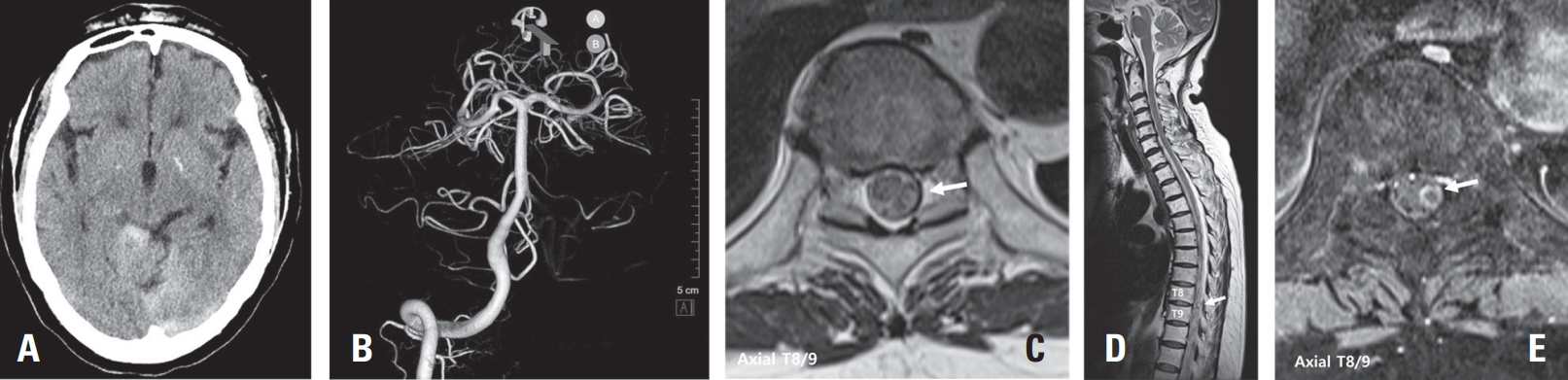
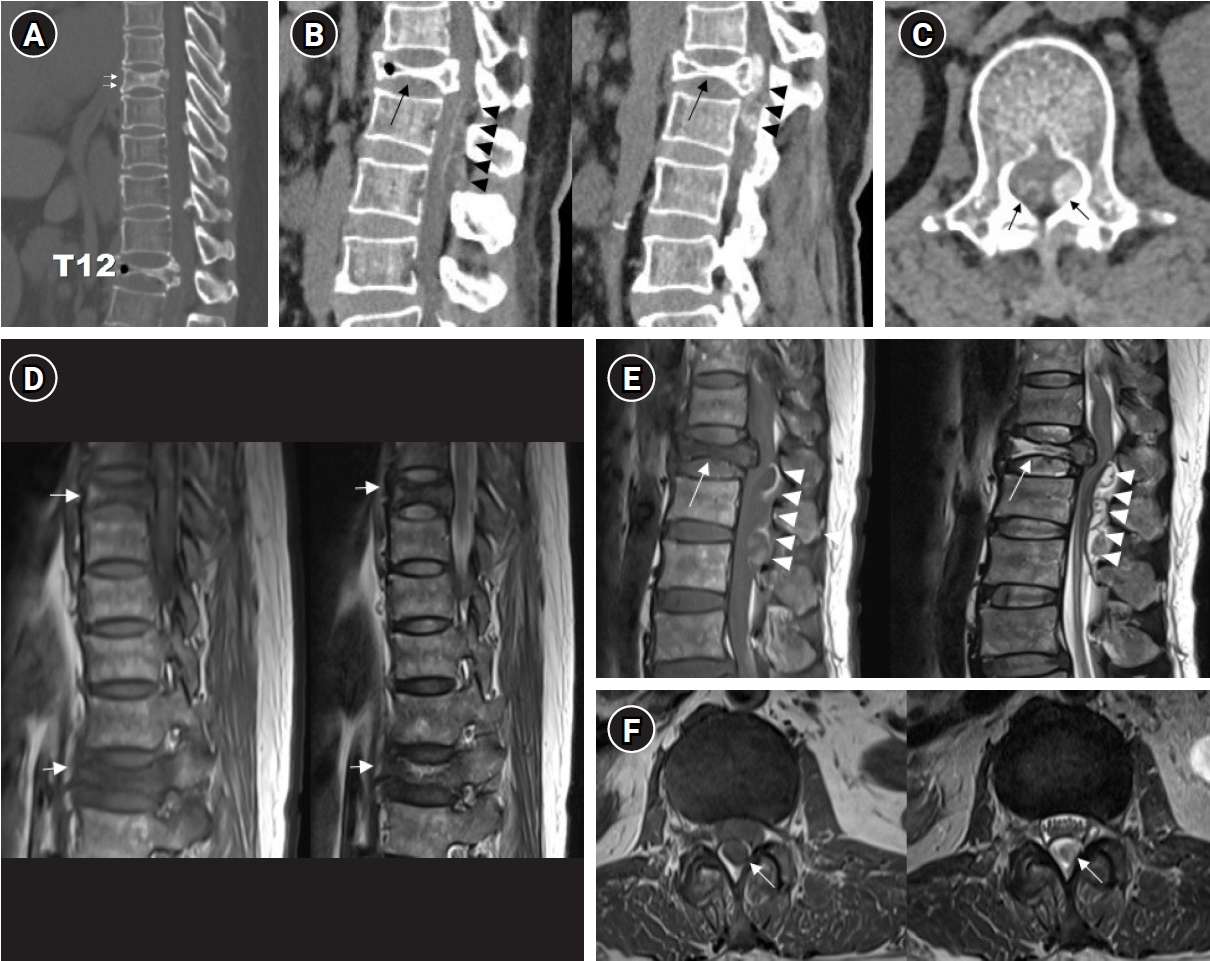
Spinal artery aneurysms are exceedingly rare, and their natural history remains poorly understood. Diagnosis can be challenging due to their small size and the difficulty in detection by MR angiography (MRA) or CT angiography (CTA); Digital Subtraction Angiography (DSA) is considered the gold standard diagnostic tool. This case report presents two cases of ruptured thoracic radicular artery aneurysms leading to subdural hematoma (SDH) and subarachnoid hemorrhage (SAH). The first patient, a 71-year-old female, presented with bilateral leg weakness, headache, and severe back pain, where multiple fusiform dilatations of the left T9 radiculopial artery were identified. She showed significant improvement after surgical intervention. The second patient, a 75-year-old female, presented with paraplegia and severe back pain, and a saccular dilatation in the right T10 radiculopial artery was found. She underwent endovascular embolization but showed no neurological improvement. These cases highlight the diverse clinical presentations, diagnostic challenges, and uncertainties in management strategies for ruptured spinal artery aneurysms, emphasizing the need for prompt intervention, especially in cases with significant or progressive neurological deficits.
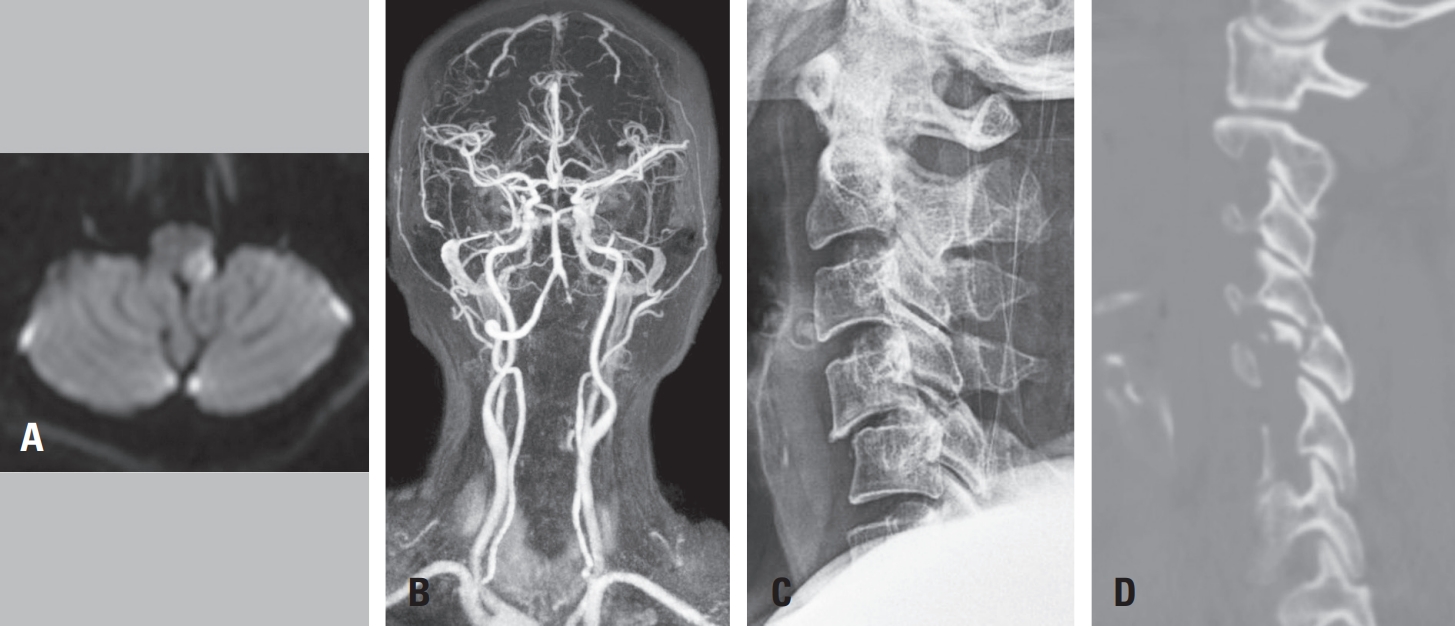
Purpose To report an uncommon case of Opalski syndrome following traumatic C4–C5 facet dislocation with vertebral artery dissection, and to discuss its diagnostic and therapeutic implications.
Materials and Methods A 60-year-old woman presented after a motor vehicle collision with bilateral upper limb weakness. Cervical X-ray, CT, MRI, and CT angiography revealed C4–C5 facet dislocation and left vertebral artery occlusion. Urgent anterior cervical discectomy and fusion were performed, and the postoperative course was monitored.
Results Immediate postoperative improvement to 4/5 strength in both arms was noted; however, new left facial numbness appeared at 12 hours and left lower limb weakness with gait ataxia at 48 hours. Brain MRI confirmed left lateral medullary infarction, and aspirin therapy was initiated. At one month, left arm strength recovered to 4/5, but ataxia persisted.
Conclusions In cervical trauma patients with C4–C5 facet dislocation and vertebral artery injury on initial imaging, the possibility of delayed lateral medullary infarction—particularly Opalski syndrome—should be considered. Prompt brainstem imaging and tailored antithrombotic therapy are essential when new neurologic deficits arise.
Study Design A retrospective comparative study.
