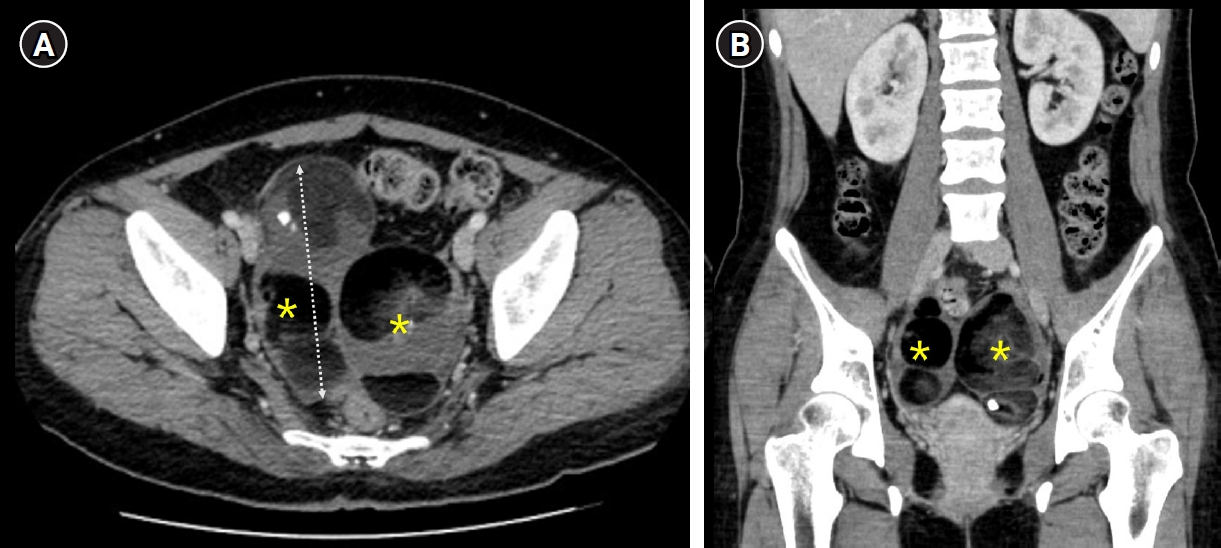
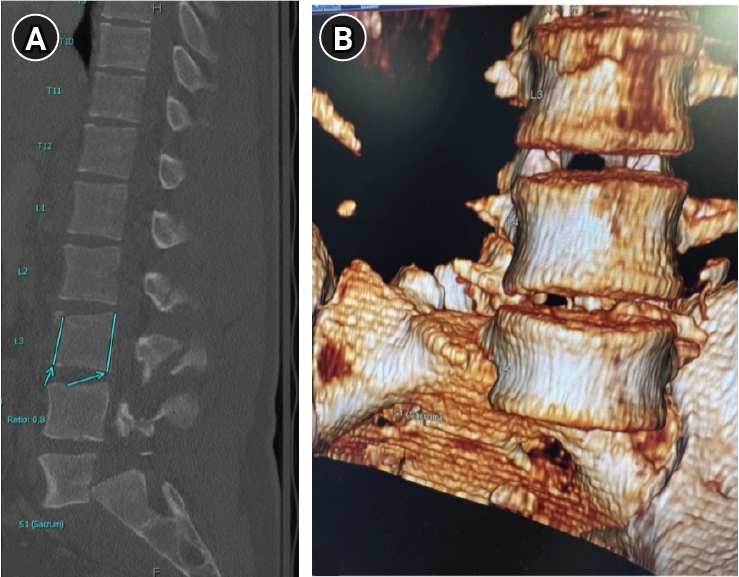
Dysplastic spondylolisthesis is a developmental subtype characterized by congenital lumbosacral abnormalities and progressive instability. Primary presentation with cauda equina syndrome (CES) has rarely been reported. We report a rare case of CES associated with highgrade dysplastic spondylolisthesis in a patient with concurrent giant ovarian teratomas, which contributed to delayed diagnosis and treatment because of overlapping pelvic symptoms. The patient presented with progressive urinary dysfunction, saddle anesthesia, and lower- extremity symptoms. Radiographic evaluation demonstrated high-grade L5–S1 dysplastic spondylolisthesis with severe canal compromise and lumbosacral deformity. Surgical treatment involved neural decompression and controlled deformity correction with sacral dome osteotomy and interbody fusion performed under provisional stabilization. Postoperatively, the patient demonstrated meaningful neurological recovery with improvement of urinary symptoms and restoration of lumbosacral alignment. This case highlights that CES can occur as an initial manifestation of dysplastic spondylolisthesis and underscores the importance of early spinal evaluation and timely surgical treatment with appropriate reduction techniques to prevent further neurological deterioration in patients with persistent neurological symptoms.
Traumatic lumbar spondyloptosis is a rare entity associated with high-velocity mechanisms and is the most severe form of lumbar spondylolisthesis. Operative management is often required; however, the relative merits of reduction versus in situ fusion remain debated, largely owing to the technical difficulty of attaining satisfactory fracture reduction. In this report, we describe external femoral traction as a novel technique for closed reduction of traumatic lumbar spondyloptosis. A 27-year-old man presented after a tree he was cutting fell on him and was found to have T3–7 AO Spine (AOS) A1 fracture, L3 AOS B2 fracture, and L5 AOS C fracture. Neurologic exam was consistent with multilevel nerve root injury. Definitive treatment included bilateral femoral traction, open reduction, and combined anterior/posterior fixation. A multidisciplinary team including orthopedic surgery, plastic surgery, vascular surgery, and neurosurgery were involved. Complete reduction was obtained, and the patient experienced near-complete resolution of neurologic symptoms. This technique offers a unique solution to the challenge of traumatic lumbar spondyloptosis. Further study and follow-up are needed to confirm the utility and durability of this technique and the cranial extent of injury for which this technique might be applied.
