Purpose This retrospective study investigated the distinct clinical and radiographic drivers of early- versus late-onset proximal junctional kyphosis (PJK) following multilevel thoracolumbar (TL) fusion.
Methods After applying the exclusion criteria (spinal infection, neuromuscular disease, age <50 years), the analysis included 136 patients who underwent ≥4-level TL fusion and were followed up for a minimum of 2 years. PJK was classified as early (≤6 months) or late (>6 months) onset. Patient-related factors, surgical variables, sagittal spinopelvic parameters, and preoperative magnetic resonance imaging findings were analyzed using multivariate logistic regression to identify independent predictors of early PJK.
Results Among 24 patients (17.6%) who developed PJK, the early and late-onset groups included 13 and 11 patients, respectively. The early PJK group exhibited significantly greater preoperative and postoperative TL angles compared with the late group (preoperative: 23.03±13.83° vs. 9.67±9.67°, p=0.024; postoperative: 19.6±6.95° vs. 6.95±6.35°, p<0.001). The Pfirrmann grade of the L1–2 intervertebral disc was significantly higher in the early PJK group (3.92±0.95 vs. 2.81±0.60, p=0.006). No surgical variables differed significantly between the groups. Multivariate analysis confirmed greater postoperative TL angle and more advanced L1–2 disc degeneration as independent predictors of early PJK.
Conclusion Early-onset PJK following multilevel TL fusion is primarily driven by regional biomechanical vulnerabilities, specifically residual postoperative TL kyphosis and advanced adjacent L1–2 disc degeneration, rather than by surgical variables. Meticulous evaluation of regional TL alignment and adjacent disc health during surgical planning is critical for risk stratification and prevention of early junctional failure.
Study Design A retrospective diagnostic accuracy study was conducted using internal training and temporal validation cohorts.
Purpose This study aimed to develop and validate sex-specific diagnostic nomograms for sarcopenia in patients with degenerative lumbar disease (DLD), based on body mass index (BMI), hand-grip strength (HGS), and computed tomography (CT)–derived lumbar muscle indices.
Overview of Literature: The Asian Working Group for Sarcopenia (AWGS) 2019 algorithm requires appendicular skeletal muscle mass (ASM) measurement by dual-energy X-ray absorptiometry or bioimpedance analysis together with HGS and a physical performance test. These measurements are not always feasible in spine clinics, although a preoperative lumbar CT is routinely available.
Methods A training set of 196 patients scheduled for lumbar surgery and a temporal validation set of 150 patients with DLD were analyzed. Sarcopenia was diagnosed according to the AWGS 2019 criteria. Sex-specific multivariable logistic regression was performed using BMI, HGS, psoas muscle index, paraspinal muscle index (PaMI), and gluteal muscle index (GMI), and the resulting models were translated into nomograms. Discrimination was assessed by the area under the receiver operating characteristic curve (AUC), calibration by calibration plots and mean absolute error (MAE), and the optimal cut-off was identified using the Youden index.
Results The prevalence of sarcopenia was 62.2% (122/196) in the training set and 58.0% (87/150) in the validation set. In the training set, sarcopenic patients had significantly lower BMI (23.7±3.7 vs. 27.0±3.3 kg/m2), HGS (20.3±8.0 vs. 29.2±30.5 kg), PaMI (8.7±5.4 vs. 13.9±8.0), and GMI (26.1±5.7 vs. 30.9±6.2) than non-sarcopenic patients (all p<0.05). On validation, the male nomogram achieved an AUC of 0.958 with an MAE of 0.040, and the female nomogram achieved an AUC of 0.830 with an MAE of 0.021. The Youden index was 0.78 for males and 0.59 for females.
Conclusion Sex-specific nomograms based on BMI, HGS, and CT-derived lumbar muscle indices provided accurate diagnosis of sarcopenia in patients with DLD without requiring whole-body ASM measurement or a physical performance test, offering a practical screening tool in the spine clinic.
Traumatic lumbar spondyloptosis is a rare entity associated with high-velocity mechanisms and is the most severe form of lumbar spondylolisthesis. Operative management is often required; however, the relative merits of reduction versus in situ fusion remain debated, largely owing to the technical difficulty of attaining satisfactory fracture reduction. In this report, we describe external femoral traction as a novel technique for closed reduction of traumatic lumbar spondyloptosis. A 27-year-old man presented after a tree he was cutting fell on him and was found to have T3–7 AO Spine (AOS) A1 fracture, L3 AOS B2 fracture, and L5 AOS C fracture. Neurologic exam was consistent with multilevel nerve root injury. Definitive treatment included bilateral femoral traction, open reduction, and combined anterior/posterior fixation. A multidisciplinary team including orthopedic surgery, plastic surgery, vascular surgery, and neurosurgery were involved. Complete reduction was obtained, and the patient experienced near-complete resolution of neurologic symptoms. This technique offers a unique solution to the challenge of traumatic lumbar spondyloptosis. Further study and follow-up are needed to confirm the utility and durability of this technique and the cranial extent of injury for which this technique might be applied.
Chondroma is a benign cartilaginous neoplasm, rarely encountered in the lumbar spine. We report a case involving a 70-year-old female who presented with lower limb radiating pain that started four years ago. Although no pronounced muscle weakness was noted, the patient experienced progressively worsening radiating pain in the L4 dermatome. Initial evaluation, including magnetic resonance imaging (MRI) performed at another medical facility, suggested a potential lesion associated with left L4–5 lumbar disc herniation. Despite non-surgical interventions, the patient experienced limited symptomatic relief, prompting her to seek further care at our clinic. Subsequent contrast-enhanced MRI conducted at our facility revealed a mass exhibiting peripheral rim enhancement surrounding the L4 nerve root. Suspecting a neurogenic tumor, we decided to perform surgical excision of the mass. Postsurgery, histopathological analysis confirmed the presence of hyaline cartilage with lobular architecture and chondrocytes in lacunae, leading to the conclusive diagnosis of chondroma. Following the surgical procedure, the previously reported radiating pain exhibited notable improvement.
Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Purpose To evaluate the association between lumbar lordosis and age using an AI-based automated measurement model applied to a large dataset of standing lateral spinal radiographs.
Materials and Methods This retrospective study analyzed 904 high-quality radiographs selected from 2,397 images acquired between 2019 and 2021. Lumbar lordosis was defined as the angle between the superior endplates of L1 and S1 and automatically measured using a validated deep learning model. Subjects were categorized into nine age groups. One-way ANOVA compared lumbar lordosis across age groups, and Pearson correlation assessed the relationship between age and lumbar lordosis.
Results Lumbar lordosis ranged from 0° to 84° (mean 45.9°±13.4°). The highest mean value was in the 10–19-year group (52.1°), and the lowest in the ≥80-year group (39.6°). Minimum values decreased to 0° in individuals aged ≥60 years. No significant differences were found across age groups (p=0.561). A weak but significant negative correlation was observed between age and lumbar lordosis (r=–0.247, p<0.0001).
Conclusions AI-based automated measurement enabled efficient large-scale analysis and revealed a wide distribution of lumbar lordosis with a gradual age-related decline. These findings highlight the value of AI in spinal alignment assessment.
Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
Purpose To develop and validate a deep learning–based artificial intelligence (AI) model for automated measurement of lumbar lordosis (LL) angles from whole spine lateral radiographs.
Materials and Methods A total of 888 lateral spine X-rays (2019–2021) were retrospectively collected and annotated with four anatomical keypoints (L1 and S1 vertebral landmarks). An AI model using Detectron2 with a Keypoint R-CNN and ResNeXt-101 backbone was trained with data augmentation. Performance was evaluated on 50 test images, comparing AI results to manual annotations by two orthopedic surgeons using intraclass correlation coefficient (ICC), Pearson’s correlation, and Bland–Altman analysis.
Results The model achieved an average precision of 71.63 for bounding boxes and 86.61 for keypoints. ICCs between AI and human raters ranged from 0.918 to 0.962. Pearson correlation coefficients were r=0.849 and r=0.903. Bland–Altman analysis showed minor underestimation biases (–3.42° and –4.28°) with acceptable agreement.
Conclusions The AI model showed excellent agreement with expert measurements and high reliability in LL angle assessment. Despite a slight underestimation, it offers a scalable, consistent tool for clinical use. Further studies should evaluate generalizability and interpretability in broader settings.
Citations
Citations to this article as recorded by
Deep Learning–based AI Analysis of the Correlation Between Lumbar Lordosis and Age Soo-Bin Lee, Ja-Yeong Yoon, Dong-Sik Chae, Sang-Bum Kim, Young-Seo Park, Kyung-Yil Kang, Min-Kyu Lee Journal of Advanced Spine Surgery.2025; 15(2): 78. CrossRef
Efficacy of Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Meta-Analysis With Single-Arm Analysis and Comparative Analysis With Microscopic Decompression and Uniportal Endoscopic Decompression Shuangwen Lv, Haiwen Lv, Yupeng He, Xiansheng Xia Operative Neurosurgery.2024; 27(2): 158. CrossRef
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Objective To investigate the utility of a deep learning model in diagnosing traumatic lumbar fractures on computed tomography (CT) images.
Summary of Background Data: CT scans are widely used as the first choice for detecting spinal fractures in patients with severe trauma. Although CT scans have high diagnostic accuracy, fractures can occasionally be missed.
Recently, deep learning has been applied in various fields of medical imaging.
Methods CT images from 480 patients (3695 vertebrae) who visited a level-one trauma center with lumbar fractures were retrospectively analyzed. The diagnostic results were confirmed by two experienced musculoskeletal radiologists and one experienced spine surgeon using magnetic resonance imaging (MRI). Deep learning networks were employed for diagnosis, with 425 cases used for training and 55 cases for testing. Sensitivity, specificity, accuracy, and the area under the receiver operating characteristic curve (AUROC) were calculated to evaluate diagnostic performance.