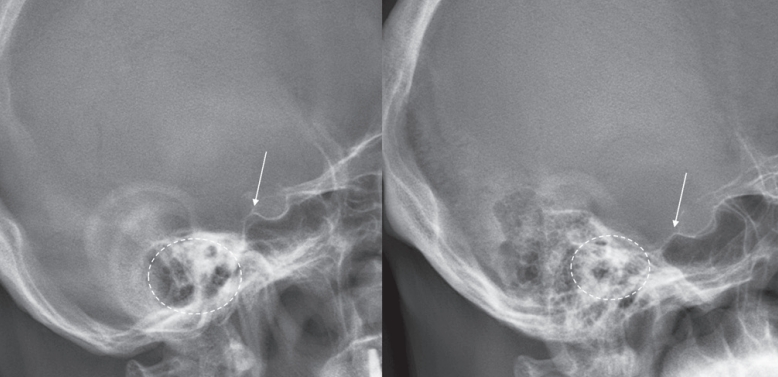
Purpose This study aimed to evaluate the reliability of the external auditory meatus (EAM) as a reference point for determining the cranial center in patients with sagittal spinal deformity. Specifically, we assessed the radiographic visibility and spatial relationship of the EAM relative to the midpoint of the nasion-inion line (MNI) and compared it with the sella turcica.
Overview of Literature: The cranial center is commonly defined as the midpoint of the nasion-inion line (MNI). The EAM has been widely used as an approximate surrogate of the MNI; however, its radiographic clarity and consistency are often limited. In contrast, the sella turcica is a singular anatomical structure that is more distinctly visualized on radiographic imaging.
Methods A total of 71 patients who underwent corrective surgery for spinal deformity between 2021 and 2024 were included. Preoperative full-spine radiographs were analyzed to evaluate the spatial relationship between both the EAM and the sella turcica relative to the MNI. Radiographic visibility was classified into three categories: single-point and clear, duplex but distinguishable, and unclear.
Results The EAM was located, on average, 1.1 mm posterior and 17.1 mm inferior to the MNI, whereas the sella turcica was located 13.8 mm anterior and 2.0 mm superior to the MNI. Relative to the femoral head axis, angular analysis revealed that the EAM exhibited a mean posterior tilt of 0.2°, while the sella turcica showed a mean anterior tilt of 1.3°. The sella turcica was clearly identifiable in 84.5% of cases, whereas the EAM was clearly visualized in only 14.1%, with the majority being either duplicated or indistinct (p<0.001).
Conclusions Although the EAM is anatomically closer to the MNI, its radiographic visibility and consistency are inferior to those of the sella turcica, thereby reducing its reliability as a cranial reference point. Further studies are needed to determine whether the sella turcica can serve as a more reliable alternative reference.
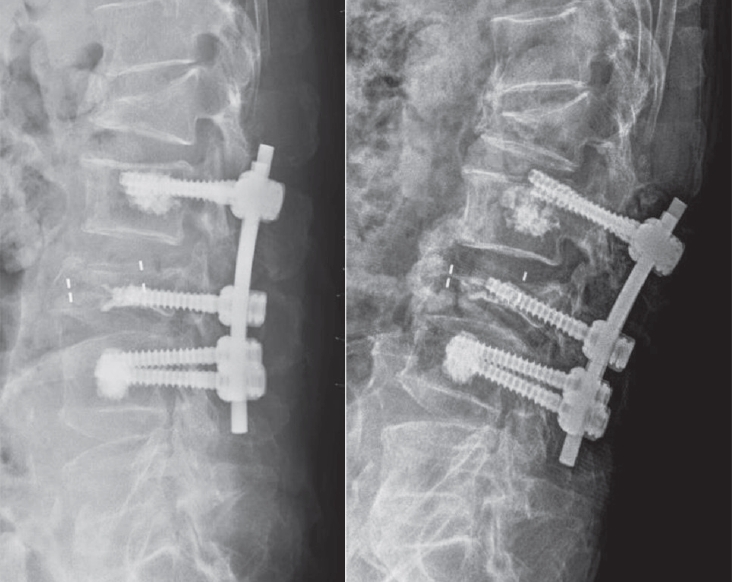
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
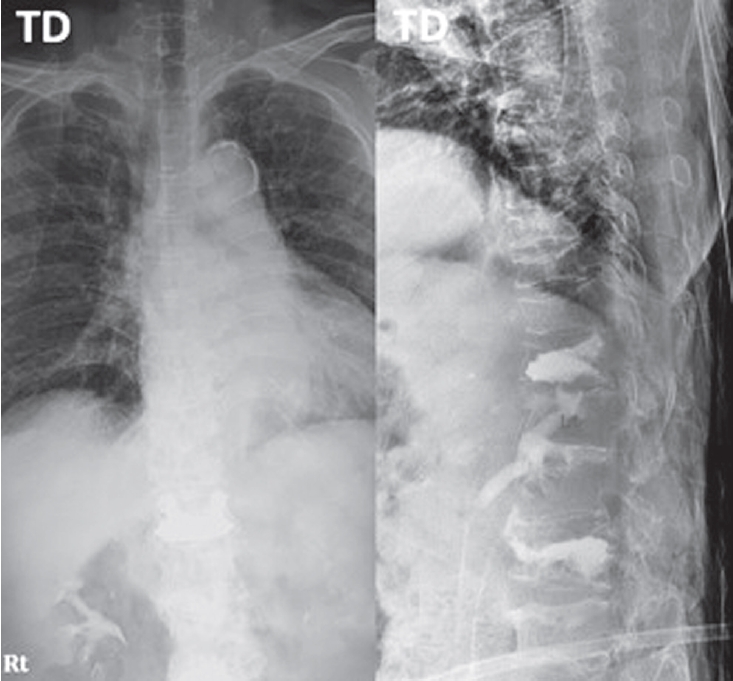
Purpose To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
Methods An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
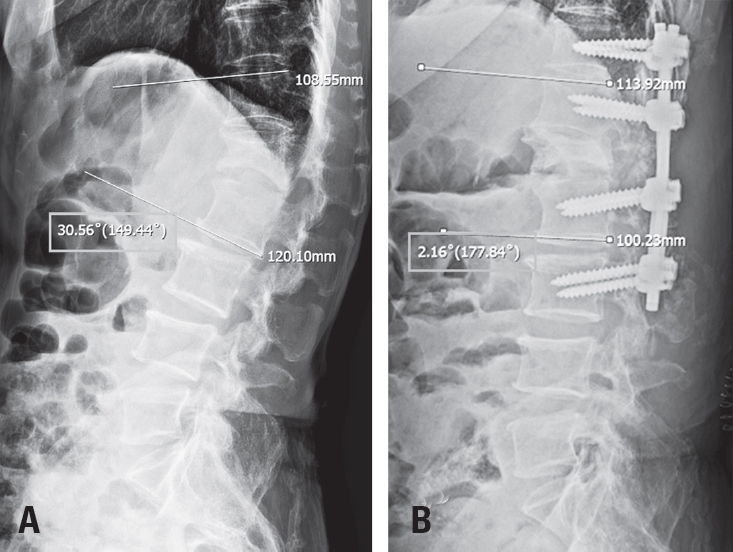
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Vertebroplasty or kyphoplasty is a widely accepted minimally invasive procedure for treating painful vertebral compression fractures. Although considered safe, rare but serious complications such as spinal subdural hematoma (SDH) can occur, particularly in patients receiving long-term anticoagulation therapy. We present a rare case of spinal SDH following kyphoplasty in a 78-year-old woman with a mechanical aortic valve on chronic warfarin therapy. Anticoagulation was managed perioperatively with warfarin discontinuation and bridging enoxaparin. Postoperative X-ray showed subtle posterior cement leakage. MRI on postoperative day 1 revealed lumbar SDH, which progressed cranially by day 2. The patient remained neurologically intact and was treated conservatively with corticosteroids and temporary suspension of anticoagulation. Follow-up imaging showed gradual hematoma resolution, and she was discharged without deficits. This case suggests the importance of maintaining a high index of suspicion for spinal hematoma in anticoagulated patients, especially when new symptoms or even minor cement leakage are present. Careful perioperative planning, including early imaging and multidisciplinary management, is crucial in such high-risk patients.
Primary glioblastoma of the spinal cord is a rare and aggressive tumor, comprising less than 1.5% of spinal neoplasms. It typically affects young adult males and arises in the cervical or thoracic regions. We report an unusual case of intradural extramedullary spinal glioblastoma in a 62-year-old man with prior lymphoma in remission. The patient presented with a 7-month history of progressive lower limb weakness, numbness, and radiating pain. MRI revealed a contrast-enhancing mass at the T6–7 level, initially suspected as lymphoma. Surgical resection via total laminectomy was performed, and en-bloc tumor removal achieved. Histopathological analysis confirmed WHO grade IV glioblastoma, IDH-wildtype, without Histone H3 mutation. This case highlights an atypical radiologic and anatomical presentation, complicating preoperative diagnosis. Histopathologic and molecular studies were essential for confirmation. Postoperative treatment included adjuvant radiotherapy and temozolomide, though their efficacy remains uncertain in spinal glioblastoma due to limited evidence and spinal cord radiosensitivity. Early biopsy and a multimodal diagnostic approach are critical for managing rare spinal tumors presenting with nonspecific clinical and imaging features.
