Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
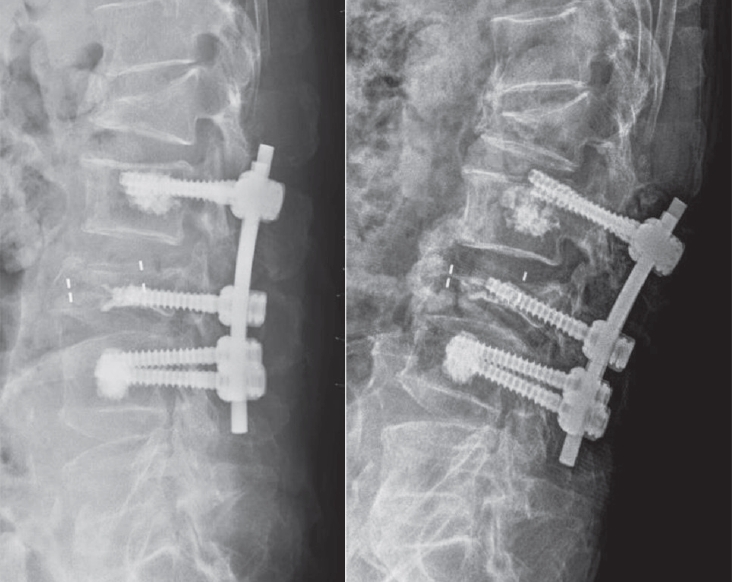
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
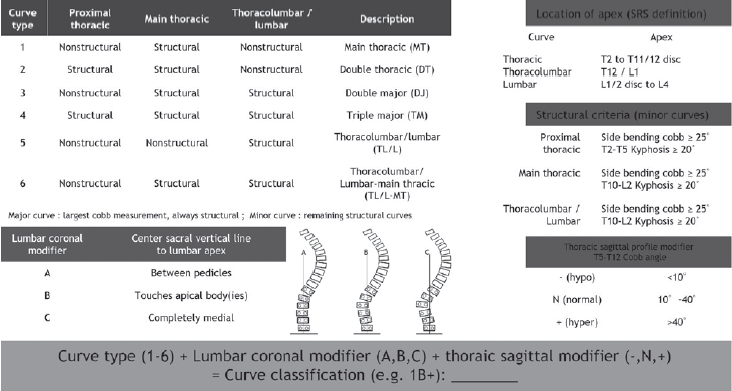
Adolescent idiopathic scoliosis refers to spinal deformity that develops from just before the onset of puberty until the completion of skeletal growth, and the primary goal of treatment is to achieve a well-balanced spine. In the late 1990s, advances in the anatomical understanding of the spine and the development of fixation instruments made posterior pedicle screw insertion feasible, thereby enabling the transmission of powerful corrective forces for deformity correction. Over the subsequent decades, accumulated clinical experience and outcomes have provided a deeper understanding of scoliotic curves and led to the establishment of effective principles for determining the extent of spinal fusion. However, these treatment principles are based on the unique biomechanics and procedural characteristics of scoliosis correction surgery, which can make them difficult to understand without sufficient explanation. In this review, we aim to describe these established treatment principles and surgical processes in detail using schematic illustrations and images. Although these principles will continue to undergo new challenges and validation over time, they will remain a meaningful reference point for those exploring alternative strategies.
Objectives The primary surgical goals when treating a spinal metastasis are usually pain relief and preservation of ambulatory function. Minimally invasive techniques have become popular, being associated with less morbidity and mortality than conventional open surgeries.
Materials and Methods Between April 2012 and September 2016, 15 consecutive patients underwent percutaneous pedicle screw fixation (PPSF) to treat spinal metastases. We retrospectively analyzed prospectively collected data, including visual analog scale (VAS) pain scores, Frankel scale scores, and complications.
Results Fifteen patients (8 males, 7 females; mean age 61 years) underwent surgery under general anesthesia. PPSF was performed on all patients, and two with poor bone quality underwent cement augmentation of the manipulated vertebra(e) just prior to pedicle screw insertion. Seven patients underwent fixation plus distraction (indirect decompression via ligamentotaxis) and two laminectomies (direct decompression) of the spinal cord. Two patients developed screw pullout requiring revision surgery. One patient died 7 days after surgery from liver cirrhosis and sepsis. All patients reported that pain was reduced after surgery. After surgery, 12 patients regained ambulatory capacity. Nine patients died during follow-up; the mean overall survival time was 14.1 months.
Conclusions PPSF is a safe and minimally invasive palliative surgery option for patients with spinal metastases.
Purpose Pull-out of pedicle screw in posterior pedicle fixation for thoracic and lumbar burst fractures causes delayed rehabilitation, persistant pain, and imblance of sagittal plane. In this study we try to analyse the factors that cause the pull-out of pedicle screw.
Materials and Methods From March 01, 2006 to December 31, 2009, we assorted into two group; Group I for pullout pedicle, Group II for control. Plane lateral x-ray view film of thoracolumbar spine was taken on preoperation, postoperation, the first time when screw was pulled out and last follow up. we measure inserted angle for the upper endplate of screw, convergency angle and change of body height loss and kyphotic angle. We analysed corelation between these measuring values and pedicle screw pull-out by Mann-Whitney test and T-test.
Results Pull-out of pedicle screw was found at mean 5weeks among nine cases. For inserted pedicle screws, which place in upper and lower vertebral body of fractured one, Value of inserted angle for upper end plate and convergency angle was found non-significant(p>0.05, Mann-Whitney test). Restoration of height loss and kyphotic angle of fractured vertebral body was statically significant(p<0.05, T-test).