Results The model successfully identified 107 out of 129 vertebrae with fractures, achieving a sensitivity of 82.95%, a specificity of 93.24%, an AUROC of 0.936, and an overall accuracy of 88.45%.
Conclusions This study demonstrated that the deep learning model showed high accuracy in diagnosing traumatic lumbar fractures. This approach has the potential to assist spine specialists, radiologists, and trauma care experts.
Further validation is needed to determine its effectiveness in clinical settings.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Purpose Few studies have assessed the prevalence of cervical and thoracic and lumbar (thoracolumbar) intervertebral disc disorders, respectively, using data from the Korean National Health Insurance Service (KNHIS).
The aim is to show the changing prevalence of cervical and thoracolumbar intervertebral disc disorder over the last decade.
Methods Data spanning 2012 to 2021 were collected from the KNHIS, encompassing primary diagnoses related to cervical and thoracolumbar intervertebral disc disorder (ICD 10 code: M50.x and M51.x except M51.4). The agestandardized prevalence was computed using the estimated Korean population in 2020 as a reference. Additionally, age-standardized number of general spinal operations per year was illustrated using the Statistical Yearbook of Major Surgeries in 2021.
Results In 2012, the age-standardized prevalence of cervical intervertebral disc disorder was 11,383 persons per 100,000 decreasing to 8,860 persons per 100,000 persons in 2021. This decline was observed in both male (from 10,101 to 8,012) and female (from 12,690 to 9,709). For thoracolumbar intervertebral disc disorders, the agestandardized prevalence decreased from 27,506 to 18,903 persons per 100,000 persons from 2012 to 2021. Notably, the age-standardized prevalence showed a greater increase in individuals aged 60 or older compared to those aged 50, for both sexes. However, there was an increase in the number of general spinal operation from 2012 to 2021.
Conclusions While the overall age-standardized prevalence of cervical and thoracolumbar intervertebral disc disorders decreased between 2012 and 2021 across all age groups, the number of general spinal operations increased during the same period.
Background This study aims to assess the clinical and radiographic outcomes of biportal endoscopic lumbar discectomy compared to microscopic lumbar discectomy in obese patients with lumbar herniated discs. Previous research has established a positive correlation between operation time and estimated blood loss in obese patients undergoing microscopic lumbar discectomy, based on an increase in body mass index. However, no studies have specifically examined the outcomes of biportal endoscopic lumbar discectomy in this patient population. Therefore, this study seeks to fill this research gap and provide valuable insights into the effectiveness of these two surgical approaches for obese patients with lumbar herniated discs.
Methods This retrospective multicenter study analyzed and compared clinical and radiological data from 48 obese patients with a body mass index (BMI) greater than 30 kg/m2 who underwent either microscopic or biportal endoscopic lumbar discectomy. The study assessed clinical outcomes using the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores. Radiological data were obtained through magnetic resonance imaging (MRI) scans.
Results The study included a total of 48 patients, with 31 patients undergoing microscopic discectomy and 17 patients undergoing biportal endoscopic discectomy. Both groups showed improvements in VAS, ODI, and EQ-5D scores following surgery compared to preoperative scores. However, there was no significant difference in these outcome measures between the two surgical techniques. Although there was a no significant difference in the occurrence of recurrent disc herniation confirmed by postoperative MRI, there was significant difference in the number of patients requiring additional surgery between the two groups.
Conclusions For obese patients with lumbar disc herniation that did not respond to conservative treatment, this study found no significant differences in clinical or radiological outcomes between microscopic and biportal endoscopic surgery methods. However, it is worth noting that the biportal group had a lower incidence of reoperation compared to the microscopic group.
Background The Selective thoracic fusion (STF) may be associated with risk of postoperative coronal decompensation, lumbar decompensation and adding-on phenomenon, which can lead to persistence of the lumbar curve and consequently to deviation of the trunk. Therefore, the STF is the most debatable issue as the optimal surgical correction in adolescent idiopathic scoliosis with Lenke 1C curves.
Methods A total of 30 patients with adolescent idiopathic scoliosis with Lenke 1C curves who underwent STF between 1996 and 2017 were included. Minimum follow-up duration was five years. We analyzed the incidence of coronal decompensation, lumbar decompensation, distal adding-on phenomenon and trunk shift in these patients for radiographic adverse event. Clinical outcome was assessed by using the Scoliosis Research Society (SRS)-22r scores.
Results The mean age at the time of surgery was 13.8±2.9 years. The mean follow-up duration was 80.4±12.3 months.
The Cobb’s angle for main thoracic curve improved by 59.6% (p<0.001), and also The Cobb’s angle for thoracolumbar/ lumbar curve improved by 40.5% comparing preoperative and postoperative values (p<0.001). There was significant improvement in the Cobb’s angle for main thoracic and Thoracolumbar/lumbar curve comparing preoperative and last follow-up values (p<0.001). At last follow-up, the coronal balance was 10.3 ± 9.1 that significant improved from the immediate postoperative value (p=0.033). The incidence of coronal decompensation, lumbar decompensation, adding-on and trunk shift in our cohort was 16.7%, 10.0%, 13.3% and 10.0% respectively. The average SRS score at last follow-up in patients with radiographic adverse events was 4.3±0.5. That of patients without adverse events was 4.4±0.6. All domains between patients with and without adverse events had no statistical significance difference.
Conclusions Selective thoracic fusion in Lenke 1C curves have acceptable risk of coronal decompensation, lumbar decompensation, distal adding-on, trunk shift. However, no revision surgery was required in these patients after long term follow-up. Therefore, STF in Lenke 1C curves seems to be enough.
Background It is well reported that the patient’s age plays an important role associated with proximal junctional failure (PJF) development. Various characteristics of adult spinal deformity (ASD) patients were different between younger and older age groups. We hypothesized that the radiographic risk factors for PJF would different according to younger and older age groups. This study aimed to evaluate different radiographic risk factor of PJF according to the two age groups undergoing thoracolumbar fusion for ASD.
Methods ASD patients aged ≥ 60 years who underwent thoracolumbar fusion from low thoracic level (T9~T12) to sacrum were included. The minimum follow-up duration was two years. PJF was defined as proximal junctional angle (PJA) ≥ 20°, fixation failure, fracture, myelopathy, or necessity of revision surgery. Using various radiographic risk factors including age-adjusted ideal pelvic incidence (PI)-lumbar lordosis (LL), univariate and multivariate analyses were performed separately according to the two age groups : <70 years and ≥70 years.
Results A total of 186 patients were enrolled (mean age=68.5 years old, 90.3% female). Mean follow-up duration was 67.4 months. PJF developed in 98 patients (32.0%). There were fracture in 53 patients, PJA ≥ 20° in 26, fixation failure in 12, and myelopathy in 6. PJF developed more frequently in patients older than 70 years than in younger than 70 years. In patients aged less than 70 years, preoperative LL, PI-LL and change in LL were significant risk factors in univariate analysis. Multivariate analysis showed only change in LL was significant for PJF development (Odds ratio [OR]=1.025, p=0.021). On the other hand, in patients older than 70 years, postoperative LL, postoperative PILL, overcorrection relative to conventional PI-LL target (within ±10°) as well as age-adjusted ideal PI-LL target were significant. On multivariate analysis, only overcorrection of PI-LL relative to age-adjusted ideal target was a single significant factor to cause PJF (OR=5.250, p=0.024).
Conclusions In patients younger than 70 years, greater change in LL was associated with PJF development regardless of PI-related value. However, in older patients, overcorrection of PI-LL relative to the age-adjusted PI-LL target was important to cause PJF.
Background When obese patients underwent lumbar discectomy using a microscope, a correlation was found between the operation time and an increase in estimated blood loss according to the increase in body mass index.
However, except for minor complications, there was no difference in postoperative outcomes between obese and normal-weight patients. These are the results of microscopic lumbar discectomy in obese patients, but there are no studies on biportal endoscopic lumbar discectomy. The aim of this study was to compare the clinical and radiographic outcomes of microscopic and endoscopic discectomy in obese patients.
Methods Clinical and radiological data were compared and analyzed in 23 obese patients with a body mass index of >30 kg/m2 who underwent microscopic and biportal endoscopic lumbar discectomy. Clinical data on the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores were measured, and radiological data were measured using magnetic resonance imaging (MRI).
Results In total, 13 patients who underwent microscopic discectomy and 10 who underwent biportal endoscopic discectomy were enrolled in this study. The VAS, ODI, and EQ-5D scores in both groups improved after surgery compared with those before surgery, although there was no difference between the two groups. Although there was a difference in the incidence of recurrent disc herniation confirmed by MRI after surgery, there was no difference in the number of patients requiring surgery between the two groups.
Conclusions There were no significant clinical or radiological differences in outcomes between microscopic and biportal endoscopic surgery methods.
Background Minimally invasive transpsoas or antepsoas lateral lumbar interbody fusion (MI-LLIF) has been reported as an effective surgical option for various lumbar diseases. Many researchers reported high fusion rate and clinical excellence of LLIF with the use of bone morphogenic protein (BMP). However, there have been paucity of studies regarding LLIF without the use of BMP. Therefore, this study aimed to analyze radiologic and clinical results of patients who underwent minimally invasive lateral lumbar interbody fusion without the use of BMP. Furthermore, a further analysis was conducted regarding the frequency of cage subsidence and its impact on the radiologic and clinical outcome.
Materials and Methods Fifty patients and 109 levels treated by MI-LLIF with postoperative follow-up of at least 2 years were included. Radiologic evaluation included intervertebral disc height, segmental lordosis, lumbar lordosis, fusion rate, cage subsidence grade, and the bone mineral density. Radiologic fusion was determined by modified Bridwell’s grade, and cage subsidence by Marchi’s grade. Clinical outcome was evaluated by VAS of low back pain (LBP) and leg pain, and ODI score. The above clinical and radiologic variables were analyzed statistically for comparison of cage subsidence and nonsubsidence groups.