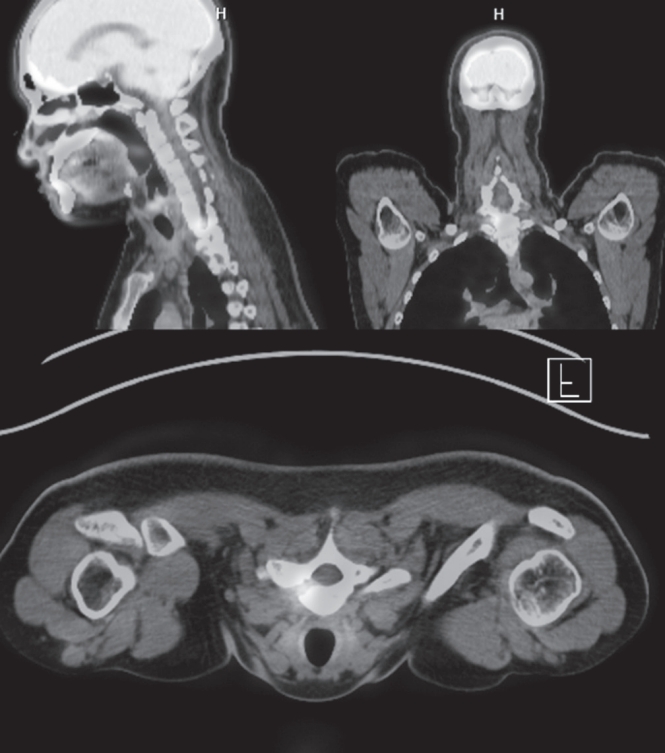
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
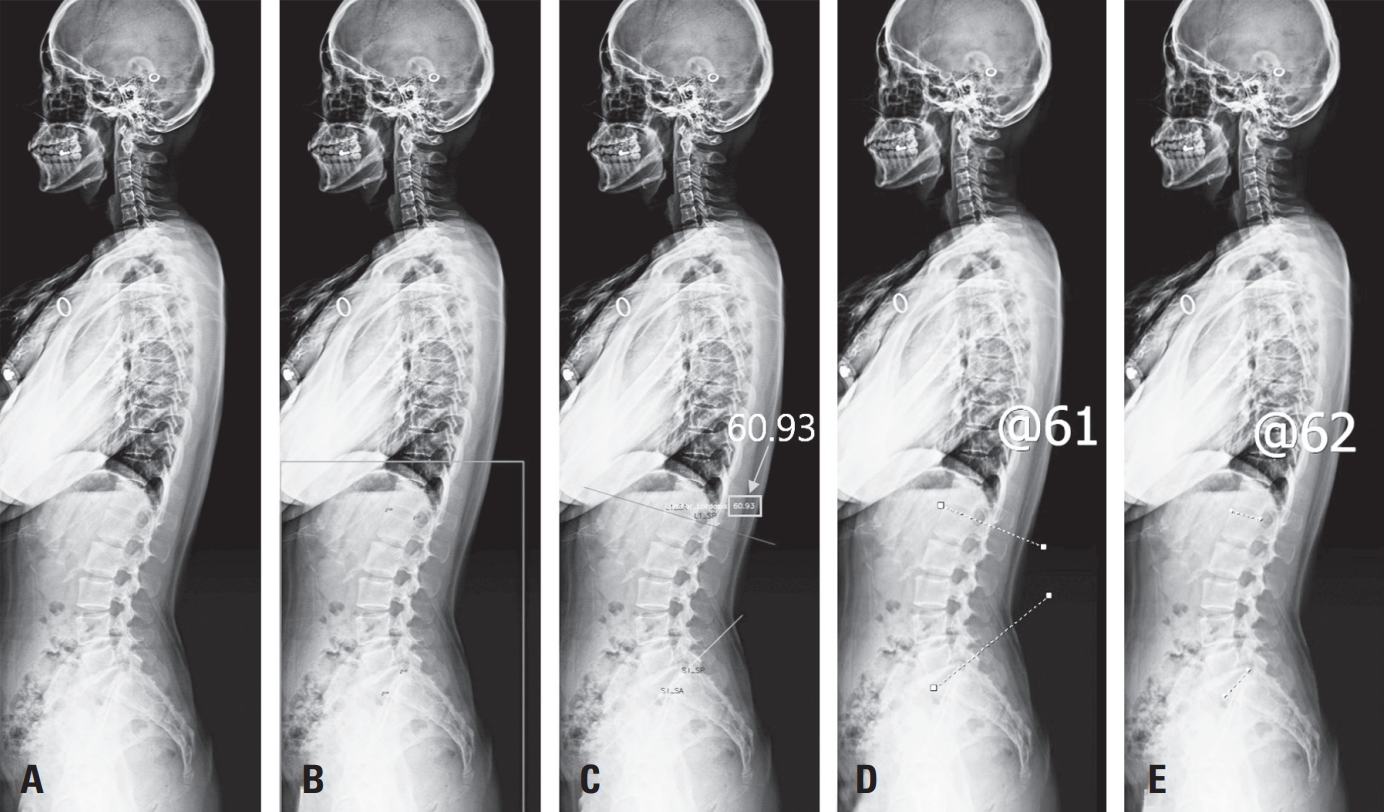
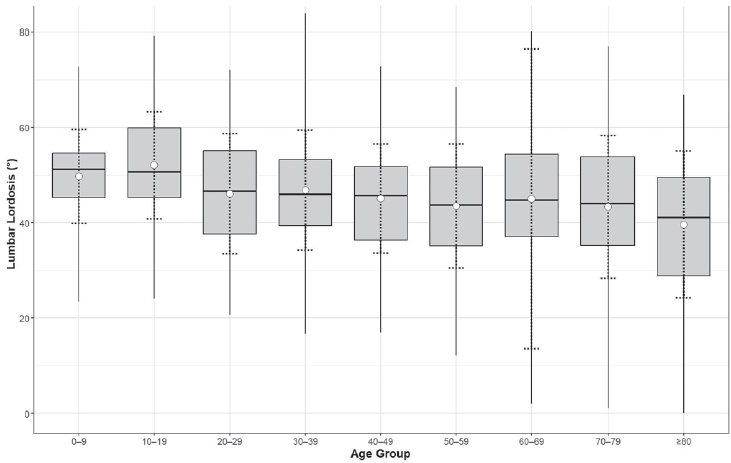
Purpose To evaluate the association between lumbar lordosis and age using an AI-based automated measurement model applied to a large dataset of standing lateral spinal radiographs.
Materials and Methods This retrospective study analyzed 904 high-quality radiographs selected from 2,397 images acquired between 2019 and 2021. Lumbar lordosis was defined as the angle between the superior endplates of L1 and S1 and automatically measured using a validated deep learning model. Subjects were categorized into nine age groups. One-way ANOVA compared lumbar lordosis across age groups, and Pearson correlation assessed the relationship between age and lumbar lordosis.
Results Lumbar lordosis ranged from 0° to 84° (mean 45.9°±13.4°). The highest mean value was in the 10–19-year group (52.1°), and the lowest in the ≥80-year group (39.6°). Minimum values decreased to 0° in individuals aged ≥60 years. No significant differences were found across age groups (p=0.561). A weak but significant negative correlation was observed between age and lumbar lordosis (r=–0.247, p<0.0001).
Conclusions AI-based automated measurement enabled efficient large-scale analysis and revealed a wide distribution of lumbar lordosis with a gradual age-related decline. These findings highlight the value of AI in spinal alignment assessment.
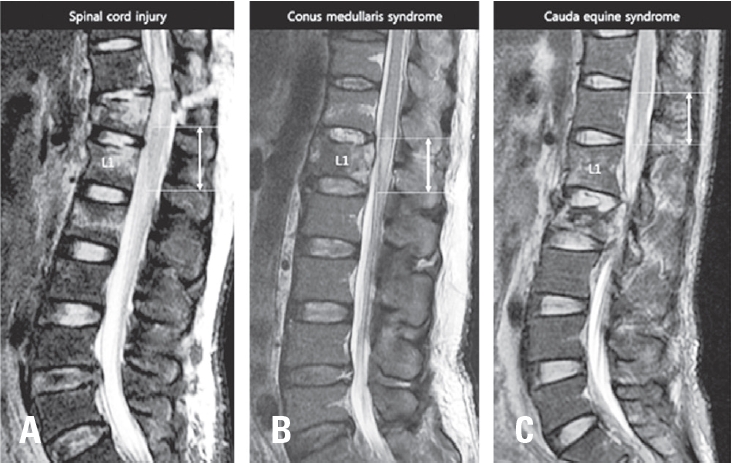
Background Neurogenic bladder dysfunction is a common and serious consequence of traumatic conus medullaris syndrome (T-CMS). Despite its clinical importance, predictive data for bladder outcomes after T-CMS remain limited. This study aimed to identify predictors of neurogenic bladder dysfunction at ≥2 years post-injury.
Methods We retrospectively reviewed 39 patients with acute T-CMS treated at a single level I trauma center from 2004–2017 who underwent spinal surgery and had ≥2 years of follow-up. Bladder function at 2 years was categorized as complete dysfunction, incomplete dysfunction, or normal. Potential predictors included demographic factors, injury mechanisms, ASIA Impairment Scale grades, MRI timing, fracture level and type, canal diameter, occupying ratio, conus signal change (normal, edema, or edema with hemorrhage), edema length, time to surgery, and surgical approach. Univariate and multivariate analyses were performed.
Results At final follow-up, 14 patients (35.9%) had complete bladder dysfunction, 12 (30.8%) had incomplete dysfunction, and 13 (33.3%) had normal function. Multivariate analysis identified edema with hemorrhage in the conus medullaris as the only independent predictor of bladder dysfunction.
Conclusions Bladder dysfunction is highly prevalent after T-CMS. Hemorrhagic edema in the conus medullaris significantly increases the risk of long-term neurogenic bladder dysfunction.
Purpose The impact of skeletal muscle mass and bone mineral density (BMD) on frailty after osteoporotic vertebral fractures (OVFs) remains unclear. This study aimed to assess the interplay between frailty, skeletal muscle mass, and bone mineral density in OVFs.
Materials and Methods A total of 66 patients with osteoporotic vertebral compression fractures were enrolled. We collected clinical and radiological data, including age, body mass index (BMI), frailty index, and parameters such as lumbar lordosis, thoracic kyphosis, skeletal muscle mass, and BMD. We then analyzed the relationships between frailty and these variables.
Results The mean age, BMI, BMD T-score, skeletal muscle mass, and frailty index were 78.0±7.8 years, 22.3±3.3 kg/ m², -3.59±0.96, 37.84±6.24 kg, and 2.59±1.08, respectively. Of the 66 patients, 14 (21.1%) were frail prior to fracture, while 37 (56.1%) were frail after fracture, indicating a worsening frailty status. Specifically, 23 patients (34.8%) transitioned from pre-frail to frail following their fracture and had both lower BMD (T-score: -3.7±0.93) and lower skeletal muscle mass (35.74±3.83 kg). Frailty was negatively correlated with BMD (r=-0.28, p=0.02), while BMD was positively correlated with skeletal muscle mass (r=0.29, p=0.02). OVFs were positively correlated with frailty (r=0.33, p=0.01), especially in terms of fatigue (r=0.31, p=0.01) and ambulation (r=0.21, p=0.01).
Conclusions In patients with osteoporotic vertebral fractures, decreased muscle mass and low BMD appear to exacerbate frailty. Furthermore, frailty may be both a contributing and a resulting factor in the development of osteoporotic vertebral fractures.
Objective To investigate the utility of a deep learning model in diagnosing traumatic lumbar fractures on computed tomography (CT) images.
Summary of Background Data: CT scans are widely used as the first choice for detecting spinal fractures in patients with severe trauma. Although CT scans have high diagnostic accuracy, fractures can occasionally be missed.
Recently, deep learning has been applied in various fields of medical imaging.
Methods CT images from 480 patients (3695 vertebrae) who visited a level-one trauma center with lumbar fractures were retrospectively analyzed. The diagnostic results were confirmed by two experienced musculoskeletal radiologists and one experienced spine surgeon using magnetic resonance imaging (MRI). Deep learning networks were employed for diagnosis, with 425 cases used for training and 55 cases for testing. Sensitivity, specificity, accuracy, and the area under the receiver operating characteristic curve (AUROC) were calculated to evaluate diagnostic performance.
