
| Se-Jun Park | 7 Articles |
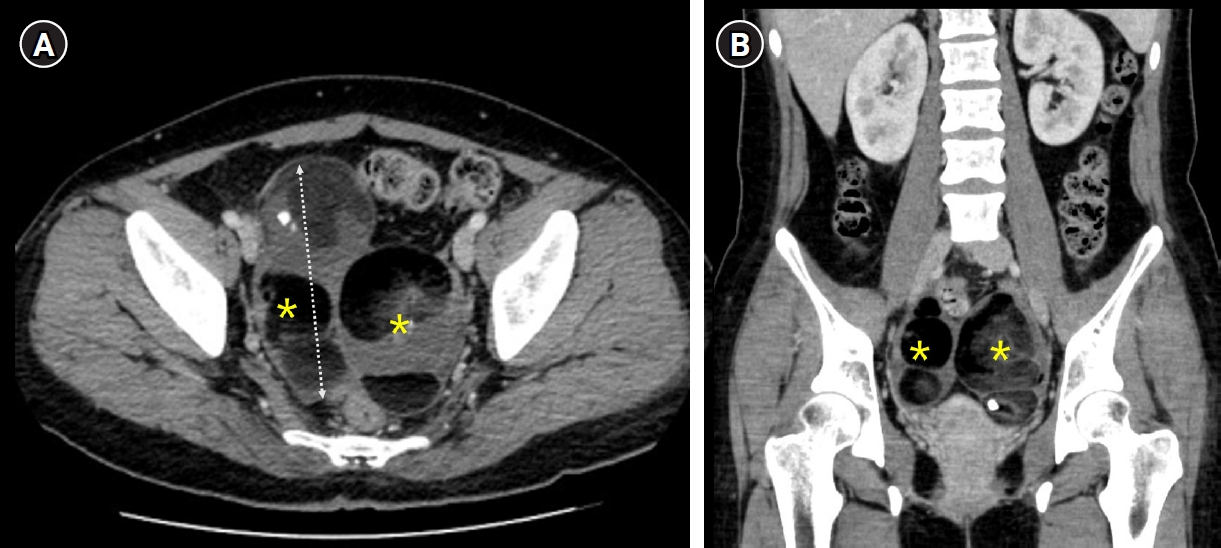
Dysplastic spondylolisthesis is a developmental subtype characterized by congenital lumbosacral abnormalities and progressive instability. Primary presentation with cauda equina syndrome (CES) has rarely been reported. We report a rare case of CES associated with highgrade dysplastic spondylolisthesis in a patient with concurrent giant ovarian teratomas, which contributed to delayed diagnosis and treatment because of overlapping pelvic symptoms. The patient presented with progressive urinary dysfunction, saddle anesthesia, and lower- extremity symptoms. Radiographic evaluation demonstrated high-grade L5–S1 dysplastic spondylolisthesis with severe canal compromise and lumbosacral deformity. Surgical treatment involved neural decompression and controlled deformity correction with sacral dome osteotomy and interbody fusion performed under provisional stabilization. Postoperatively, the patient demonstrated meaningful neurological recovery with improvement of urinary symptoms and restoration of lumbosacral alignment. This case highlights that CES can occur as an initial manifestation of dysplastic spondylolisthesis and underscores the importance of early spinal evaluation and timely surgical treatment with appropriate reduction techniques to prevent further neurological deterioration in patients with persistent neurological symptoms.
Objective
To investigate stiffness-related disability (SRD) following surgical treatment in adolescent idiopathic scoliosis (AIS) patients particularly with respect to the lowest instrumented vertebra (LIV). Summary of Background Extensive spinal fusion inevitably results in loss of mobility which may induce SRD during activities of daily living. Few studies have examined SRD after surgical correction for AIS. Methods Patients who underwent surgical correction for AIS between 2014 and 2021 and were followed up for two years were included. The degree of SRD was evaluated using the Stiffness-Related Disability Index (SRDI) which consists of four categories, each containing three questions, giving a total of 12 components of the questionnaire. The SRDI scores were compared according to the (LIV) levels. Correlation analysis was performed to examine the relationship between the SRDI and legacy health-related quality of life (HRQOL) measurements. Results This study included 174 patients (47 males, 127 females) with a mean age of 13.8 years. Among the 12 items of the SRDI, the scores of nine items showed a significant increase after surgery. The total sum of the SRDI scores also significantly increased after surgery. Pearson correlation analysis showed that the SRDI scores were significantly correlated with ODI (Oswestry disability index), nearly all domains, and the total sum of SRS-22 (Scoliosis Research Society-22 questionnaire), and SF-36 (Short Form 36 health questionnaire). No differences in the SRDI score were found among cases with the LIV between T12 and L3. However, The SRDI scores of patients with LIV at L4 were significantly higher than those of patients with other LIV levels. . Conclusions Various degree of SRD occurred after spinal fusion for AIS. The SRDI significantly correlated with the HRQOL measures. The SRDI score was highest in patients with the LIV at L4 compared to those with other LIV levels.