Results There were 20 male and 30 female patients with the average age of 69 years. Average follow-up period was 29.6 months(24-42 months). Graft material used for PEEK cage was autogenous bone only in 9 levels, autogenous bone and DBM in 19 levels, and DBM only in 81 levels. Twelve patients received surgery on 1 level, 20 patients on 2 levels, 17 patients on 3 levels, and 1 patient on 4 levels, respectively. Operated levels were L1-2 in 7 cases, L2-3 in 27, L3-4 in 41, and L4-5 in 34, respectively. Mean low back pain (LBP) VAS decreased from preoperative 5.5 to 2.2 at the final follow-up, leg pain from 6.1 to 1.7, and ODI score from 25.6 to 13.7, with statistical significance (p<0.001). Mean disc height increased from preoperative 5.9 mm to postoperative 11.5 mm, and subsequently decreased to 9.6mm at the final follow-up. Average lumbar lordosis increased from preoperative 18.6 degrees to postoperative 37.0 degrees, and 35.9 degree at final follow-up. Radiologic union rate was 90.8%. Cage subsidence was observed in 6 levels (5.5%) on immediate postoperative radiographs; and in 20 levels (18.3%) at final follow-up. Comparison between cage subsidence and non-subsidence groups revealed no significant difference in age and BMD. Immediate postoperative segmental lordosis was considered as a risk factor of cage subsidence (p=0.005, odds ratio 0.813, CI 0.703~0.940). Furthermore, the preoperative and the final follow-up measurement of disc height, VAS score of LBP and leg pain, and ODI score were not different between the two groups. However, pseudoarthrosis rate was higher in subsidence group.
Conclusions Minimally invasive LLIF was an effective surgical option with high fusion rate even without the use of BMP.
Although cage subsidence also increases the frequency of pseudarthrosis, it does not significantly deteriorate the lumbar lordosis correction and clinical outcome.
Background Percutaneous-short segment screw fixation (SSSF) without bone fusion has proven to be a safe and effective modality for thoracolumbar spine fractures (TLSFs). When fracture consolidation is confirmed, pedicle screws are no longer essential, but clear indications for screw removal following fracture consolidation have not been established.
Methods In total, we enrolled 31 patients with TLSFs who underwent screw removal following treatment using percutaneous-SSSF without fusion. Plain radiographs, taken at different intervals, measured local kyphosis using Cobb’ angle (CA), vertebra body height (VBH), and the segmental motion angle (SMA). A visual analogue scale (VAS) and the Oswestry disability index (ODI) were applied pre-screw removal and at the last follow-up.
Results The overall mean CA deteriorated by 1.58º (p<0.05) and the overall mean VBH decreased by 0.52 mm (p=0.001). SMA preservation was achieved in 18 patients (58.1%) and kyphotic recurrence occurred in 4 patients (12.9%). SMA preservation was statistically significant in patients who underwent screw removal within 12 months following the primary operation (p=0.002). Kyphotic recurrence occurred in patients with a CA ≥20º at injury (p<0.001) with a median interval of 16.5 months after screw removal. No patients reported worsening pain or an increased ODI score after screw removal.
Conclusion Screw removal within 12 months can be recommended for restoration of SMA with improvement in clinical outcomes. Although, TLSFs with CA ≥20º at the time of injury can help to predict kyphotic recurrence after screw removal, the clinical outcomes are less relevant.
Purpose Minimally invasive technique in spinal surgery have evolved including cortical bone trajectory (CBT) screw technique which is s new lumbar pedicle screw path, as an alternative fixation technique for lumbar spine.
Theoretical advantage is that it provides enhanced screw torque and has biomechanical characteristics, also it minimizes approach-related damages. Midline lumbar fusion (MIDLF) has appeared with CBT screw technique.
Many studies of CBT screw reported the effectiveness of MIDLF. We adopted this technique for lumbar degenerative spondylolisthesis and evaluated early radiological outcomes.
Materials and Methods From May 2014 to March 2015, 17 patients (mean age 65.6±7.5 years; 4 males, 13 females) underwent MIDLF procedures for the treatment of single level lumbar spondylolisthesis. Average follow-up period was 8.8±2.7 months. Initial and last follow-up X-ray and computed tomography (CT) were evaluated for screw malposition, detection of peri-screw halo, loosening of the construct, or signs of spinal instability.
Results The average bone mineral density (BMD) was -1.9±0.8. Eleven patients were fused at L4-5, 5 were at L3-4, and 1 was at L2-3. Five CBT screws were converted into pedicle screws due to intraoperative misposition of screws, so total 63 CBT screws were evaluated for peri-screw halo and malposition. There were no findings of screw pull-out or breakage in all screws. Four out of 63 (6.3%) screws were judged as peri-screw halo, and 20 (41.2%) screws were judged as malposition (1 medial; 2 superior; 17 lateral pedicle violation). But, there were no screw related nerve root injury. In all cases, interbody bony mass were identified. Four out of 17 (23.6%) patients were detected more than 2 degrees motions on flexion-extension lateral X-rays at final follow-up, and 1 out of these 4 patients was identified loss of reduction. There was no operation related complication.
Conclusion There is no doubt that MIDLF with CBT screw is the minimally invasive method. Many numbers of screw malposition identified in our series were thought to be due to our earlier experience of trying free hands technique.
We recommend the use of intraoperative fluoroscopy, which achieve accuracy. Although MIDLF with CBT has theoretical strengths, we must evaluate further long-term clinical follow-up and measure outcome.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Purpose To evaluate whether the contralateral radiating pain improved after unilateral decompression and minimally invasive transforaminal lumbar interbody fusion (TLIF) in the patients with bilateral radiating pain due to degenerative lumbar disease.
Materials and Methods Patients with the degenerative lumbar disease who underwent unilateral minimally invasive TLIF and were followed for more than 1 year were included. Clinically, low back pain and radiating pain on the dominant symptom side and the contralateral side were evaluated by the visual analogue score (VAS), and the Oswestry disability index (ODI) score was also evaluated.
Results ODI and VAS of low back pain and radiating pain were effectively reduced in a total of 57 cases. Thirty cases having bilateral radiating pain, among these patients, unilateral decompression was performed in 15 cases and bilateral decompression thru unilateral approach in 15 patients. In unilateral decompression group, radiating pain on the dominant symptom side, and radiating pain on the contralateral side were also improved at the final followup. In 15 cases who underwent bilateral decompression, radiating pain on the dominant symptom side and the contralateral side were improved at the final follow-up. There was no significant difference between the two groups in terms of preoperative ODI, VAS of low back and radiating pain.
Conclusions Minimally invasive TLIF via unilateral approach with or without contralateral decompression showed good clinical results in patients having unilateral or bilateral radiating pain. Minimally invasive TLIF could be an useful option even if there is bilateral radiating pain in degenerative lumbar disease.
Background Oblique and anterior lumbar interbody fusion have been widely performed in the lumbar spinal disease but we cannot get a direct decompression effect with these procedure.
Objective: The purpose of this study is to report clinical and imaging outcomes of microscope assisted direct decompression combined with oblique lumbar interbody fusion (OLIF) or anterior lumbar interbody fusion (ALIF).
Methods Twelve patients who received microscope assisted direct decompression during OLIF or ALIF for lumbar spinal stenosis were enrolled. The OLIF was performed for the lesion upper than the L4-5 or in the case of multisegmental disease. The ALIF was performed for the lesion at the L5-S1. After anterior-approaching surgery, percutaneous fixation of pedicle screw was performed and we did not perform an additional decompression posteriorly in all cases. For the clinical outcomes, we evaluated short form 36 (SF-36), Oswestry disability index (ODI) score and visual analog scale (VAS) pain score. For the imaging outcomes, we obtained postoperative lumbar magnetic resonance imaging (MRI).
Results The OLIF was performed for 9 patients and the ALIF was performed for 3 patients. In the clinical outcomes, SF-36 was improved from 25.40 to 69.83 and ODI score was also improved from 69.83 to 16.50. VAS pain score of back was improved from 4.3 to 1.6 and VAS pain score of leg was improved from 7.5 to 2.2. In the imaging outcomes, all patients had severe stenosis before surgery. After surgery the severity of the stenosis was reduced to mild state in 9 cases and moderate state in 3 cases postoperatively.
Conclusions We could obtain the good clinical outcomes and effective decompression through microscope assisted direct decompression during OLIF or ALIF.
Purpose The current study aims to report the results of analyzed factors that ultimately undergo surgical treatment after selective nerve root block in patients with spinal structural pathology that cause lower back pain and radiating pain in the lower extremities.
Material and methods: A retrospective study was performed on 537 patients diagnosed with spinal canal stenosis or disc herniation among patients who underwent selective nerve root block at our hospital for five years from May 2015 to December 2017. The patients were divided into Group A (patients with an only selective spinal nerve root, n=99) and Group B (patients with surgical treatment, n=20). We evaluated the primary demographic factors, including age, sex, onset, symptom duration, diabetes mellitus, hypertension, angina, osteoporosis. The clinical variables included in the analysis were the preoperative visual analog scale (VAS) pain score, the Korean version of the Oswestry Disability Index (K-ODI), and the Roland-Morris disability questionnaire (RMDQ).
Results The average symptom duration was 22.6±1.2 weeks in group A, and 35.7±0.9 in group B. Of a total of 20 patients (16.8%), four males (20%) and 16 females (80%) were underwent surgical procedures because there was no improvement in symptoms. Group B had a significantly higher proportion of female patients and longer symptom duration than group A. And there were no statistically significant differences between groups in other variables.
Conclusions Although the frequency of surgical treatment decreased after selective nerve root block, the longer symptom duration and the female gender might be related to the risk factors for surgical treatment.