Results The model successfully identified 107 out of 129 vertebrae with fractures, achieving a sensitivity of 82.95%, a specificity of 93.24%, an AUROC of 0.936, and an overall accuracy of 88.45%.
Conclusions This study demonstrated that the deep learning model showed high accuracy in diagnosing traumatic lumbar fractures. This approach has the potential to assist spine specialists, radiologists, and trauma care experts.
Further validation is needed to determine its effectiveness in clinical settings.
Tethered cord syndrome (TCS) is a condition in which the spinal cord becomes pathologically stretched due to various congenital or acquired etiologies, leading to progressive neurological symptoms. While surgical detethering is the gold standard for pediatric patients, adult-onset recurrent TCS presents a significant surgical challenge. Reoperation carries substantial risks—including spinal cord injury, cerebrospinal fluid leakage, and a high rate of retethering—often resulting in suboptimal long-term outcomes. Recently, spine-shortening osteotomy (SSO) has emerged as an alternative technique to reduce spinal cord tension without direct manipulation of the neural elements. Here, we report a case of recurrent adult TCS associated with a lipomyelomeningocele, which was exacerbated by post-traumatic kyphosis from an L1 compression fracture. The patient was successfully treated with SSO at the L1 level. This case highlights the utility of SSO as a safe and effective alternative to conventional revision detethering, particularly in complex cases involving spinal deformity.
Advanced imaging technologies have revolutionized the diagnosis and management of spinal pathologies by providing superior precision and efficiency. Modalities such as PET-CT, SPECT, diffusion tensor imaging (DTI), and magnetic resonance spectroscopy (MRS) offer unique insights into the metabolic, structural, and functional aspects of spinal diseases, enabling better differentiation of lesions, improved surgical planning, and early detection of pathological changes. Furthermore, the integration of artificial intelligence (AI) has enhanced imaging workflows by enabling automated analysis, prediction of clinical outcomes, and segmentation of spinal structures. Despite these advancements, challenges such as technical limitations, high costs, and ethical concerns, including issues of data privacy and AI-generated inaccuracies, hinder widespread adoption. This review explores the clinical applications, limitations, and future directions of these emerging technologies, highlighting the need for multidisciplinary collaboration and large-scale research to standardize protocols and optimize patient outcomes. The seamless integration of advanced imaging and AI represents a transformative potential for improving diagnostic accuracy and treatment efficacy in spinal care.
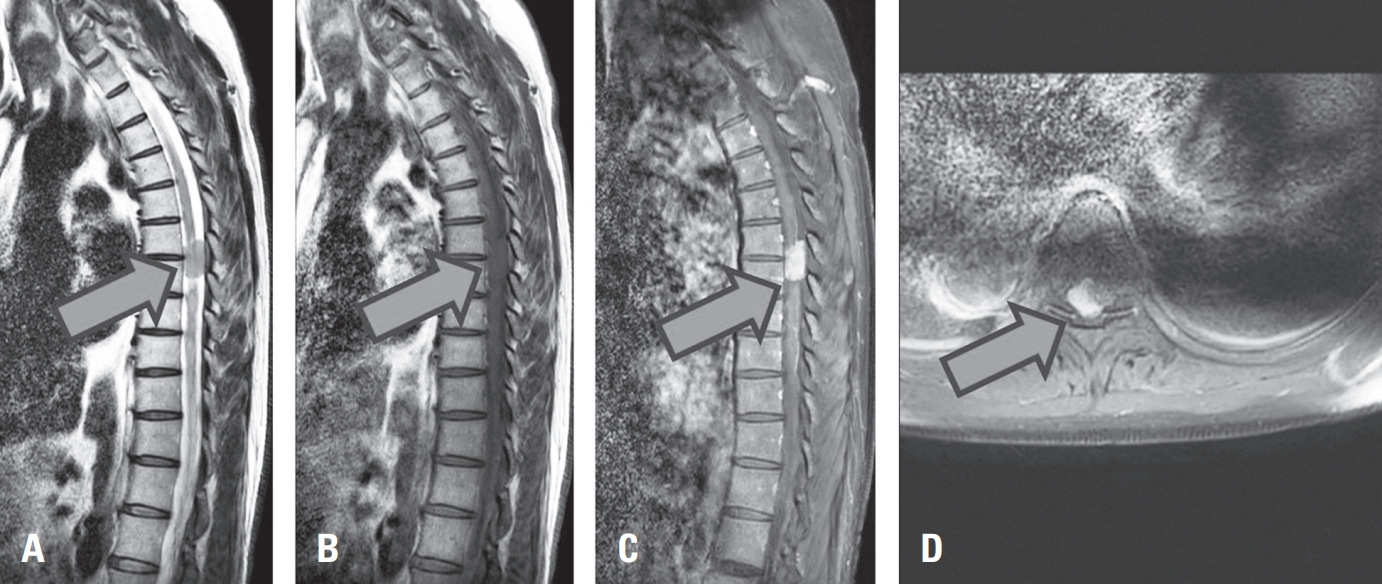
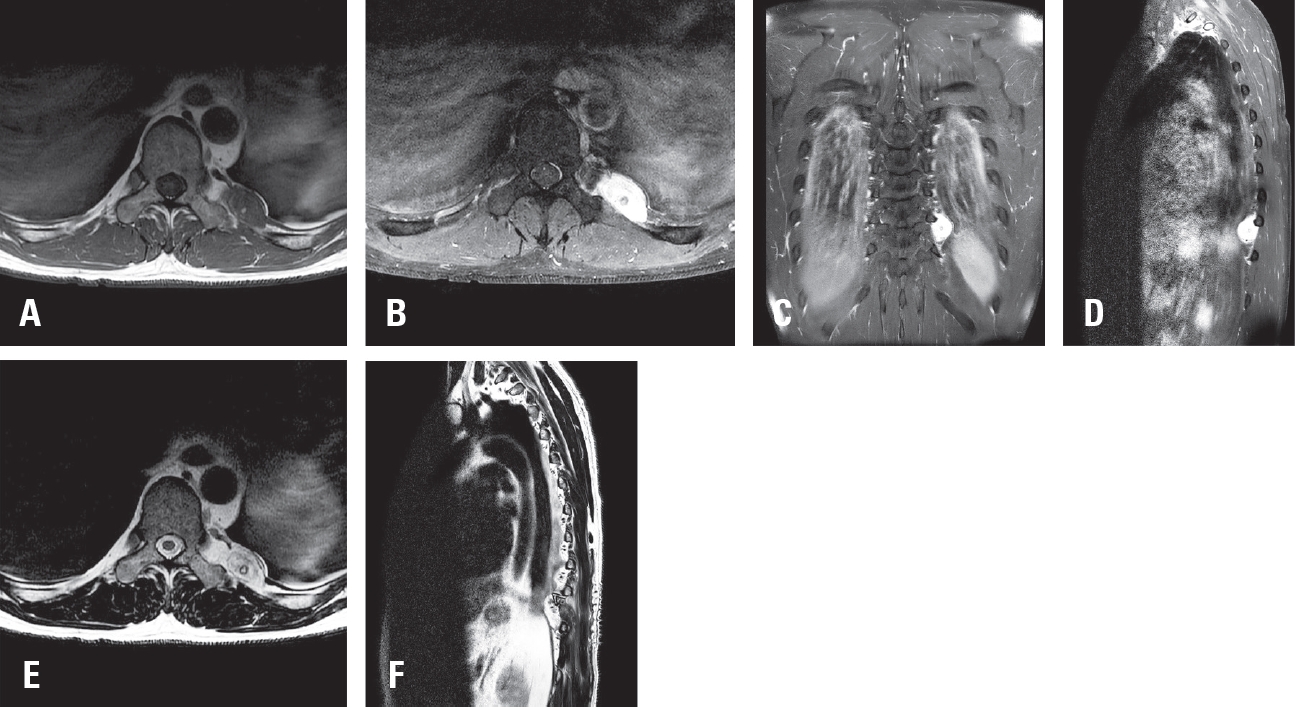
Purpose Glomangiomas of the spine are exceptionally rare benign vascular tumors, frequently misdiagnosed as more common lesions such as schwannomas or meningiomas. Although most spinal glomangiomas exhibit benign behavior, the presence of a BRAF V600E mutations may indicate uncertain malignant potential. Accurate diagnosis and complete surgical excision are essential for favorable outcomes.
Methods A 43-year-old male with left flank pain was evaluated with thoracic MRI and underwent surgical resection. Histopathological and molecular analyses were performed.
Results Thoracic magnetic resonance imaging (MRI) revealed a 2.8 cm ovoid, hypervascular mass adjacent to left T10 transverse process, extending to the posterior hemithorax. Surgical resection was performed, and histopathological examination confirmed a glomangioma with positive smooth muscle actin (SMA) expression and a BRAF V600E mutation.
Conclusions This case highlights the diagnostic challenge posed by paraspinal glomangiomas and emphasizes the importance of histopathological and molecular analysis in establishing the correct diagnosis. A review of the literature demonstrates that complete surgical excision remains the treatment of choice, with excellent prognosis. The identification of BRAF mutations may warrant closer follow up.
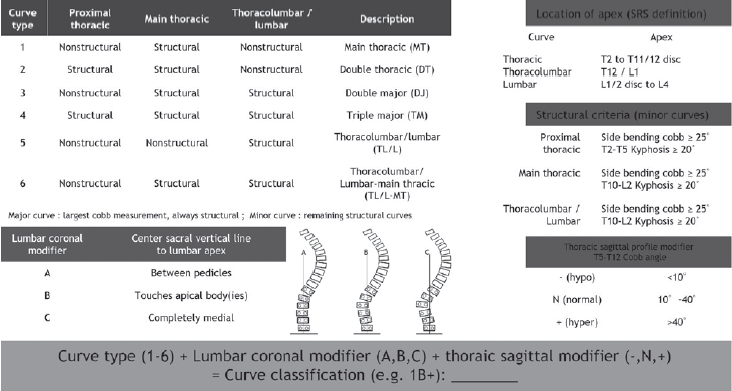
Adolescent idiopathic scoliosis refers to spinal deformity that develops from just before the onset of puberty until the completion of skeletal growth, and the primary goal of treatment is to achieve a well-balanced spine. In the late 1990s, advances in the anatomical understanding of the spine and the development of fixation instruments made posterior pedicle screw insertion feasible, thereby enabling the transmission of powerful corrective forces for deformity correction. Over the subsequent decades, accumulated clinical experience and outcomes have provided a deeper understanding of scoliotic curves and led to the establishment of effective principles for determining the extent of spinal fusion. However, these treatment principles are based on the unique biomechanics and procedural characteristics of scoliosis correction surgery, which can make them difficult to understand without sufficient explanation. In this review, we aim to describe these established treatment principles and surgical processes in detail using schematic illustrations and images. Although these principles will continue to undergo new challenges and validation over time, they will remain a meaningful reference point for those exploring alternative strategies.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Object: This pilot study aimed to evaluate the effectiveness of cervical epidural block (CEB) in improving upper extremity muscle strength in individuals diagnosed with cervical disc herniation.
