Purpose To evaluate the association between lumbar lordosis and age using an AI-based automated measurement model applied to a large dataset of standing lateral spinal radiographs.
Materials and Methods This retrospective study analyzed 904 high-quality radiographs selected from 2,397 images acquired between 2019 and 2021. Lumbar lordosis was defined as the angle between the superior endplates of L1 and S1 and automatically measured using a validated deep learning model. Subjects were categorized into nine age groups. One-way ANOVA compared lumbar lordosis across age groups, and Pearson correlation assessed the relationship between age and lumbar lordosis.
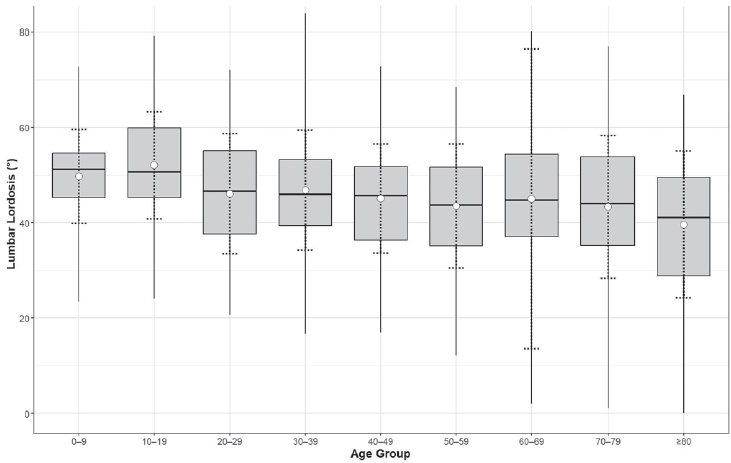
Results Lumbar lordosis ranged from 0° to 84° (mean 45.9°±13.4°). The highest mean value was in the 10–19-year group (52.1°), and the lowest in the ≥80-year group (39.6°). Minimum values decreased to 0° in individuals aged ≥60 years. No significant differences were found across age groups (p=0.561). A weak but significant negative correlation was observed between age and lumbar lordosis (r=–0.247, p<0.0001).
Conclusions AI-based automated measurement enabled efficient large-scale analysis and revealed a wide distribution of lumbar lordosis with a gradual age-related decline. These findings highlight the value of AI in spinal alignment assessment.
Purpose To develop and validate a deep learning–based artificial intelligence (AI) model for automated measurement of lumbar lordosis (LL) angles from whole spine lateral radiographs.
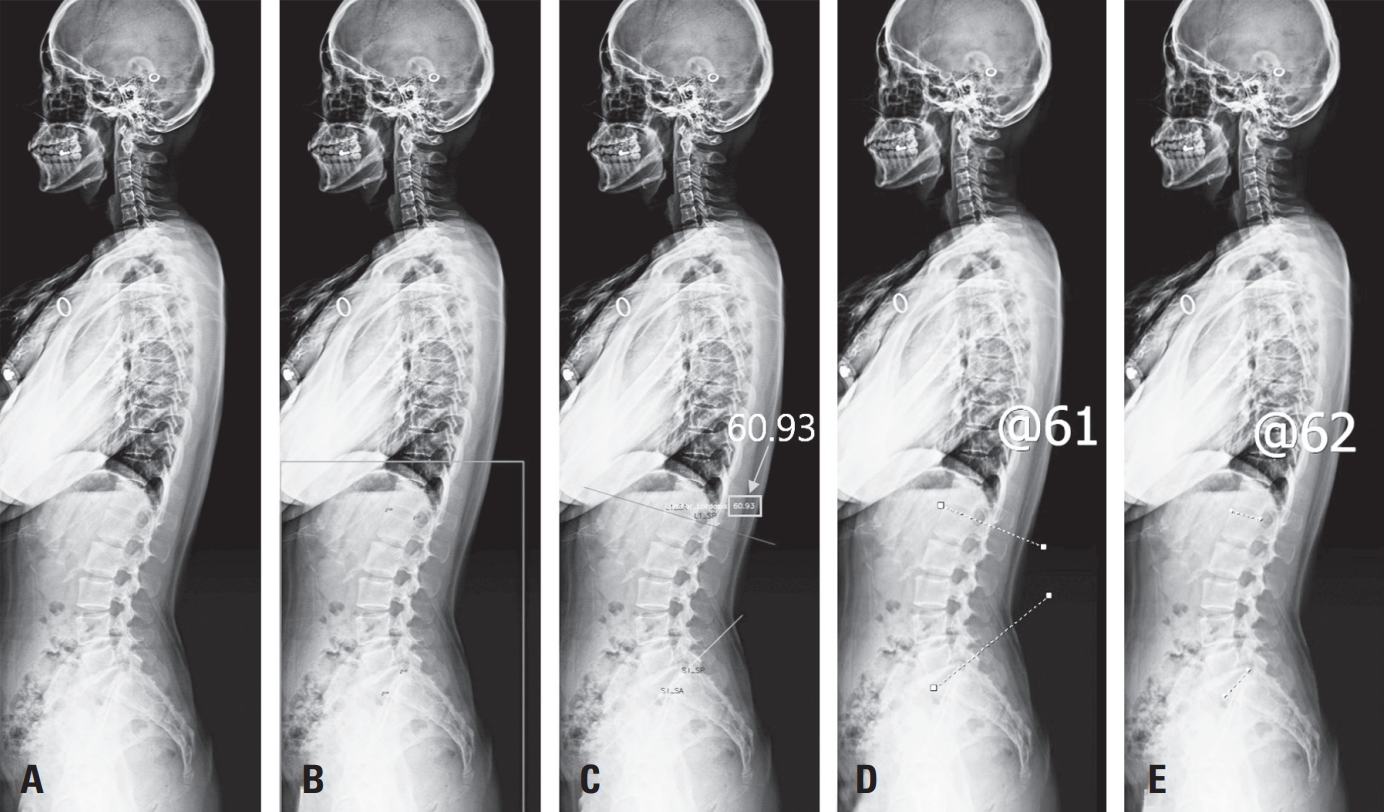
Materials and Methods A total of 888 lateral spine X-rays (2019–2021) were retrospectively collected and annotated with four anatomical keypoints (L1 and S1 vertebral landmarks). An AI model using Detectron2 with a Keypoint R-CNN and ResNeXt-101 backbone was trained with data augmentation. Performance was evaluated on 50 test images, comparing AI results to manual annotations by two orthopedic surgeons using intraclass correlation coefficient (ICC), Pearson’s correlation, and Bland–Altman analysis.