Purpose Spinal fusion is useful method of treatment of degenerative lumbar diseases, and is divided into anterior and posterior surgery. Each approach has advangages and disadvantages. Recently, minimally invasive lateral lumbar interbody fusion (LLIF) supplemented disadvantages of anterior and posterior surgery is interested. We introduce LLIF and present about application and indication of LLIF.
Materials and Methods A 76-year-old female was diagnosed by degenerative disc disease on L2-3. A 66-year-old male was diagnosed by central spinal stenosis on L2-3-4-5. A 86-year-old female was diagnosed by foraminal stenosis on L3-4-5 and degenerative scoliosis. A 73-year-old male was diagnosed by spinal stenosis on L3-4-5 and spondylolisthesis. A 70-year-old male was diagnosed nonunion on L4-5. On past history, the patient was operated by fusion because of L2 burst fracture. A 75-year-old female was diagnosed by infective spondylodiscitis on L3-4.
Results Degenerative disc disease, severe central and foraminal spinal stenosis, degenerative scoliosis, spondylolisthesis and infective spondylodiscitis were application and indication of LLIF.
Conclusions LLIF merges the advantages and covers the disadvantages of anterior and posterior surgery. However, approach-related lumbar plexus injury and L5-S1 approach were remained obstacles.
Introduction A spondylitis developed after a surgery has been usually treated with drainage and curettage through anterior approach and autoiliac strut bone graft. However, anterior support with titanium cage combined with posterior pedicle screw fixation has been attempted. Implanting a foreign material is usually prohibited at an active pyogenic infection site. We tried to prove the usefulness of chip bone graft with metal cages in surgical treatment of spondylitis developed in posterior lumbar intebody fusion cases.
Materials and Methods This is a retrospective study. The patients who received posterior lumbar interbody fusion (PLIF) between Jan. 2007 and Dec 2017 and had a spondylitis around the cage were reviewed. There were 1,831 PLIFs during the study period. There were 32 cases of surgical site infection and 20 of them were spondylitis around the cage. Ten out of the 20 cases had a revision surgery. All implants removal, drainage and curettage were done and interbody bone graft and pedicle screw re-fixation was done simultaneously. Five cases used autoiliac strut bone (Group I) and the other 5 cases used titanium cage and autoiliac chip bone (Group II) as interbody graft materials.
The demographic, diagnostic and microbiological characteristics were investigated and the results of treatment were compared between the two groups.
Results The diagnosis of infection was made at 282.0±106.1 (180~410) days in group I and 209±118.4 (75~335) days in group II after the PLIF. All cases had neither general fever nor local manifestations like heating and redness etc.
All patients had back pain, however, only 2 cases of group II had neurological symptoms. C-reactive protein (CRP) level was elevated at 2 weeks from the PLIF in all cases (p<0.001). All cases had implant loosening at the time of their diagnosis. There was no failure of infection control. All cases showed normalization of CRP and radiological interbody fusion. The final Oswestry disability index (ODI) showed no difference between the two groups. ODI improved from 54.6±11.5 to 42.2±6.8 in group I (p=0.095) and from 63.6±6.9 to 44.8±11.7 in group II (p=0.025).
Conclusion For the surgical treatment of spondylitis that were developed in PLIF, a comprehensive one stage operation that comprised all implants removal, drainage and curettage followed by simultaneous intebody bone graft with metal cages and pedicle screw re-fixation was useful to control the infection.
Objective To investigate the association of quantitative paraspinal muscle measurements to the Oswestry disability index (ODI) in patients with lumbar spondylolisthesis.
Materials and Methods Ninety two patients (mean age, 61.6 years; male, mean age, 71.8 years ; female; mean body mass index [BMI], 24.9 kg/m2 ) who had undergone lumbar fusion due to spondylolisthesis with available selfcompleted postoperative ODI were included. The total cross-sectional area (CSA) and functional CSA (FCSA; i.e., area containing only lean muscle tissue) of the paraspinal muscle group (multifidus and erector spinae muscles) and the psoas muscles were measured at L2–L3, L3–L4, and L4–L5 disc levels each on preoperative magnetic resonance imaging (MRI) and the sum of areas at each level served as representative values for each muscle. The FCSA/total CSA ratio and the skeletal muscle index (SMI=muscle area [cm2 ]/patient height2 [m2 ]) were calculated.
Pearson’s correlation analyses were performed to evaluate the relationship between preoperative paraspinal muscle measurements and postoperative ODI.
Results Quantitative values of low paraspinal muscle showed significant correlation with high ODI values. As a result of this study, the preoperative paraspinal muscle was quantified in the group of patients undergoing spinal fusion.
Patients with low value in CSA and FCSA of paraspinal muscle could observe the tendency to transition to low clinical outcomes. Therefore, quantitative values of surrounding muscles are factors affecting clinical outcomes of patients undergoing spinal surgery Conclusion: Smaller muscle bulk (total CSA) of psoas muscles and lean muscle mass (FCSA) of paraspinal muscle group and psoas muscles combined on preoperative MRI were associated with significant postoperative disability based on ODI in patients with lumbar spondylolisthesis.
Numerous improvements in minimally invasive spine surgery (MISS) have been made during the past decade.
Classic treatment methods have reserved surgical intervention for trauma patients with neurological compromises or instability. When used in thoracolumbar spine trauma management, MISS should achieve the similar results as classic treatment with less morbidity.(1) In the past decade, minimally invasive surgical (MIS) techniques for spine surgery have been increasingly used. The goal of minimally invasive surgery is to decrease surgical morbidity through decreased soft-tissue dissection providing similar structural stability as classic techniques. An increasing number of studies is reporting good clinical and radiographic outcomes with MIS techniques. However, the literature is lacking high-quality evidence comparing these newer techniques to classic treatments. In the future, development of techniques can expand the indications and treatment possibilities in spine trauma treatment. We reviewed the current literatures to clarify the indications of minimally invasive techniques with spinal trauma.
Lumbar fusion surgery for lumbar degenerative diseases has increased in the past several decades and many techniques for fusion surgery have been introduced. Recently lateral lumbar interbody fusion with minimally invasive technique was introduced and accepted as a useful method for various lumbar degenerative disease. It can produce good correction for sagittal and coronal imbalance with relatively decreased morbidity. The advantage of lateral lumbar interbody fusion is that it can avoid injury to the abdominal large vessels and neural structures which is more common during posterior approaches. However various complications had been reported. Complications related with lateral lumbar interbody fusion include neurologic complications including thigh pain and numbness, vascular complications including arterial injury, cage related complication such as cage subsidence and vertebral body fractures. Therefore special care should be taken to avoid possible complications in lateral lumbar interbody fusion surgery.
Purpose To evaluate and analyze the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor between recurrence and non-recurrence group, and to assess the merits of minimally invasive spinal surgery.
Overview of Literature: No large registry study has so far investigated the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor.
Methods From July 2003 to April 2011 we retrospectively studied a consecutive series of 156 patients who underwent lumbar microdiscectomy using minimally invasive tubular retractor. The following data were collected: clinical outcomes, operative time, intraoperative blood loss, recurrence, and complications. The clinical outcomes were measured using a visual analog scale (VAS) and assessed by the modified MacNab criteria.
Results Minimally invasive tubular microdiscectomy was performed in 156 patients. The clinical outcomes assessed by MacNab criteria were excellent in 63 patients (40%), good in 71 patients (45%). VAS scores of low-back pain decreased from a mean of 6.7 prior to surgery to 2.5 after surgery, and that of leg pain decreased from 7.2 to 2.1. The average operative time was 68 minutes (range, 25 to 180 minutes). The average blood loss was 42 mL (range, 0 to 500 mL). None of the patients needed blood replacement. One patient had wound infection problem but there was no dural tear case. Twenty-two patients had recurrence. Average time to recurrence was about 42 months. Seventeen cases recurred at the same level and five cases recurred at the adjacent level. Eleven cases in 22 patients with recurrence were contained disc type and the others were non-contained disc type. Eighteen cases in 22 patients with recurrence were paracentral disc herniation type and the others were far lateral type. Average body mass index (BMI) of recurrence cases was 24.7 (range, 17.5 to 31.3) and that of non-recurrence cases was 24.5 (range, 16.3 to 39.2).
Conclusions Lumbar microdiscectomy using tubular retractor can offer a useful modality for the treatment of lumbar herniated disc with the merits of minimally invasive spinal surgery. Further randomized, prospective investigations are needed to fully evaluate the impact of this technique.
Background Context: There are few reports of changes in global sagittal alignment and corresponding factors like hand grip strength (HGS) and muscle performance tests to detect changes in global sagittal alignment after surgery for lumbar spinal stenosis (LSS).
Purpose The purpose of the study was to determine whether HGS can be a useful predictive marker of global sagittal alignment changes after decompression with fusion surgery for LSS.
Study Design: This is a retrospective observational study.
Patient Sample: Patients who underwent spine surgery for LSS were included in the present study.
Outcome Measures: Radiological spinopelvic parameters including sagittal vertical axis (SVA), lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), global tilt (GT), and T1 pelvic angle (T1PA) were assessed. Clinical outcomes parameters like Oswestry Disability Index (ODI), Euro-QOL (EQ-5D), visual analog scale (VAS) scores for back or leg pain were assessed. To assess muscle performance, three functional mobility tests (6-meter walk test, timed up and go test, sit-to-stand test) and HGS were checked.
Materials and Methods A total 91 consecutive patients who underwent spine fusion surgery for LSS were included. 1 year after posterior decompression and fusion surgery, the patients were further classified into four groups according to preoperative and postoperative SVA. We analyzed radiological parameters like SVA, LL, PT, PI, GT, and T1PA. The ODI, the EQ-5D and VAS scores for back or leg pain were recorded as clinical outcomes assessment. To assess muscle performance, SMT, TUGT, STS, and HGS were checked.