Materials and Methods 5 patients diagnosed with cervical disc herniation were included and underwent a single CEB treatment. Patients were monitored weekly for 2 weeks via an outpatient clinic. Hand grip strength of affected side and difference of hand grip strength between affected and unaffected side (DHGS) was recorded using dynamometers; before treatment, immediate after treatment, after 1week and 2weeks of treatment. Pain on neck and radiating pain to upper extremity (UE) were measured using the visual analogue scale (VAS) before treatment and 2weeks after treatment.
Results The median age of the patients was 48 (37.0-78.0) years, and the affected disc levels were C5-6 (3 patients), C6-7 (1 patient), and C5-6-7 (1 patient) respectively. In terms of pain, VAS of neck decreased from 6.8 to 3.2, and VAS of UE decreased from 7.4 to 3.0. Both hand grip strength of affected side and DHGS showed improvement when comparing before and after treatment (immediate, 1 week and 2 weeks after treatment) (p<0.001). However, there was no difference between immediate, 1 week and 2 weeks after treatment. The result was same for adjusting age and sex as covariates (p<0.001).
Conclusions These findings suggest that CEB has the potential in improving pain and UE muscle weakness associated with cervical disc herniation. Further large-scale studies are necessary to validate these preliminary outcomes and establish the long-term effectiveness and sustainability of CEB in managing cervical disc herniation.
Purpose This study was conducted to identify risk factors predicting the loss of cervical lordosis (LCL) in patients with multilevel ossification of the posterior longitudinal ligament (OPLL) following laminoplasty.
Material and Methods: We conducted a retrospective analysis of data from patients who underwent laminoplasty at Chonnam National University Hospital between January 2013 and December 2022. Various radiological parameters and clinical outcome measures were collected perioperatively. Patients were divided into 2 groups according to the severity of LCL. We examined preoperative radiological parameters associated with LCL.
Results We analyzed data from 109 patients (92 men and 17 women; mean age, 60.31±10.80 years). A higher T1 slope (odds ratio [OR], 1.420; p<0.001) and a lower extension ratio (OR, 0.883; p=0.019) were associated with a higher risk of LCL. T1 slope was shown to be an excellent predictor of LCL, with a cut-off value of 28° (p<0.001, area under the curve=0.918). Also, The T1 slope and extension ratio were statistically significant correlated with clinical outcomes.
Conclusions T1 slope and extension ratio were significantly associated with LCL in patients with multilevel OPLL following laminoplasty. The cut-off value for the T1 slope was 28°, and the cut-off value for the extension ratio was 33. Therefore, in multilevel OPLL patients with a T1 slope exceeding 28° or an extension ratio below 33, a warning regarding the potential LCL should be given before performing cervical laminoplasty.
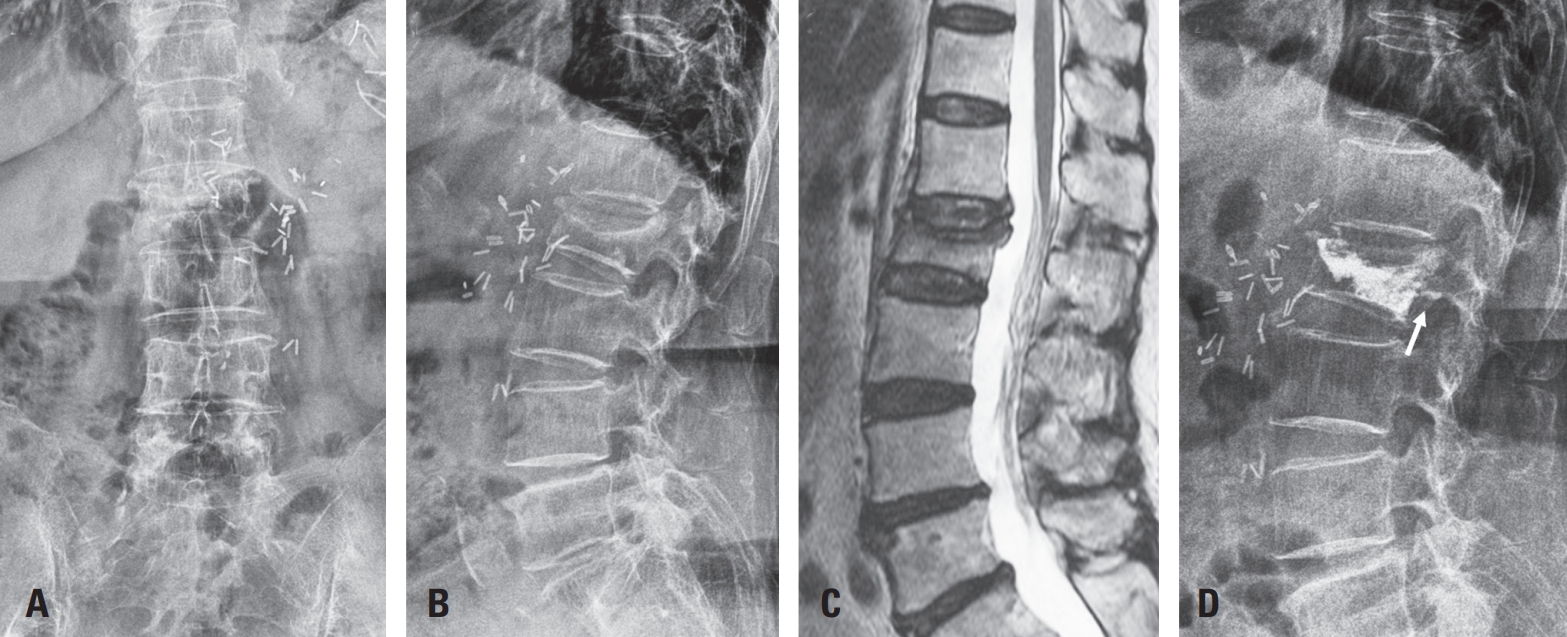
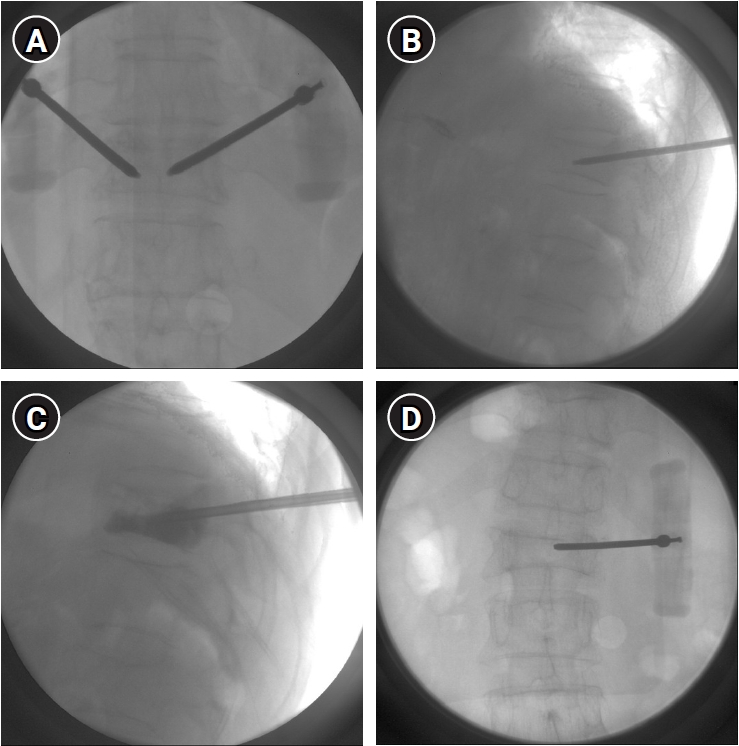
Purpose This study aimed to evaluate whether percutaneous vertebroplasty (PVP) contributes to vertebral height restoration and sagittal alignment correction in osteoporotic vertebral compression fractures (OVCF), focusing on thoracolumbar junction fractures.
Methods A retrospective review of 40 patients with single-level OVCF at T10–L2 treated with PVP was performed. Vertebral heights (anterior, middle, and posterior) and sagittal alignment (thoracic kyphosis, lumbar lordosis, sagittal vertical axis, and segmental Cobb's angle) were measured preoperatively, at 3 months, and at 6 months. Clinical outcomes included visual analog scale and EuroQol-5 Dimensions.
Results Significant pain relief and improvement in quality of life were observed at 6 months postoperatively. Vertebral height restoration, particularly in the anterior and middle portions, was noted at 3 months; however, partial loss of the restored height occurred by 6 months. Most sagittal alignment parameters showed no significant postoperative change, although lumbar lordosis significantly increased, resulting in a reduced pelvic incidence–lumbar lordosis mismatch.
Conclusion PVP provides meaningful clinical improvement in thoracolumbar OVCFs and offers early vertebral height restoration; however, this radiologic benefit is not sustained over time. While limited improvement in lumbar lordosis was observed, PVP does not substantially correct global sagittal alignment. These findings suggest that PVP should be considered primarily a pain-relieving and stabilizing procedure rather than a deformity-correcting intervention.
Chondroma is a benign cartilaginous neoplasm, rarely encountered in the lumbar spine. We report a case involving a 70-year-old female who presented with lower limb radiating pain that started four years ago. Although no pronounced muscle weakness was noted, the patient experienced progressively worsening radiating pain in the L4 dermatome. Initial evaluation, including magnetic resonance imaging (MRI) performed at another medical facility, suggested a potential lesion associated with left L4–5 lumbar disc herniation. Despite non-surgical interventions, the patient experienced limited symptomatic relief, prompting her to seek further care at our clinic. Subsequent contrast-enhanced MRI conducted at our facility revealed a mass exhibiting peripheral rim enhancement surrounding the L4 nerve root. Suspecting a neurogenic tumor, we decided to perform surgical excision of the mass. Postsurgery, histopathological analysis confirmed the presence of hyaline cartilage with lobular architecture and chondrocytes in lacunae, leading to the conclusive diagnosis of chondroma. Following the surgical procedure, the previously reported radiating pain exhibited notable improvement.