Objective
Proximal junctional fracture (PJFx) at the uppermost instrumented vertebra (UIV) or UIV+1 is the most common mechanism of PJF. There are few studies assessing the radiographic progression after PJFx development. Therefore, this study sought to identify the risk factors for radiographic progression of PJFx in surgical treatment for ASD. Methods In this retrospective study, among 317 patients aged > 60 years who underwent ≥5-level fusion from the sacrum, 76 with PJFx development were included. According to the change in proximal junctional angle (PJA), two groups were created: Group P (change ≥10°) and Group NP (change <10°). Patient, surgical, and radiographic variables were compared between the groups to demonstrate risk factors for PJFx progression using uni- and multivariate analysis. The receiver operating characteristic (ROC) curve was used to calculate cutoff values. Clinical outcomes, such as visual analog scale (VAS) scores for back and leg pain, the Oswestry Disability Index (ODI) score, and the Scoliosis Research Society (SRS)-22 score, and revision rate were compared between the two groups. Results The mean age at the index surgery was 71.1 years, and there were 67 women enrolled in the study (88.2%). There were 45 patients in Group P and 31 in Group NP. A mean increase of PJA was 15.6° (from 23.2° to 38.8°) in Group P and 3.7° (from 17.2° to 20.9°) in Group NP. The clinical outcomes were significantly better in Group NP than Group P, including back VAS score, ODI value, and the SRS-22 scores for all items. Revision rate was significantly greater in group P than in group NP (17.8% vs. 51.6%, p=0.001). Multivariate analysis revealed that overcorrection relative to the age-adjusted ideal pelvic incidence (PI)–lumbar lordosis (LL) target at the index surgery (odds ratio [OR]=4.484, p=0.030], PJA at the time of PJFx identification (OR=1.097, p=0.009), fracture at UIV versus UIV+1 (OR =3.410, p=0.027) were significant risk factors for PJFx progression. The cutoff value of PJA for PJFx progression was calculated as 21° using the ROC curve. Conclusions The risk factors for further progression of PJFx were overcorrection relative to age-adjusted PI–LL target at the index surgery, PJA > 21° at initial presentation, and fracture at the UIV level. Close monitoring is warranted for such patients not to miss the timely revision surgery.
Background
The Selective thoracic fusion (STF) may be associated with risk of postoperative coronal decompensation, lumbar decompensation and adding-on phenomenon, which can lead to persistence of the lumbar curve and consequently to deviation of the trunk. Therefore, the STF is the most debatable issue as the optimal surgical correction in adolescent idiopathic scoliosis with Lenke 1C curves. Methods A total of 30 patients with adolescent idiopathic scoliosis with Lenke 1C curves who underwent STF between 1996 and 2017 were included. Minimum follow-up duration was five years. We analyzed the incidence of coronal decompensation, lumbar decompensation, distal adding-on phenomenon and trunk shift in these patients for radiographic adverse event. Clinical outcome was assessed by using the Scoliosis Research Society (SRS)-22r scores. Results The mean age at the time of surgery was 13.8±2.9 years. The mean follow-up duration was 80.4±12.3 months. The Cobb’s angle for main thoracic curve improved by 59.6% (p<0.001), and also The Cobb’s angle for thoracolumbar/ lumbar curve improved by 40.5% comparing preoperative and postoperative values (p<0.001). There was significant improvement in the Cobb’s angle for main thoracic and Thoracolumbar/lumbar curve comparing preoperative and last follow-up values (p<0.001). At last follow-up, the coronal balance was 10.3 ± 9.1 that significant improved from the immediate postoperative value (p=0.033). The incidence of coronal decompensation, lumbar decompensation, adding-on and trunk shift in our cohort was 16.7%, 10.0%, 13.3% and 10.0% respectively. The average SRS score at last follow-up in patients with radiographic adverse events was 4.3±0.5. That of patients without adverse events was 4.4±0.6. All domains between patients with and without adverse events had no statistical significance difference. Conclusions Selective thoracic fusion in Lenke 1C curves have acceptable risk of coronal decompensation, lumbar decompensation, distal adding-on, trunk shift. However, no revision surgery was required in these patients after long term follow-up. Therefore, STF in Lenke 1C curves seems to be enough.