Results HGS was significantly correlated with age, postoperative SVA, ODI, EQ-5D and muscle performance test. HGS was related with change of preoperative sagittal alignment 1yr after surgery. Using a receiver operating characteristic (ROC) curve to determine the cutoff values of HGS as predictors of postoperative balanced sagittal alignment according to SVA, cutoff value of HGS demonstrated 19.5 kg with a sensitivity of 82.1% and specificity of 66.7%.
Conclusion Patients with non-balanced sagittal alignment in LSS demonstrated decreased muscle function and muscle strength. If the muscle strength was weak in the group in which the sagittal balance was maintained preoperatively, it could be converted to non-balanced sagittal alignment. Thus, preoperative HGS may be a good predictor of postoperative SVA change.
Purpose of Study: Purpose of this study is to summarize the technique of UBE surgery in lumbar interbody fusion and review the clinical outcomes and complications of UBE surgery in lumbar interbody fusion.
Materials and Methods Medical databases were searched for the key words of unilateral biportal endoscopic surgery and lumbar spinal stenosis using PubMed from 2005 to the present.
Conclusion UBE spinal surgery is a new technique that can be a feasible alternative and an effective treatment modality for spinal degenerative diseases and can achieve the necessary surgical skills for experienced microscopic surgeons, which is still expanding the indications for lumbar spinal surgery.
Objectives We report the new minimally invasive technique and its clinical results of oblique lumbar interbody fusion (OLIF) combined with central decompression using biportal endoscopic spinal surgery (BESS).
Summary of Literature Review: The OLIF procedure is one of the minimally invasive spine surgeries and is being frequently attempted recently to treat lumbar degenerative disease. It has been reported that it effectively decompresses foraminal stenotic lesions indirectly by inserting a large cage anteriorly, which reduces spondylolisthesis and widens the disc space. However, OLIF has limited effect for severe central canal stenosis, since it cannot achieve direct decompression. Therefore, authors report a new minimally invasive technique of OLIF combined with direct central decompression using BESS for severe central stenosis along with its clinical results as a pilot study.
Materials and Methods For patients who were candidate for fusion surgery due to spondylolisthesis (more than one segment) or foraminal stenosis, authors performed OLIF and central decompression using BESS simultaneously, when the patients had concomitant severe central canal stenosis. From June to December, 2017, 8 patients (16 levels) were enrolled, the operative time, blood loss, complications and clinical results have been evaluated. The clinical results were analyzed by Visual analog scale (VAS) scores, Oswestry disability index (ODI) and Roland Morris Disability Questionnaire (RMDQ) of preoperative, 1month, 3month postoperative and final follow-up.
Results Mean operative time and blood loss were 238.4 minutes and 173.3ml, respectively. In all cases, there were no operative complications, and mean follow-up period was 7.1 months. The mean back VAS, lower extremity VAS, ODI, and RMDQ at the final follow-up were improved from 5.4±2.4 to 2.0±0.9, 7.0±1.1 to 1.6±1.7, 64.2±11.8 to 44.2±10.6, and from 17.5±4.2 to 12.9±4.0.
Conclusion A new combination technique of OLIF and BESS for direct decompression can be regarded as effective alternative procedure to treat the foraminal and central stenotic lesions of lumbar degenerative disease.
The foramen of L5-S1 can develop several degenerative diseases such as extraforaminal lumbar disc herniation, foraminal stenosis with disc height collapse, degenerative or spondylolytic spondylolisthesis, and far-out syndrome.
The floating technique in biportal endoscopic spine surgery (BESS) keeps a certain distance between instruments and spinal structures. 1) This key point makes the floating technique different from conventional endoscopic surgery, which uses the Kambin’s safe triangle as a work zone. The floating view can enable the surgeon to see the structures panoramically, under high magnification: consequently, fine discrimination of their margin and safe manipulation of neural structures can be guaranteed. A certain gap between the floating scope and lesion can permit various instruments, generally used in open spine surgery, to be inserted from the sides with fewer limitations. Extraforaminal or foraminal lesions under the lamina can be reached by avoiding the iliac crest, and total facetectomy, which has the potential of iatrogenic instability, is not required to explore the foraminal structures. However, the floating view can be obstructed by small bleeds from laminectomized bone and/or surrounding vessels. This present article describes the technique and provides tips on how to perform BESS with floating technique safely and successfully for various lesions at the L5-S1 foramen.
Many techniques have been introduced and performed, with different strengths and benefits. The lateral lumbar interbody fusion techniques (direct lateral lumbar interbody fusion [DLIF] and oblique lateral interbody fusion [OLIF]) have yielded good results for elderly patients. These are useful options for elderly patients with high risk of complications with traditional approaches.
A 77-year-old female suffering from severe degenerative scoliosis, spinal stenosis and lumbar disc herniation underwent Direct lateral lumbar interbody fusion (DLIF) at L2-4. On the 3rd postoperative day, she complained of severe back pain without any trauma history. Simple radiograph revealed L3 vertebral fracture and cage subsidence.
Pain was subsided after conservative treatment including TLSO and medication. Radiographic union was achieved at fractured vertebra after 3 months. Solid fusion was observed at operated level after 6 months. Patient has visited our clinic without any pain. DLIF is one of novel minimally invasive spine procedures available today. It is designed to maximize benefits and minimize risks of other traditional techniques such as anterior approach and posterior approach. However, there can be some risk of cage subsidence and vertebral fracture after DLIF. Therefore, care should be taken to avoid cage subsidence during the operation.
Minimally invasive TLIF has been reported to be a useful treatment option for the patients with various degenerative lumbar diseases. Many studies have reported the favorable clinical results of MIS TLIF. However it remains technically demanding, leading to higher complication rates and longer operative times during the early period of the learning curve. It showed some potential complications due to small working space and visual field. In this study, authors tried to find out various possible complications and some tips avoiding these complications through the review of various articles and authors’ clinical experiences. In many studies, the general complication fusion rates of MIS TLIF have been reported to be similar to that of open fusion. The technical difficulty of the procedure, combined with inadequate training, is evident in initial studies of MIS TLIF. A difficult learning curve of MIS TLIF demands that surgeons have sufficient preclinical training, and education is obtained before the application of MIS TLIF in clinical practice.
Purpose The purpose of this study was to determine the early failure rate of percutaneous epidural neuroplasty (PEN) that led to subsequent decompressive lumbar surgery. We also assessed the limits of spinal pain management by using the current PEN technique.
Materials and Methods We classified 1763 cases according to their diagnoses and radiological findings. Patients who underwent subsequent open surgery when PEN failed to improve or aggravated their symptoms were included.
Results All 37 patients underwent open decompressive surgery within 3 months after PEN. There were 18 in the intracanalicular focal herniation category, 11 in intracanalicular broad based herniation category, and 8 in foraminal category; the early failure rates were 1.7%, 1.9%, and 5.6%, respectively. There was no significant statistical difference between the intracanalicular categories with regard to failure rate, but the foraminal category had a higher rate of failure than that of intracanalicular categories (p<0.05). Moreover, there were 11 cases in intracanalicular categories that experienced deterioration or new symptoms due to posterior longitudinal ligament rupture or fragment migration. Among these, there were 9 cases (82%) with preexisting intracanalicular migrating fragments.
Conclusion PEN with targeted drug delivery may be an effective treatment for low back pain and/or radiculopathy.
However, its early failure rate is at least 2.1%, and the presence of intracanalicular migrating fragments or symptomatic foraminal lesions are predictors of poor outcome. Patients must be carefully selected on the basis of thorough radiologic reviews to improve the rate of satisfactory PEN outcomes.
Purpose Pull-out of pedicle screw in posterior pedicle fixation for thoracic and lumbar burst fractures causes delayed rehabilitation, persistant pain, and imblance of sagittal plane. In this study we try to analyse the factors that cause the pull-out of pedicle screw.
Materials and Methods From March 01, 2006 to December 31, 2009, we assorted into two group; Group I for pullout pedicle, Group II for control. Plane lateral x-ray view film of thoracolumbar spine was taken on preoperation, postoperation, the first time when screw was pulled out and last follow up. we measure inserted angle for the upper endplate of screw, convergency angle and change of body height loss and kyphotic angle. We analysed corelation between these measuring values and pedicle screw pull-out by Mann-Whitney test and T-test.
Results Pull-out of pedicle screw was found at mean 5weeks among nine cases. For inserted pedicle screws, which place in upper and lower vertebral body of fractured one, Value of inserted angle for upper end plate and convergency angle was found non-significant(p>0.05, Mann-Whitney test). Restoration of height loss and kyphotic angle of fractured vertebral body was statically significant(p<0.05, T-test).
Conclusion In posterior pedicle fixation for thoracic and lumbar burst fractures, sufficient restoration of height loss and kyphotic angle is important factor for prevention of screw pull-out than inserted angle for upper end plate and convergency angle at a short period of time. Therefore we think that sufficient anterior fixation of vertebral body and restoration of kyphotic angle have a decisive effect on prognosis of patients.
Injection therapy is a major component of conservative management for spinal disorders like herniated nucleus pulposus (HNP) and spinal stenosis. The most common problem faced during the injection – transforaminal, interlaminar or caudal epidural block is delivering the drug at the exact site of lesion due to adhesions more so when there has been a previous open spinal surgery. Conventional neurolysis effect was limited because adhesiolysis and drug delivery were in the posterior epidural space. So, we report a simple neurolysis technique which can inject drugs directly to nerve roots and intervertebral discs at anterior epidural space through the caudal approach using conventional neurolysis devices.
Purpose To assess the volume of fusion mass after posterior lumbar interbody fusion (PLIF) using Hounsfield units methods.