Conclusion In posterior pedicle fixation for thoracic and lumbar burst fractures, sufficient restoration of height loss and kyphotic angle is important factor for prevention of screw pull-out than inserted angle for upper end plate and convergency angle at a short period of time. Therefore we think that sufficient anterior fixation of vertebral body and restoration of kyphotic angle have a decisive effect on prognosis of patients.
Purpose To evaluate the method of inserting cortical bone trajectory pedicle screws (cortical screws) and potential complications when performing lumbar fusion.
Methods Lumbar fusion with cortical screw fixation in the hard cortical bone of the pars interarticularis of vertebrae was introduced to replace conventional pedicle screws. We review the literature on the biomechanics of cortical screw insertion and on the clinical outcomes.
Results In vitro biomechanical testing has shown that cortical screws have greater pullout strength than traditional pedicle screws due to the strong bone–screw interface in cortical bone. Cortical screws have the advantages of requiring minimal muscle dissection and shortening the surgery. However, early screw loosening and loss of reduction have been reported.
Conclusions When inserting cortical screws, the entry point and trajectory of the screws are important and a meticulous surgical technique is needed to prevent potential screw-related complications.
Purpose The purpose of the study was to investigate the effect of obesity on the accuracy of percutaneous pedicle screw placement.
Materials and Methods We performed a retrospective analysis on the first 89 patients undergoing minimally invasive lumbar fusion with percutaneous pedicle screw placements for the treatment of degenerative lumbar spinal disorder.
Based on patient’s body mass index (BMI), patients were divided into 3 groups: group 1 – normal weight (BMI<25, 38 patients, 157 screws); group 2 – overweight (25≤BMI<30, 29 patients, 124 screws); group 3 – obese (BMI≥30, 22 patients, 89 screws). Using postoperative computed tomography (CT) scans, the position of placed screws to the pedicle or anterior body perforation was evaluated using the following grading method: Grade A, completely in the range without pedicle cortex violation; Grade B, pedicle wall violation<2 mm; Grade C, pedicle wall violation 2 to 4 mm; and Grade D, pedicle wall violation>4 mm.
Results Among the 370 pedicle screws, 308 screws (83%) were perfectly placed within the pedicle. Among the 62 misplaced screws, 45 screws were grade B pedicle breaches (73%, 45/62), and 45 screws were misplaced in lateral direction (73%, 45/62). 36 screws (10%) perforated the anterior vertebral cortex. Twenty eight screws were misplaced in overweight group, 12 screws in obese group, and 22 screws in normal weight group. With the number of screws available, subgroup analysis did not reveal a significant difference in the grade (p=0.10) or the direction (p=0.97) of pedicle breaches among groups.
Conclusion Our data suggest that obesity does not affect the accuracy of percutaneous pedicle screw placement. We do not hesitate or deny the surgery because of patient’s heavy body habitus, which seems to be a apparent benefit of minimally invasive spinal surgery.
Lumbar cortical screw, an alternative to the traditional pedicle screw, has more cranially and laterally oriented trajectory within pedicle after being anchored in the pars interarticularis. Such cortical trajectory can lower the risk of nerve root impingement by traditional pedicle screw and reduce the iatrogenic soft tissue damage that occurs with muscle stripping and lateral retraction for traditional trajectory. In addition, lumbar cortical screw proved equivalent pullout strength compared with the traditional pedicle trajectory despite its shorter and smaller screw design.
However, clinical trial is still in the beginning stage, and further clinical studies are required to clarify the actual outcome of the lumbar cortical screw.
Purpose To verify the validity of a pedicle screw based posterior dynamic stabilization(PDS).
Materials and Methods At first, theoretical evidences were reviewed and presented the objections against PDS. The answers were investigated by reviewing the development concepts and clinical evidences of each device.
Results There is no PDS which has been approved as a dynamic stabilizer by US FDA yet. Dynesis® and Isobar TTL® were approved as a fusion adjunct. AccFlex® and CD-Horizon Legacy PEEK rod® were approved as a single level posterior lumbar interbody fusion adjunct. Dynesys® is undergoing an FDA IDE study as a non-fusion dynamic stabilizer. Patient’s symptoms were improved, however, there were scarce controlled studies with simple decompression or fusion surgeries. Furthermore quantitative comparison of improvement was impossible because the subjects were not homogenous. Adjacent segment degeneration was not prevented. Stabilized segments showed further degeneration and there wasn’t a case which showed regeneration of disc. Most of segments were fused or became more stable than physiologic motion and allowance of the PDS. Device failure was reported as 5-21%, however most cases were asymptomatic.
Conclusion In the light of current evidences, PDS is considered not to prevent the problems which were engendered by fusion surgeries. It is not convincible that PDS has a niche between decompression and fusion surgeries.
Protecting cranially located facet joints during pedicle screw placement is one of the modifiable factors that could prevent possible adjacent level problems related with spinal fusion procedure. Placing pedicle screws percutaneously appears to be more challenging in the technical aspect than performing with traditional open technique because of its limited selecting entry point for screw placement. The authors have reported surprisingly higher incidence and risk factors of cranial facet joint violations by percutaneously placed pedicle screws. The purpose of this literature was to illustrate the surgical technique focusing on the tips to avoid cranial facet joint violation during percutaneous placement of pedicle screws.

 First
First Prev
Prev