Results The model achieved an average precision of 71.63 for bounding boxes and 86.61 for keypoints. ICCs between AI and human raters ranged from 0.918 to 0.962. Pearson correlation coefficients were r=0.849 and r=0.903. Bland–Altman analysis showed minor underestimation biases (–3.42° and –4.28°) with acceptable agreement.
Conclusions The AI model showed excellent agreement with expert measurements and high reliability in LL angle assessment. Despite a slight underestimation, it offers a scalable, consistent tool for clinical use. Further studies should evaluate generalizability and interpretability in broader settings.
Citations
Citations to this article as recorded by
Deep Learning–based AI Analysis of the Correlation Between Lumbar Lordosis and Age Soo-Bin Lee, Ja-Yeong Yoon, Dong-Sik Chae, Sang-Bum Kim, Young-Seo Park, Kyung-Yil Kang, Min-Kyu Lee Journal of Advanced Spine Surgery.2025; 15(2): 78. CrossRef
Efficacy of Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Meta-Analysis With Single-Arm Analysis and Comparative Analysis With Microscopic Decompression and Uniportal Endoscopic Decompression Shuangwen Lv, Haiwen Lv, Yupeng He, Xiansheng Xia Operative Neurosurgery.2024; 27(2): 158. CrossRef
Background It is well reported that the patient’s age plays an important role associated with proximal junctional failure (PJF) development. Various characteristics of adult spinal deformity (ASD) patients were different between younger and older age groups. We hypothesized that the radiographic risk factors for PJF would different according to younger and older age groups. This study aimed to evaluate different radiographic risk factor of PJF according to the two age groups undergoing thoracolumbar fusion for ASD.