Methods The present study was within the frame work about a prospective observational cohort study to compare the surgical outcomes of a single-level PLIF for LSS between the local bone (LbG) and local bone plus hydroxyapatite groups (LbHa). The fusion material for each case was determined by the amount of available local bone. After the fusion material was chosen, patients were assigned to either the LbG group (n=20) or the LbHa group (n=20). The primary outcome was the assessment of fusion mass volume in each group.
Results We used the new method using Hounsfield units for volumetric assessments of interbody fusion mass. There was no difference in fusion rates or volume of the fusion mass between the 2 groups.
Conclusions Hounsfield unit method, that is the CT-based summation method using a cross-sectional slice, can be applied usefully to other areas of orthopaedics.
Purpose To evaluate the method of inserting cortical bone trajectory pedicle screws (cortical screws) and potential complications when performing lumbar fusion.
Methods Lumbar fusion with cortical screw fixation in the hard cortical bone of the pars interarticularis of vertebrae was introduced to replace conventional pedicle screws. We review the literature on the biomechanics of cortical screw insertion and on the clinical outcomes.
Results In vitro biomechanical testing has shown that cortical screws have greater pullout strength than traditional pedicle screws due to the strong bone–screw interface in cortical bone. Cortical screws have the advantages of requiring minimal muscle dissection and shortening the surgery. However, early screw loosening and loss of reduction have been reported.
Conclusions When inserting cortical screws, the entry point and trajectory of the screws are important and a meticulous surgical technique is needed to prevent potential screw-related complications.
Purpose To analyze the serial changes of the lumbar sagittal alignment from preop. to final follow-up and to evaluate the role of the posterior spinal instrumentation, especially, short level fusion in correction and maintenance of the lumbar sagittal alignment in degenerative lumbar disease.
Materials and Methods Various lumbar sagittal profiles such as lumbar lordosis(LL), lordosis above, within and below instrumentation(LAI, LWI, LBI), horizontal vertebra and sacral inclination were serially measured in 54 patients whose radiographs at preop., intraop., immed. postop. postop. 2wks and final follow up(>1 yr) were completely equipped.
Results Intraop. posture, instrumentation itself and interbody fusion could not increase the LL and LWI sufficiently irrespective of the length of fixation. LWI was decreased compared with preop. values irrespective of length of fixation, while interbody fusion has a great role in maintaining the LWI. Loss of LWI was overcompensated at the segments above instrumentation in 1 or 2 levels fixation while compensation has not occurred in longer fixations.