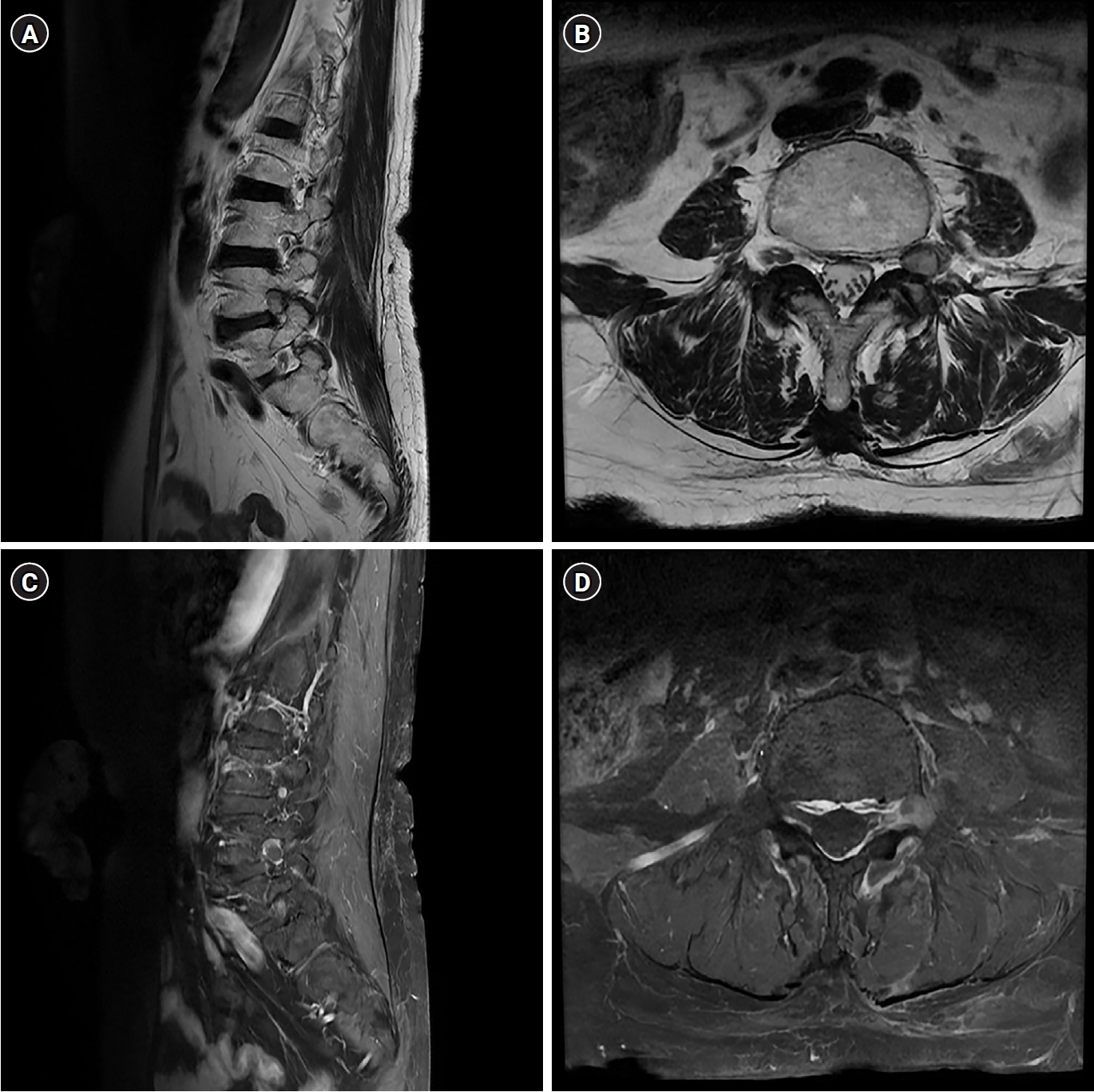
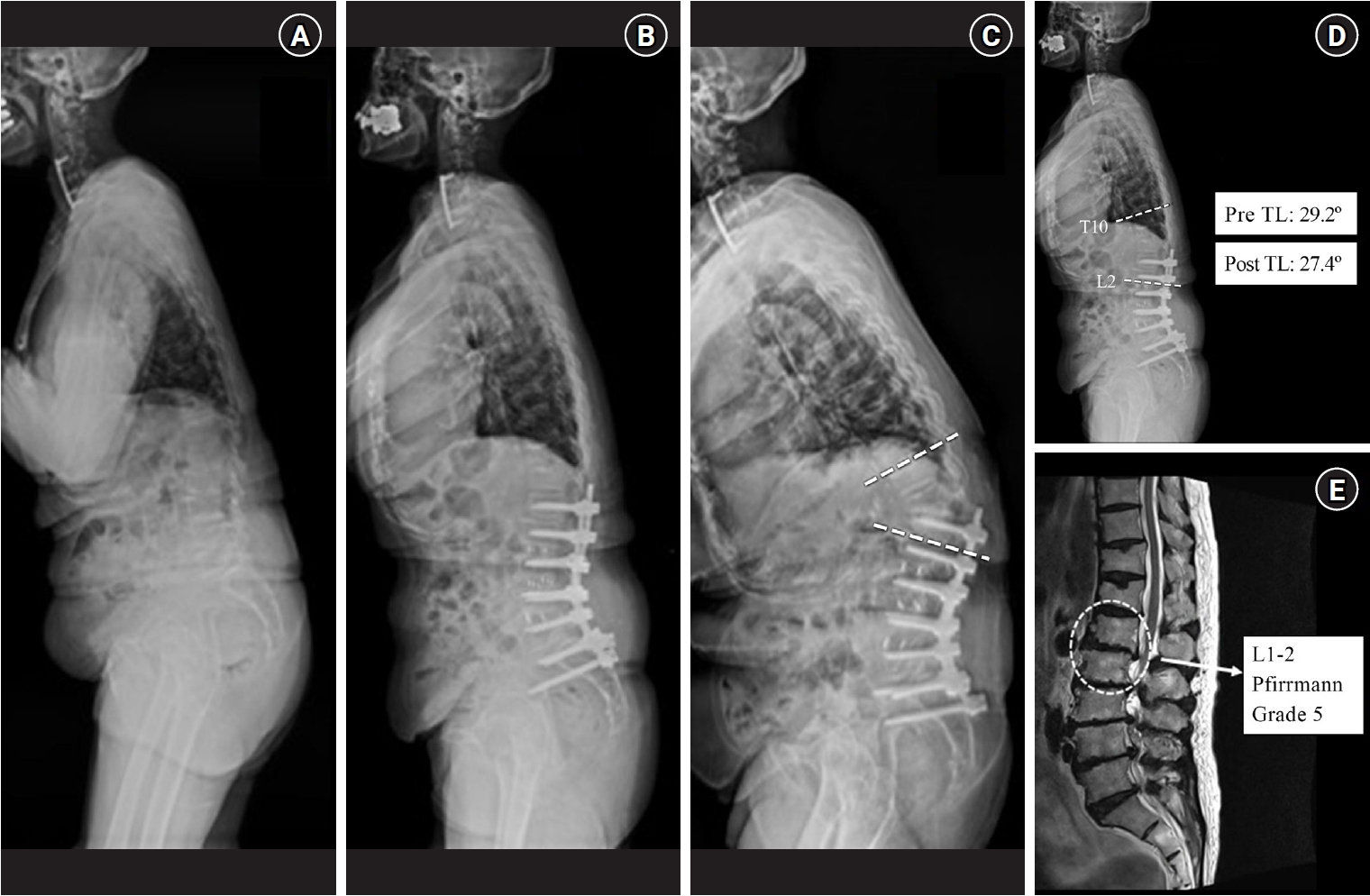
Purpose This retrospective study investigated the distinct clinical and radiographic drivers of early- versus late-onset proximal junctional kyphosis (PJK) following multilevel thoracolumbar (TL) fusion.
Methods After applying the exclusion criteria (spinal infection, neuromuscular disease, age <50 years), the analysis included 136 patients who underwent ≥4-level TL fusion and were followed up for a minimum of 2 years. PJK was classified as early (≤6 months) or late (>6 months) onset. Patient-related factors, surgical variables, sagittal spinopelvic parameters, and preoperative magnetic resonance imaging findings were analyzed using multivariate logistic regression to identify independent predictors of early PJK.
Results Among 24 patients (17.6%) who developed PJK, the early and late-onset groups included 13 and 11 patients, respectively. The early PJK group exhibited significantly greater preoperative and postoperative TL angles compared with the late group (preoperative: 23.03±13.83° vs. 9.67±9.67°, p=0.024; postoperative: 19.6±6.95° vs. 6.95±6.35°, p<0.001). The Pfirrmann grade of the L1–2 intervertebral disc was significantly higher in the early PJK group (3.92±0.95 vs. 2.81±0.60, p=0.006). No surgical variables differed significantly between the groups. Multivariate analysis confirmed greater postoperative TL angle and more advanced L1–2 disc degeneration as independent predictors of early PJK.
Conclusion Early-onset PJK following multilevel TL fusion is primarily driven by regional biomechanical vulnerabilities, specifically residual postoperative TL kyphosis and advanced adjacent L1–2 disc degeneration, rather than by surgical variables. Meticulous evaluation of regional TL alignment and adjacent disc health during surgical planning is critical for risk stratification and prevention of early junctional failure.
Study Design The study was designed as a retrospective clinical study.
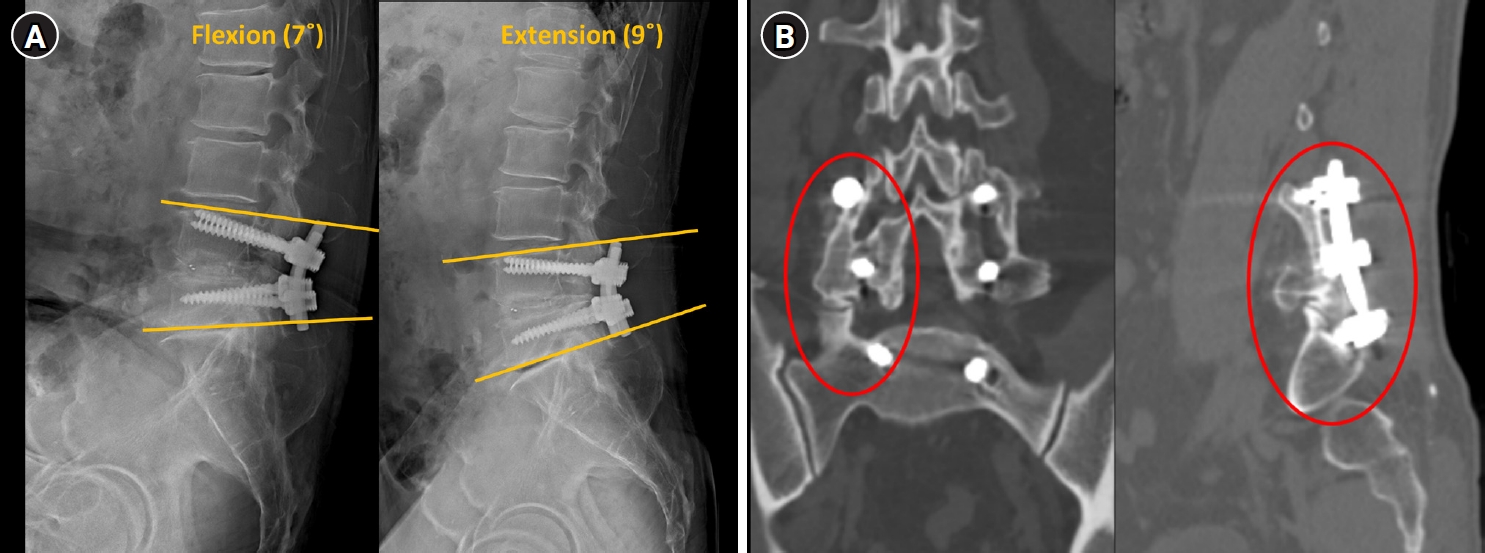
Purpose This study aimed to demonstrate that solid fusion and favorable outcomes can be achieved even without fusion extension through the application of an allograft bone chip insertion technique.