Methods ASD patients aged ≥ 60 years who underwent thoracolumbar fusion from low thoracic level (T9~T12) to sacrum were included. The minimum follow-up duration was two years. PJF was defined as proximal junctional angle (PJA) ≥ 20°, fixation failure, fracture, myelopathy, or necessity of revision surgery. Using various radiographic risk factors including age-adjusted ideal pelvic incidence (PI)-lumbar lordosis (LL), univariate and multivariate analyses were performed separately according to the two age groups : <70 years and ≥70 years.
Results A total of 186 patients were enrolled (mean age=68.5 years old, 90.3% female). Mean follow-up duration was 67.4 months. PJF developed in 98 patients (32.0%). There were fracture in 53 patients, PJA ≥ 20° in 26, fixation failure in 12, and myelopathy in 6. PJF developed more frequently in patients older than 70 years than in younger than 70 years. In patients aged less than 70 years, preoperative LL, PI-LL and change in LL were significant risk factors in univariate analysis. Multivariate analysis showed only change in LL was significant for PJF development (Odds ratio [OR]=1.025, p=0.021). On the other hand, in patients older than 70 years, postoperative LL, postoperative PILL, overcorrection relative to conventional PI-LL target (within ±10°) as well as age-adjusted ideal PI-LL target were significant. On multivariate analysis, only overcorrection of PI-LL relative to age-adjusted ideal target was a single significant factor to cause PJF (OR=5.250, p=0.024).
Conclusions In patients younger than 70 years, greater change in LL was associated with PJF development regardless of PI-related value. However, in older patients, overcorrection of PI-LL relative to the age-adjusted PI-LL target was important to cause PJF.
Purpose To analyze the serial changes of the lumbar sagittal alignment from preop. to final follow-up and to evaluate the role of the posterior spinal instrumentation, especially, short level fusion in correction and maintenance of the lumbar sagittal alignment in degenerative lumbar disease.
Materials and Methods Various lumbar sagittal profiles such as lumbar lordosis(LL), lordosis above, within and below instrumentation(LAI, LWI, LBI), horizontal vertebra and sacral inclination were serially measured in 54 patients whose radiographs at preop., intraop., immed. postop. postop. 2wks and final follow up(>1 yr) were completely equipped.
Results Intraop. posture, instrumentation itself and interbody fusion could not increase the LL and LWI sufficiently irrespective of the length of fixation. LWI was decreased compared with preop. values irrespective of length of fixation, while interbody fusion has a great role in maintaining the LWI. Loss of LWI was overcompensated at the segments above instrumentation in 1 or 2 levels fixation while compensation has not occurred in longer fixations.
Conclusions The longer the fixation, the more correction could be obtained. However, maintenance of this correction is more difficult in longer fixations. Prudent consideration should be taken in restoring sufficient lumbar lordosis and maintenance for favorable long term results.
In patient with loss of lumbar lordosis, lumbar lordosis restoration is very important to get a normal sagittal balance. It is difficult to know the ideal lumbar lordosis, because it is a individual-unique pattern and is influenced by numerous variables. To restore a more ideal lumbar lordosis, careful analysis and planning will be needed because incomplete restoration of lumbar lordosis may result in poor clinical outcomes and serious complications.
Lumbar lordosis has strong relationship with pelvic orientation, so there are many reports about predictive equation of lumbar lordosis using pelvic parameters. Pelvic incidence is major determinant of pelvic orientation, therefore, influence on lumbar lordosis. So pelvic incidence is a useful value to determine the ideal lumbar lordosis, and we recommend that the degree of restoration of lumbar lordosis is just enough to pelvic incidence at least. And also, a close study and understanding of the numerous factors affecting lumbar lordosis was needed to effective lumbar lordosis restoration.

 First
First Prev
Prev