Conclusions The longer the fixation, the more correction could be obtained. However, maintenance of this correction is more difficult in longer fixations. Prudent consideration should be taken in restoring sufficient lumbar lordosis and maintenance for favorable long term results.
Purpose of study: The purpose of this study is to understand the biomechanics of interspinous devices in lumbar spinal surgery and to review the effectiveness of the devices for lumbar spinal stenosis through recent related articles.
Materials and Methods Medical databases were searched for the key words of interspinous device and lumbar spinal stenosis using PubMed from 2010 to the present.
Results Several studies have shown sustained symptomatic improvements after interspinous device insertion.
However, most of the prospective, randomized, double-blinded studies have shown that it is not superior to conventional laminectomy from a statistical perspective. Furthermore, interspinous device insertion has been shown to have a higher reoperation rate and to be less cost effective.
Conclusions A large prospective cohort study with a longer follow-up period comparing decompressive surgery alone versus interspinous device insertion for the treatment of lumbar spinal stenosis is needed to conclusively determine whether the interspinous device is beneficial.
Introducing a 61-year old woman who was suffering from complicated traumatic thoracolumbar spine fractures, we contemplated the appropriate management algorithm. The Thoracolumbar Injury Classification and Severity score (TLICS) system is the latest and widely used scoring system by spine surgeons for thoracolumbar injuries (TLI). The originator of the system claims for easy application, high reproducibility, and direct link to a clinical decision-making algorithm. However, because of its simple and narrow boundaries, there are many limitations to apply the system in complicated situations. Besides, a fair number of TLI are caused by high velocity traumas, which mostly lead to complicated fractures and other medical conditions. For these reasons, practically, we also consider traditional and former concepts of TLI classifications. Furthermore, new algorithm should be suggested which includes not only the spine morphology and neurological manifestation but also comprehensive medical considerations of the patient.