Overview of Literature: Screw loosening and nonunion are common complications following lumbar posterior fixation, often resulting from fusion failure. The optimal surgical strategy remains controversial, and most surgeons prefer extending fusion levels above or below the affected segment.
Methods Twelve patients who underwent revision surgery for screw loosening and nonunion by a single surgeon were retrospectively analyzed. Allograft bone chips were inserted into loosened screw holes to enhance fixation and promote fusion. Radiologic outcomes were evaluated at 1 year using dynamic flexion–extension X-ray and computed tomography (CT). Solid fusion was defined as ≤3° of motion on X-ray and, in eight patients with CT, as a continuous trabecular bone bridge. Clinical outcomes were assessed using the numerical rating scale (NRS) for back and leg pain and the Oswestry Disability Index (ODI).
Results From January 2020 to February 2022, 12 patients (7 men, 5 women; mean age, 65.8 years) underwent surgery. Eight were treated without fusion extension, three required one-level extension for adjacent segmental disease, and one for deformity correction. At 1 year, all patients achieved solid fusion with ≤3° motion, and CT confirmed a trabecular bone bridge in eight cases. Mean NRS scores for back and leg pain improved by 6.9 and 5.1 points, respectively, and ODI showed marked functional recovery.
Conclusion The allograft bone chip insertion technique appears to be a practical revision option for managing screw loosening and nonunion in selected patients. It can achieve solid fusion and favorable outcomes without fusion extension, thereby minimizing surgical morbidity and preserving motion segments.
Study Design This study was a retrospective single-center cohort study.
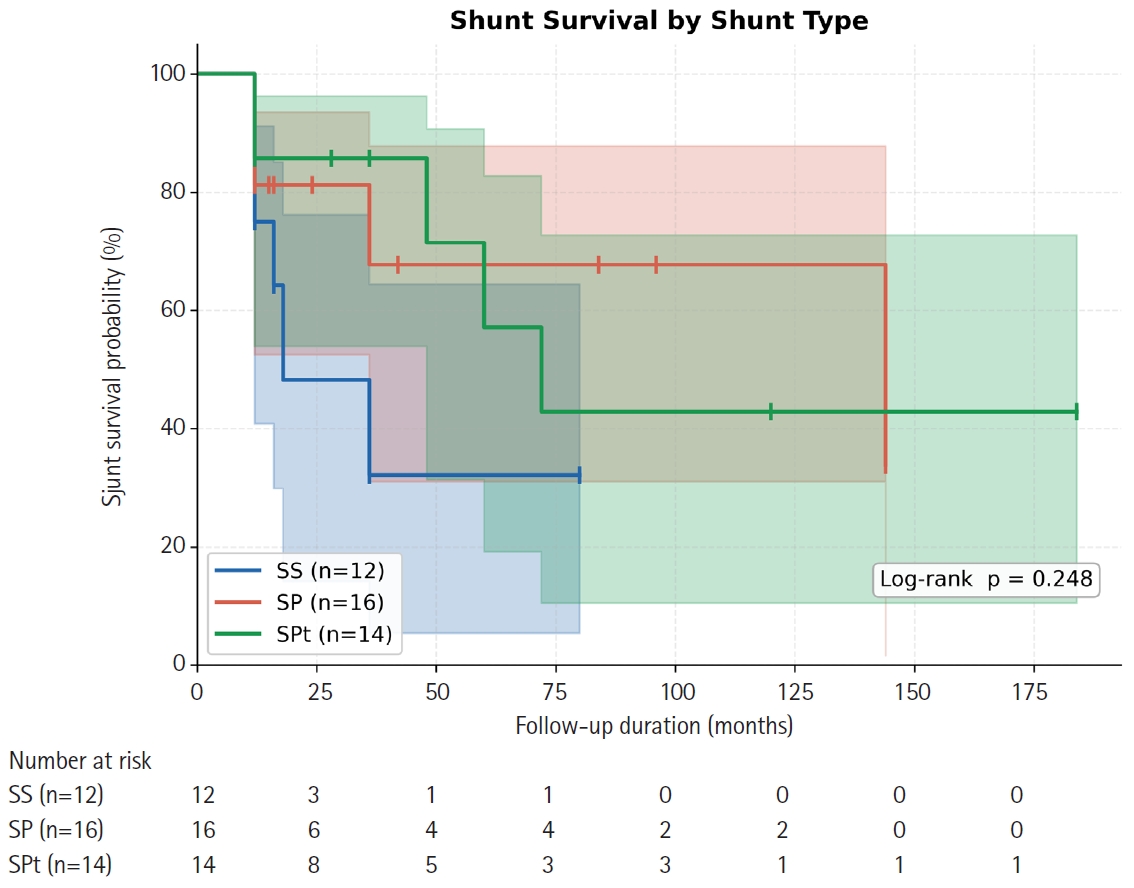
Purpose This study aimed to compare long-term shunt patency by shunt type (syringo-subarachnoid [SS], syringo-pleural [SP], syringo-peritoneal [SPt]) and disease etiology (post-traumatic, post-infectious, idiopathic) in patients surgically treated for syringomyelia, using Kaplan-Meier survival methodology.
Overview of Literature: Syringomyelia shunting carries a well-documented revision burden, but direct comparative survival data across shunt modalities and etiologic subgroups are scarce, particularly from East Asian centers.
Methods We retrospectively analyzed 42 patients (mean age, 47.6±11.8 years; 57.1% male) who underwent syringomyelia shunting at a tertiary neurosurgical center (January 2000–December 2020) with ≥12 months follow-up. Shunt type was classified as SS (n=12), SP (n=16), or SPt (n=14); etiology as post-traumatic (n=24), post-infectious (n=10), idiopathic (n=6), or hemorrhage/tumor-related (n=2). The primary endpoint was shunt revision surgery. Kaplan-Meier analysis, log-rank testing, and Cox proportional hazards regression were performed.
Results Over a median follow-up of 15 months (range, 12 to 184 months), 16 patients (38.1%) underwent shunt revision. Overall 12- and 24-month patency rates were 79.6% and 72.5%, respectively (median shunt survival 72 months). By shunt type, 12-month patency was 75.0% (SS), 81.3% (SP), and 85.7% (SPt); 24-month patency declined to 48.2% for SS while SP and SPt remained at 81.3% and 85.7% (log-rank p=0.248). Post-infectious syringomyelia showed the shortest median shunt survival (36 months) compared with post-traumatic (not reached) and idiopathic (not reached) groups (log-rank p=0.232). No independent predictor of shunt failure was identified on multivariate Cox regression.
Conclusion All three shunting techniques achieve approximately 80% one-year patency. SS may carry a higher long-term occlusion risk. Post-infectious syringomyelia requires closer postoperative surveillance. Larger prospective studies are needed to establish definitive shunt selection criteria.
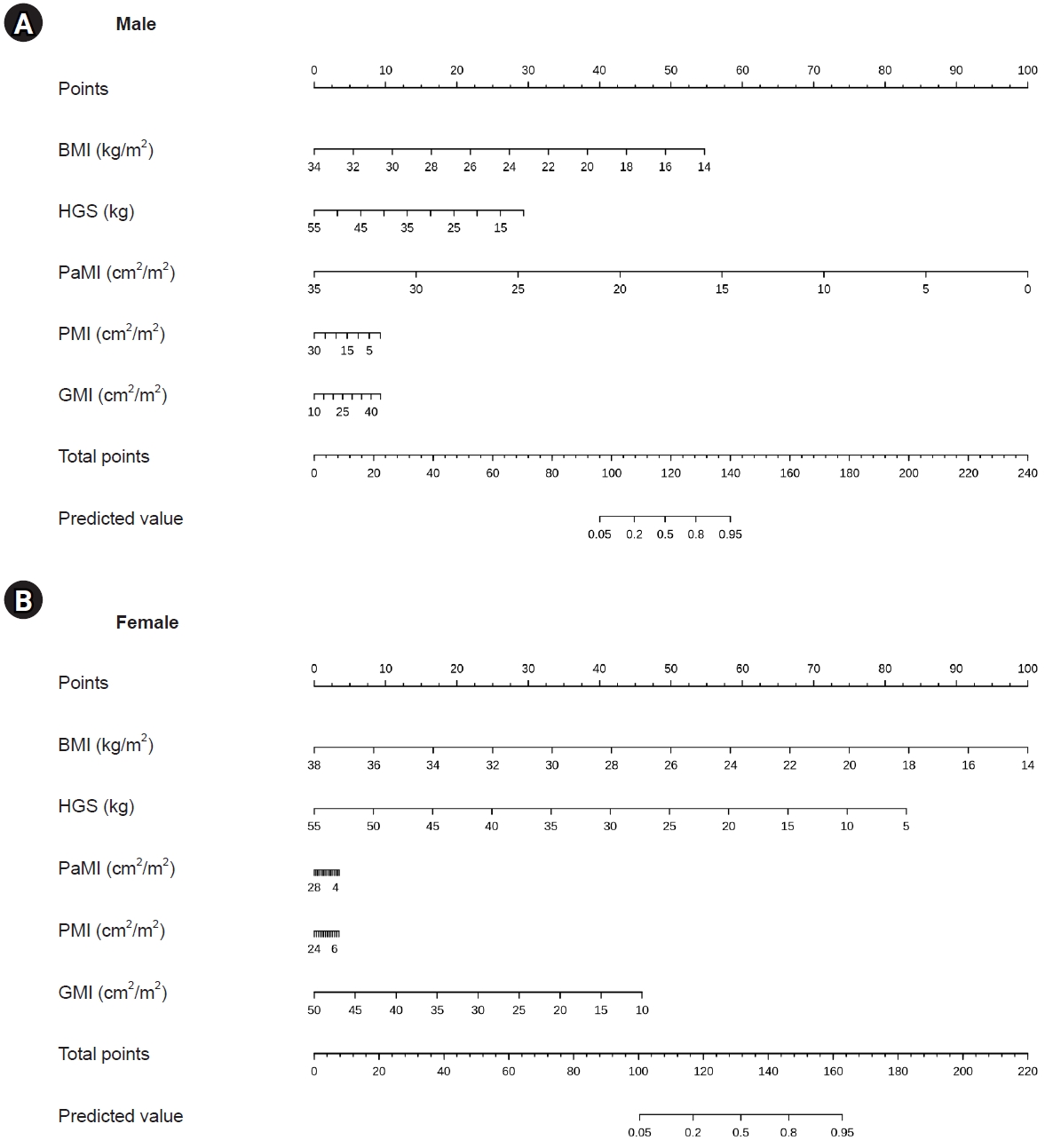
Study Design A retrospective diagnostic accuracy study was conducted using internal training and temporal validation cohorts.