Background
Proximal junctional kyphosis (PJK) following long instrumented fusion is a well-recognized complication that does not negatively affect the clinical outcomes. However, there were few studies with regard to the long-term consequences of PJK. Objective: To investigate the long-term clinical and radiographic consequences of proximal junctional kyphosis (PJK) following the long instrumented fusion for elderly patients with sagittal imbalance. Methods Patients older than 60 years who underwent ≥4 fusion including the sacrum for sagittal imbalance were followed up longer than five years. PJK was defined as proximal junctional angle (PJA) >10° without any bony compromise or myelopathy. The radiographic and clinical outcomes were compared between PJK and non-PJK groups. Clinical outcome measures included visual analog scale (VAS) for back and leg, Oswestry disability index (ODI), and Scoliosis Research Society (SRS)-22 scores. Results A mean age was 69.2 years. An average follow-up duration was 92.4 months. There were 30 patients in PJK group and 43 in non-PJK group. At the final follow-up, pelvic incidence-lumbar lordosis mismatch, pelvic tilt, and sacral vertical axis were not different between the two groups. In PJK group, PJA significantly increased from 6.5° postoperatively to 21.2° at the final follow-up. At the final follow-up, clinical outcomes were worse in PJK group than in non-PJK group with regard to VAS for back, ODI, and SRS-22 scores except satisfaction domain. Three (10%) of 30 patients underwent a revision surgery for PJK progression. Conclusions PJK progressed with time and negatively affect the clinical outcomes in a long-term follow-up after ASD surgery.
Purpose
There were few available data regarding the prognosis after the surgical treatment for spinal metastases from non-small cell lung cancer (NSCLC) despite its great frequency. The aim of this study was to investigate the prognostic factors for patients who underwent the surgical treatment for spinal metastases from NSCLC. Materials and Methods Eighty-seven patients who underwent surgical treatment for spinal metastases from NSCLC were followed up semi-prospectively. There were 43 patients with metastatic spinal cord compression (MSCC) and 44 patients without MSCC. The prognosis analysis was performed according to 3-categorical variables: patients’ , oncologic, and treatments’ factors. Major complications and mortality rate were recorded. The impact of postoperative chemotherapy was evaluated separately. Results The overall survival time was median 6.8 months. Postoperative ECOG-PS (0-2 vs. 3, 4) was shown as a significant prognostic factors in both MSCC and non-MSCC groups with HR (hazards ratio) of 2.46 and 2.54, respectively. Major complications developed in 26 patients and 30-day mortality rate was 8.0%. The presence of major complications was also prognostic factor in both groups with HR of 2.55 and 4.47. Earlier surgery within 72 hours showed better prognosis in MSCC group with HR of 2.46. Patients who underwent postoperative chemotherapy survived longer significantly than those who couldn’t with median survival time of 12.0 vs 2.8 months. Conclusions Postoperative ECOG-PS and complications were significant prognostic factors in both groups and earlier surgery in MSCC group. The postoperative chemotherapy was another independent prognostic factor affecting the survival time
Purpose
Despite the increasing prevalence of spinal deformity correction using lateral lumbar interbody fusion (LLIF) for degenerative adult spinal deformity, the amount of sagittal plane correction is reported to be suboptimal. Thus, authors have performed mini-open anterior lumbar interbody fusion (ALIF) at the most caudal segment in adjunct to LLIF to make sufficient lumbar lordosis (LL). This study is performed to demonstrate the feasibility of mini-open anterior lumbar interbody fusion (ALIF) combined with lateral lumbar interbody fusion (LLIF) followed by 2-stage posterior fixation in terms of the correction capacity and complications by comparing with a matched control group undergoing posterior-only surgery. Materials and Methods This study was case-control study. Thirty patients who underwent ALIF with LLIF followed by 2-stage posterior fixation (ALIF/LLIF group) for adult spinal deformity were compared to 60 patients who underwent posterior-only surgery (posterior group) and were matched according to age, sex, diagnosis, fusion length, pelvic incidence (PI), and follow-up duration. Spinopelvic parameters, hospitalization data, clinical outcomes, and complications were evaluated and compared between ALIF/LLIF and posterior groups. Results In the ALIF/LLIF group, interbody fusions were performed for a mean of 4.0 levels, comprising 1.6 and 2.4 levels for ALIF and LLIF, respectively. Interbody fusion in the posterior group was performed for a mean of 3.3 levels. The mean follow-up duration did not differ between two groups (16.7 mo vs. 19.2 mo, p=0.056). Postoperative LL was greater in the ALIF/LLIF than in the posterior group (52.0° vs. 40.9°, p<0.001). The reduction in the sagittal vertical axis was also greater for the ALIF/LLIF group than the posterior group (62.3 mm vs. 24.7 mm). The operation time of the ALIF/LLIF group was longer than the posterior group (11.2 hr vs. 8.6 hr, p<0.001), while estimated blood loss and red cell transfusion was less in the ALIF/LLIF group. Medical complications developed more frequently in the posterior group, while perioperative surgical complications were not different between groups. Delayed surgical complications were observed more in the posterior group. In the posterior group, there were 7 patients who experienced nonunion and rod breakage and 10 patients who experienced decompensation, while there were no such cases in the ALIF/LLIF group. Conclusion Mini-open ALIF combined with LLIF can restore sagittal balance more appropriately with a lower rate of complications compared with posterior-alone surgery for the correction of ASD.
|
|