Since its introduction in 1980s, Laser therapy, a minimally invasive, outpatient, effective, and relatively safe procedure for spine disease, has established itself world-wide. percutaneous laser disc decompression (PLDD) was mainly applied to treat lumbar disc herniation with a satisfactory efficacy. Recently, laser therapy has been used for many cases of lumbar stenosis and cervical disease.In this article, advantages and disadvantages of laser will be discussed, and technical and clinical aspects of current applications will presented. Such applications include Percutaneous lumbar disk decompression (PLDD), Percutaneous endoscopic laser annuloplasty(PELA), Epiduroscopic laser neural decompression(ELND), Laser disk decompression in cervical disk diseases.
Objectives The aim of this study was to monitor the quality control of pedicle screw fixation using a cumulative summation test (CUSUM).
Overview of Literature: CUSUM test has already been used in several different surgical settings including the assessment of outcomes in transplant, laparoscopic, and total hip replacement surgeries. However, there has been no data regarding CUSUM analysis for spine surgery.
Methods Patients with lumbar spinal stenosis who underwent lumbar fusion surgery were included in this study.
The primary outcome was the CUSUM analysis for monitoring the quality control of the accuracy of pedicle screw insertion.
Results Seven screws of the 100 pedicle screw insertions were considered to have failed in the lumbar fusion surgery, respectively. Throughout the monitoring period, there was no indication by the CUSUM test that the quality of performance of the pedicle screw fixation procedure was inadequate.
Conclusions Thisstudy demonstrates the CUSUM test can be a useful tool for monitoring of the quality of procedures related with spine surgery.
Far lateral lumbar disc herniation (FLLDH) is a rare type of intervertebral disc herniations based on its anatomical location. A herniated lesion compressing the exiting nerve root superiorly makes clinical symptoms of lumbar radiculopathy. We report a 77-year-old female patient presenting lower back pain, left buttock pain and numbness, radiating pain, tingling sensation on the left lower extremity. Radiological images revealed a 16.2x13.8x7.2 mm sized mass like lesion outside the left foraminal canal of the L5-S1 disc space, mimicking nerve sheath tumor at a extradural location. Histopathological examination of the specimen was confirmed as a sequestrated disc fragments.
We conclude that preoperative careful evaluation should be exercised for the differential diagnosis of the extraforaminal soft mass.

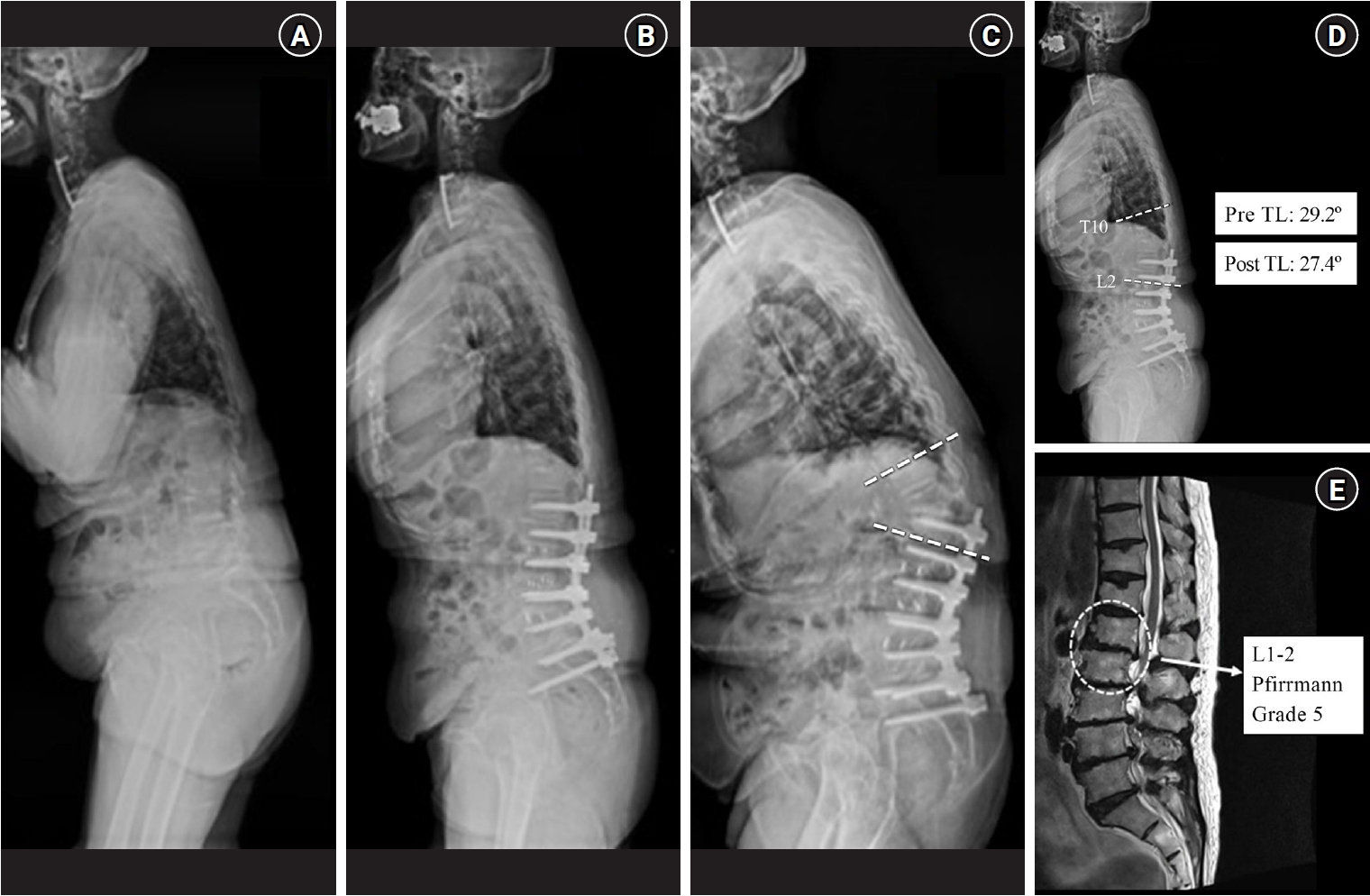
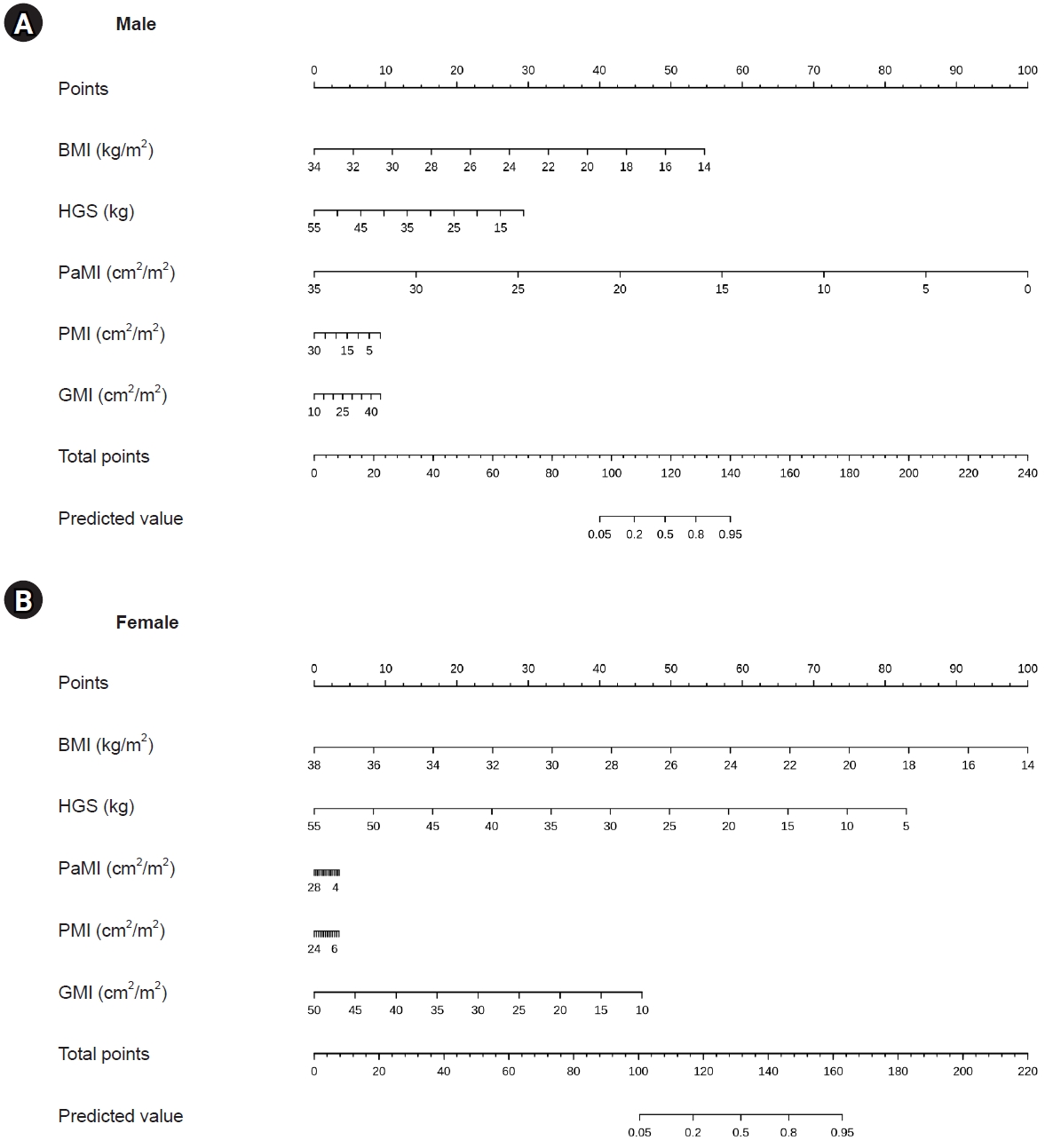
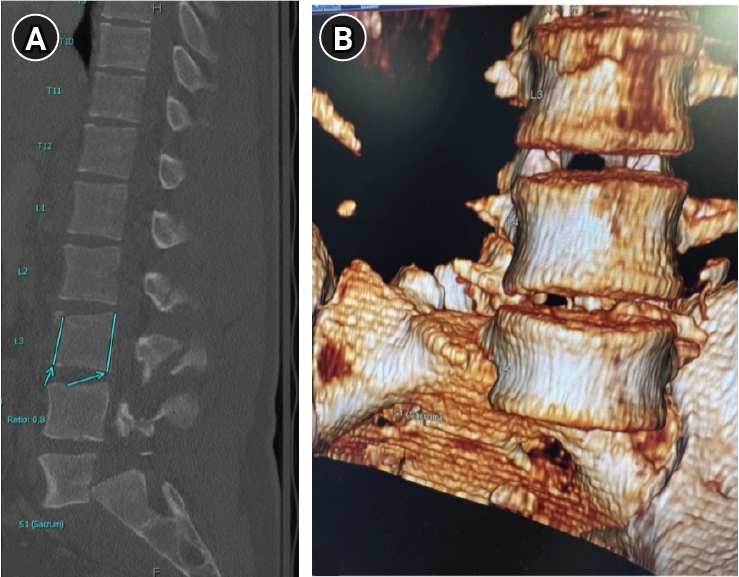
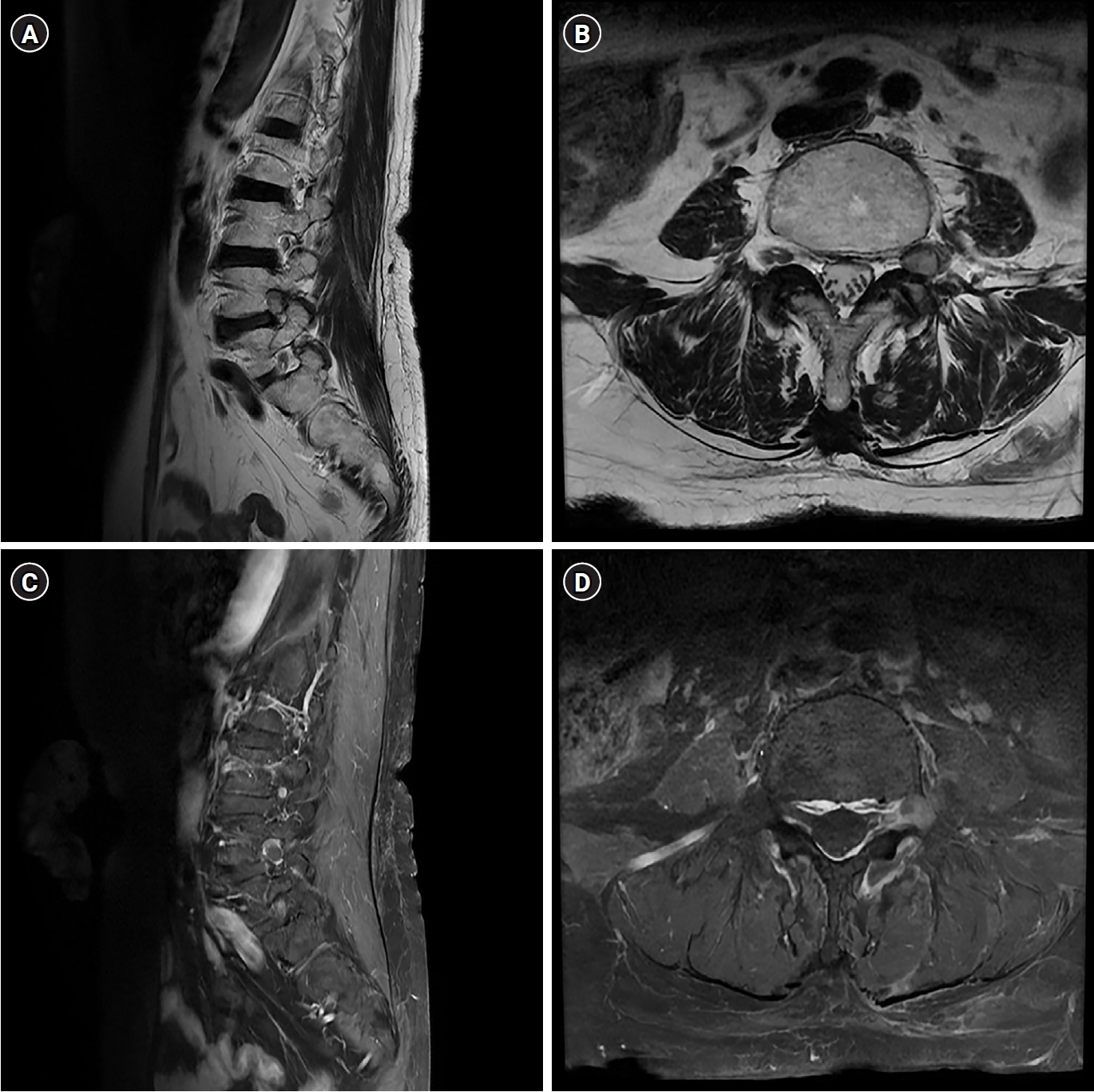
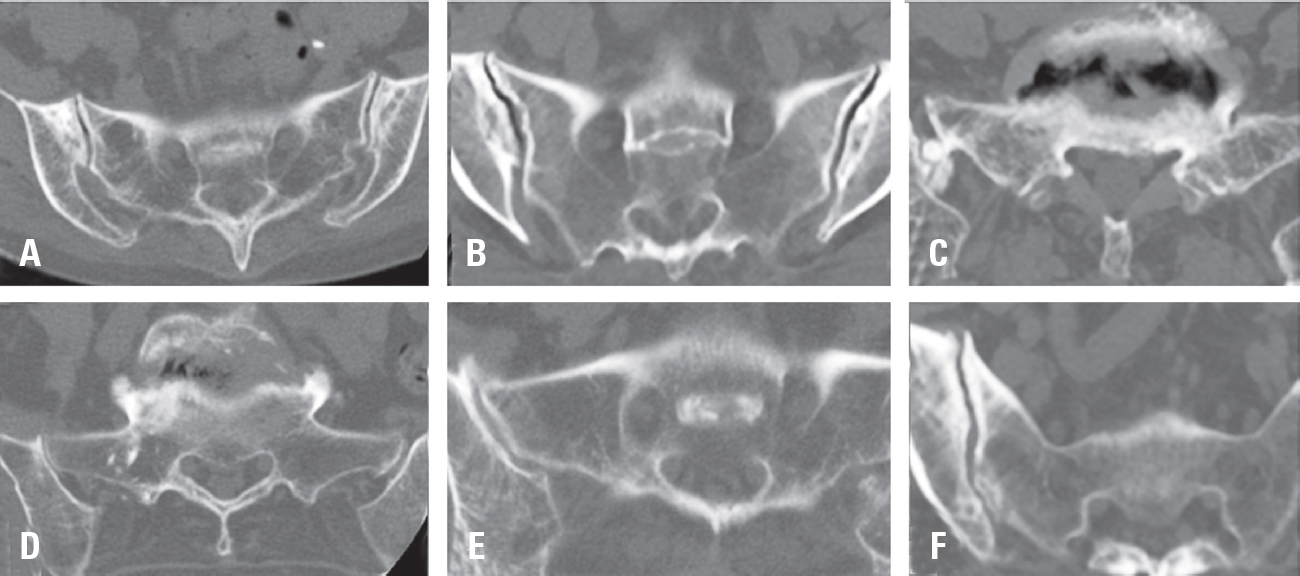
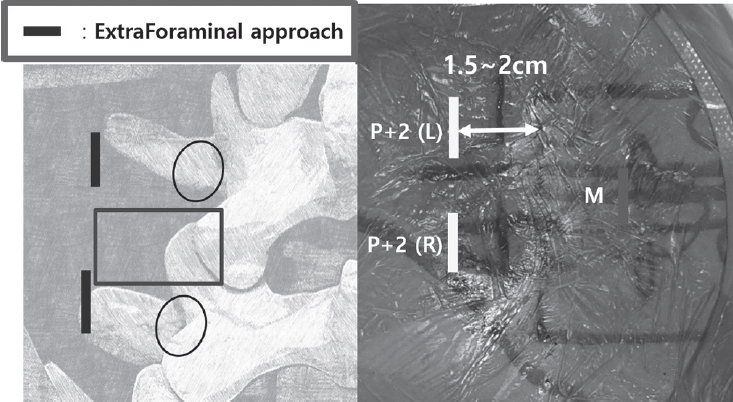
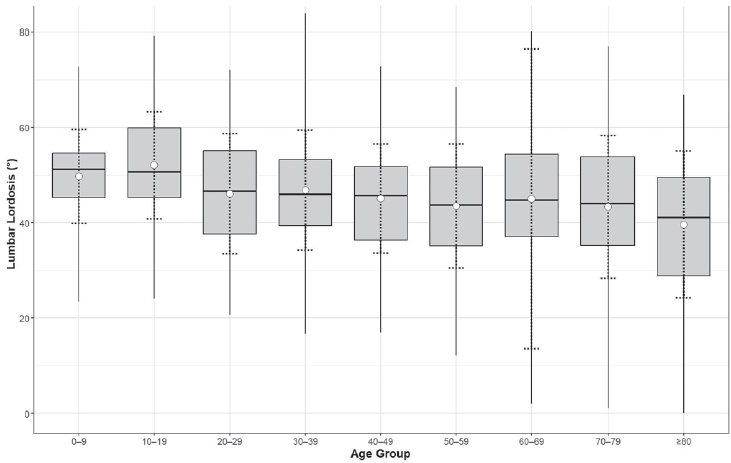
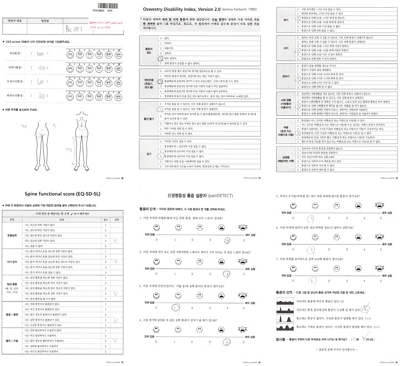
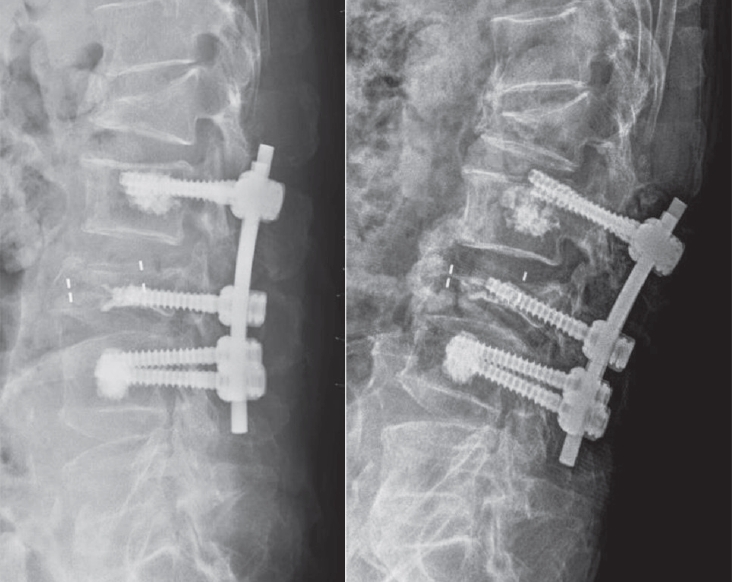
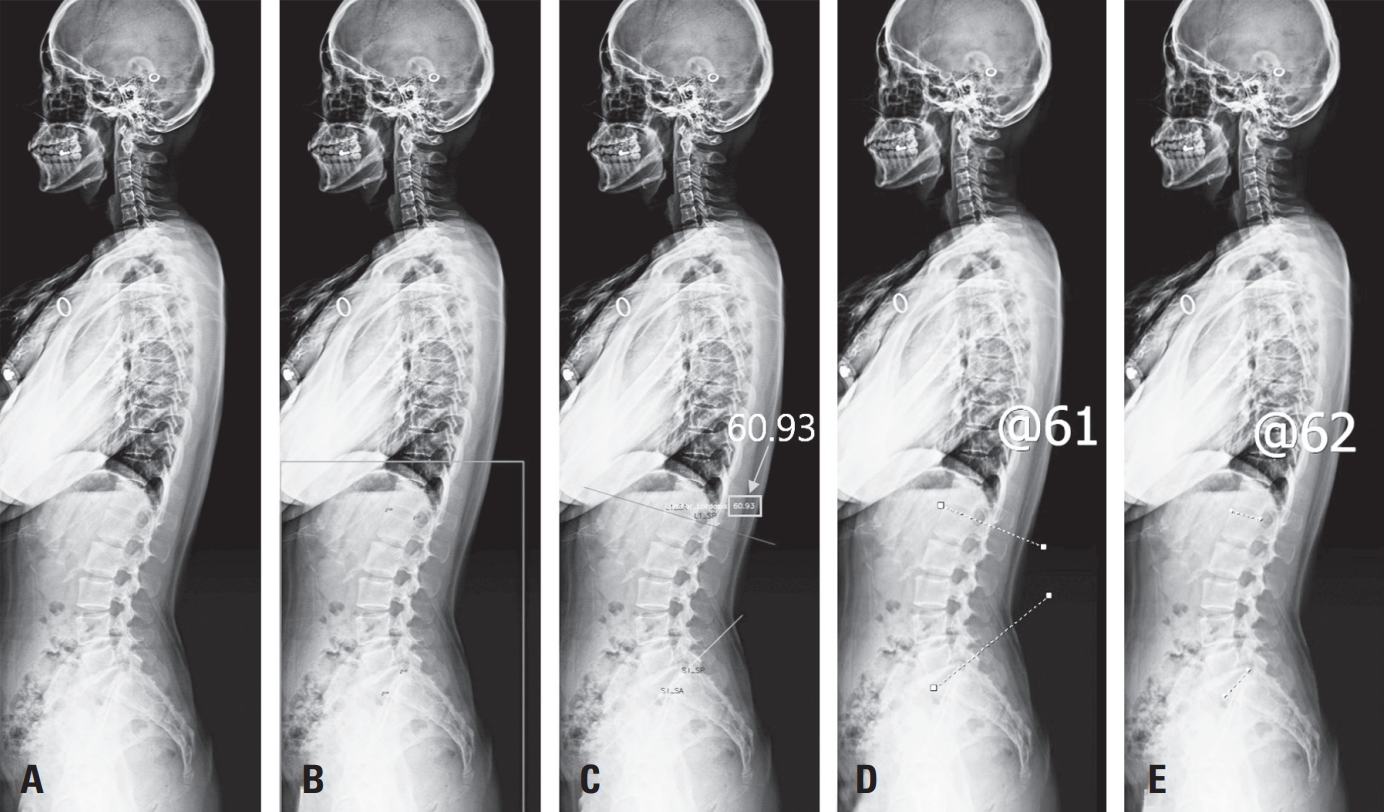
 First
First Prev
Prev