Purpose This study aimed to develop and validate sex-specific diagnostic nomograms for sarcopenia in patients with degenerative lumbar disease (DLD), based on body mass index (BMI), hand-grip strength (HGS), and computed tomography (CT)–derived lumbar muscle indices.
Overview of Literature: The Asian Working Group for Sarcopenia (AWGS) 2019 algorithm requires appendicular skeletal muscle mass (ASM) measurement by dual-energy X-ray absorptiometry or bioimpedance analysis together with HGS and a physical performance test. These measurements are not always feasible in spine clinics, although a preoperative lumbar CT is routinely available.
Methods A training set of 196 patients scheduled for lumbar surgery and a temporal validation set of 150 patients with DLD were analyzed. Sarcopenia was diagnosed according to the AWGS 2019 criteria. Sex-specific multivariable logistic regression was performed using BMI, HGS, psoas muscle index, paraspinal muscle index (PaMI), and gluteal muscle index (GMI), and the resulting models were translated into nomograms. Discrimination was assessed by the area under the receiver operating characteristic curve (AUC), calibration by calibration plots and mean absolute error (MAE), and the optimal cut-off was identified using the Youden index.
Results The prevalence of sarcopenia was 62.2% (122/196) in the training set and 58.0% (87/150) in the validation set. In the training set, sarcopenic patients had significantly lower BMI (23.7±3.7 vs. 27.0±3.3 kg/m2), HGS (20.3±8.0 vs. 29.2±30.5 kg), PaMI (8.7±5.4 vs. 13.9±8.0), and GMI (26.1±5.7 vs. 30.9±6.2) than non-sarcopenic patients (all p<0.05). On validation, the male nomogram achieved an AUC of 0.958 with an MAE of 0.040, and the female nomogram achieved an AUC of 0.830 with an MAE of 0.021. The Youden index was 0.78 for males and 0.59 for females.
Conclusion Sex-specific nomograms based on BMI, HGS, and CT-derived lumbar muscle indices provided accurate diagnosis of sarcopenia in patients with DLD without requiring whole-body ASM measurement or a physical performance test, offering a practical screening tool in the spine clinic.
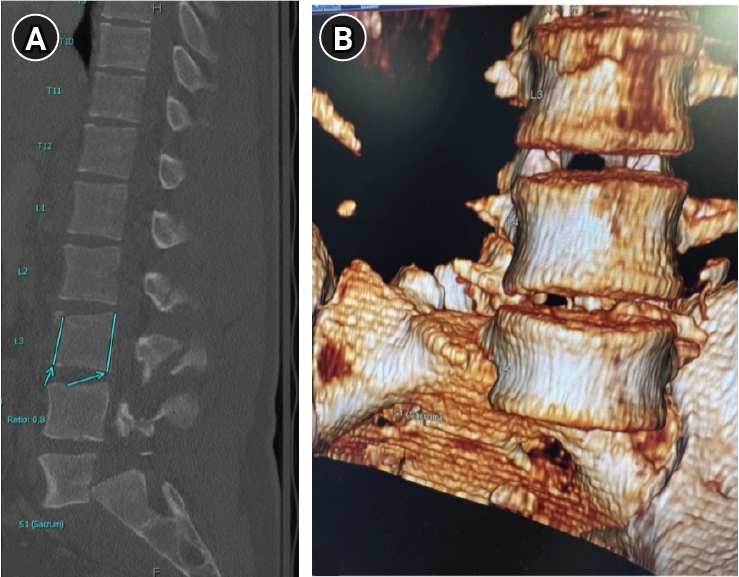
Traumatic lumbar spondyloptosis is a rare entity associated with high-velocity mechanisms and is the most severe form of lumbar spondylolisthesis. Operative management is often required; however, the relative merits of reduction versus in situ fusion remain debated, largely owing to the technical difficulty of attaining satisfactory fracture reduction. In this report, we describe external femoral traction as a novel technique for closed reduction of traumatic lumbar spondyloptosis. A 27-year-old man presented after a tree he was cutting fell on him and was found to have T3–7 AO Spine (AOS) A1 fracture, L3 AOS B2 fracture, and L5 AOS C fracture. Neurologic exam was consistent with multilevel nerve root injury. Definitive treatment included bilateral femoral traction, open reduction, and combined anterior/posterior fixation. A multidisciplinary team including orthopedic surgery, plastic surgery, vascular surgery, and neurosurgery were involved. Complete reduction was obtained, and the patient experienced near-complete resolution of neurologic symptoms. This technique offers a unique solution to the challenge of traumatic lumbar spondyloptosis. Further study and follow-up are needed to confirm the utility and durability of this technique and the cranial extent of injury for which this technique might be applied.
Postoperative radicular pain may persist after lumbar spine surgery despite adequate decompression and the absence of a definite compressive lesion on imaging. Management of such cases remains challenging. This study aimed to report the clinical outcomes of combined pulsed radiofrequency (PRF) and low-temperature thermal radiofrequency. We retrospectively reviewed two patients with postoperative radicular pain without evidence of a high-grade compressive lesion. Both patients showed temporary relief after selective nerve root block. PRF (42°C, 120 seconds), followed by low-temperature thermal radiofrequency (55°C, 60 seconds), was applied under fluoroscopic guidance. Both patients demonstrated significant pain reduction without neurological complications, and symptom improvement was maintained for at least 12 months. The combination of PRF and low-temperature thermal radiofrequency may represent a feasible minimally invasive treatment option. Further studies are required to clarify its effectiveness and indications.
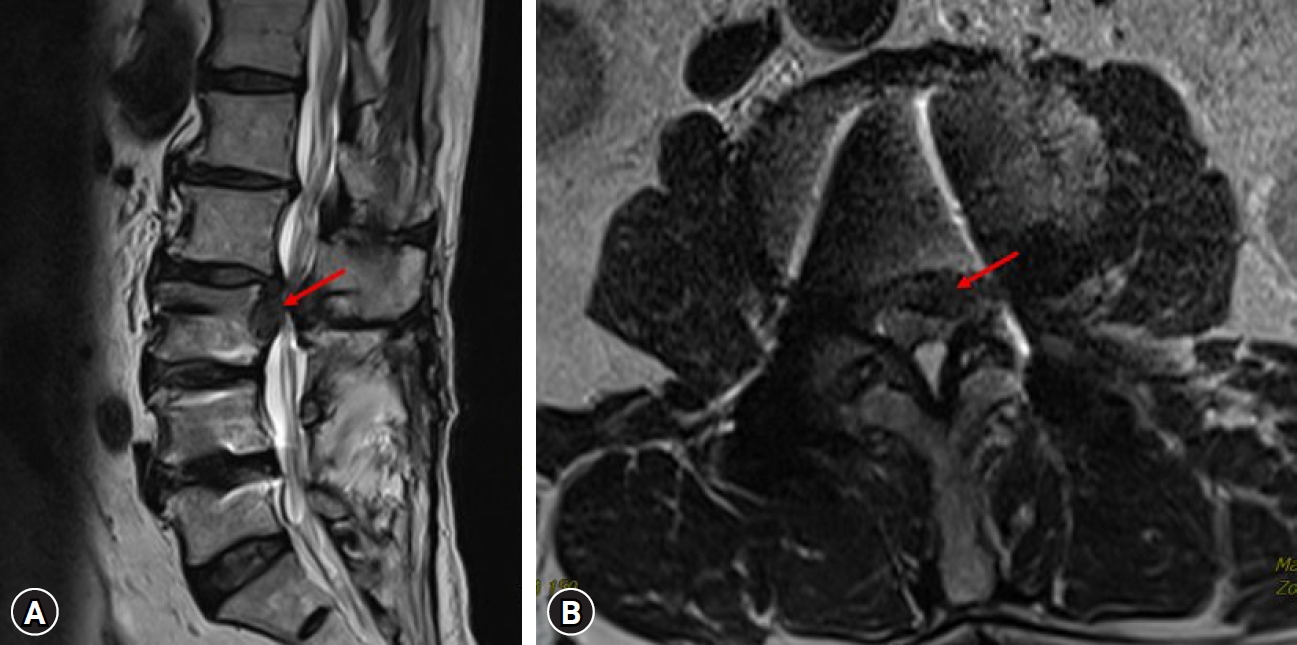
The incidence of compression fractures is increasing in aging populations. Differentiating pathological fracture types is complex and requires careful consideration during diagnosis. This case report describes the clinical course of a 54-year-old female patient presenting with progressive paraplegia after a back injury sustained while lifting a heavy object. Initial imaging revealed a burst fracture at T12 and severe spinal cord compression due to an epidural mass extending from T12 to L2. Clinical assessment raised suspicions of a hematologic malignancy or pathological fractures. Laminectomy and spinal fusion, along with mass removal, resulted in partial improvement in motor function and patient-reported pain levels. However, further evaluation and biopsy revealed chronic inflammation with fibrosis consistent with an unresolved hematoma. This case underscores the importance of a comprehensive differential diagnosis and multidisciplinary collaboration, integrating radiologic, surgical, and pathologic correlation, in the management of complex spinal pathologies.
Dysplastic spondylolisthesis is a developmental subtype characterized by congenital lumbosacral abnormalities and progressive instability. Primary presentation with cauda equina syndrome (CES) has rarely been reported. We report a rare case of CES associated with highgrade dysplastic spondylolisthesis in a patient with concurrent giant ovarian teratomas, which contributed to delayed diagnosis and treatment because of overlapping pelvic symptoms. The patient presented with progressive urinary dysfunction, saddle anesthesia, and lower- extremity symptoms. Radiographic evaluation demonstrated high-grade L5–S1 dysplastic spondylolisthesis with severe canal compromise and lumbosacral deformity. Surgical treatment involved neural decompression and controlled deformity correction with sacral dome osteotomy and interbody fusion performed under provisional stabilization. Postoperatively, the patient demonstrated meaningful neurological recovery with improvement of urinary symptoms and restoration of lumbosacral alignment. This case highlights that CES can occur as an initial manifestation of dysplastic spondylolisthesis and underscores the importance of early spinal evaluation and timely surgical treatment with appropriate reduction techniques to prevent further neurological deterioration in patients with persistent neurological symptoms.

 First
First Prev
Prev