Background The Selective thoracic fusion (STF) may be associated with risk of postoperative coronal decompensation, lumbar decompensation and adding-on phenomenon, which can lead to persistence of the lumbar curve and consequently to deviation of the trunk. Therefore, the STF is the most debatable issue as the optimal surgical correction in adolescent idiopathic scoliosis with Lenke 1C curves.
Methods A total of 30 patients with adolescent idiopathic scoliosis with Lenke 1C curves who underwent STF between 1996 and 2017 were included. Minimum follow-up duration was five years. We analyzed the incidence of coronal decompensation, lumbar decompensation, distal adding-on phenomenon and trunk shift in these patients for radiographic adverse event. Clinical outcome was assessed by using the Scoliosis Research Society (SRS)-22r scores.
Results The mean age at the time of surgery was 13.8±2.9 years. The mean follow-up duration was 80.4±12.3 months.
The Cobb’s angle for main thoracic curve improved by 59.6% (p<0.001), and also The Cobb’s angle for thoracolumbar/ lumbar curve improved by 40.5% comparing preoperative and postoperative values (p<0.001). There was significant improvement in the Cobb’s angle for main thoracic and Thoracolumbar/lumbar curve comparing preoperative and last follow-up values (p<0.001). At last follow-up, the coronal balance was 10.3 ± 9.1 that significant improved from the immediate postoperative value (p=0.033). The incidence of coronal decompensation, lumbar decompensation, adding-on and trunk shift in our cohort was 16.7%, 10.0%, 13.3% and 10.0% respectively. The average SRS score at last follow-up in patients with radiographic adverse events was 4.3±0.5. That of patients without adverse events was 4.4±0.6. All domains between patients with and without adverse events had no statistical significance difference.
Conclusions Selective thoracic fusion in Lenke 1C curves have acceptable risk of coronal decompensation, lumbar decompensation, distal adding-on, trunk shift. However, no revision surgery was required in these patients after long term follow-up. Therefore, STF in Lenke 1C curves seems to be enough.
Purpose Minimally invasive technique in spinal surgery have evolved including cortical bone trajectory (CBT) screw technique which is s new lumbar pedicle screw path, as an alternative fixation technique for lumbar spine.
Theoretical advantage is that it provides enhanced screw torque and has biomechanical characteristics, also it minimizes approach-related damages. Midline lumbar fusion (MIDLF) has appeared with CBT screw technique.
Many studies of CBT screw reported the effectiveness of MIDLF. We adopted this technique for lumbar degenerative spondylolisthesis and evaluated early radiological outcomes.
Materials and Methods From May 2014 to March 2015, 17 patients (mean age 65.6±7.5 years; 4 males, 13 females) underwent MIDLF procedures for the treatment of single level lumbar spondylolisthesis. Average follow-up period was 8.8±2.7 months. Initial and last follow-up X-ray and computed tomography (CT) were evaluated for screw malposition, detection of peri-screw halo, loosening of the construct, or signs of spinal instability.
Results The average bone mineral density (BMD) was -1.9±0.8. Eleven patients were fused at L4-5, 5 were at L3-4, and 1 was at L2-3. Five CBT screws were converted into pedicle screws due to intraoperative misposition of screws, so total 63 CBT screws were evaluated for peri-screw halo and malposition. There were no findings of screw pull-out or breakage in all screws. Four out of 63 (6.3%) screws were judged as peri-screw halo, and 20 (41.2%) screws were judged as malposition (1 medial; 2 superior; 17 lateral pedicle violation). But, there were no screw related nerve root injury. In all cases, interbody bony mass were identified. Four out of 17 (23.6%) patients were detected more than 2 degrees motions on flexion-extension lateral X-rays at final follow-up, and 1 out of these 4 patients was identified loss of reduction. There was no operation related complication.
Conclusion There is no doubt that MIDLF with CBT screw is the minimally invasive method. Many numbers of screw malposition identified in our series were thought to be due to our earlier experience of trying free hands technique.
We recommend the use of intraoperative fluoroscopy, which achieve accuracy. Although MIDLF with CBT has theoretical strengths, we must evaluate further long-term clinical follow-up and measure outcome.
Introduction A spondylitis developed after a surgery has been usually treated with drainage and curettage through anterior approach and autoiliac strut bone graft. However, anterior support with titanium cage combined with posterior pedicle screw fixation has been attempted. Implanting a foreign material is usually prohibited at an active pyogenic infection site. We tried to prove the usefulness of chip bone graft with metal cages in surgical treatment of spondylitis developed in posterior lumbar intebody fusion cases.
Materials and Methods This is a retrospective study. The patients who received posterior lumbar interbody fusion (PLIF) between Jan. 2007 and Dec 2017 and had a spondylitis around the cage were reviewed. There were 1,831 PLIFs during the study period. There were 32 cases of surgical site infection and 20 of them were spondylitis around the cage. Ten out of the 20 cases had a revision surgery. All implants removal, drainage and curettage were done and interbody bone graft and pedicle screw re-fixation was done simultaneously. Five cases used autoiliac strut bone (Group I) and the other 5 cases used titanium cage and autoiliac chip bone (Group II) as interbody graft materials.
The demographic, diagnostic and microbiological characteristics were investigated and the results of treatment were compared between the two groups.
Results The diagnosis of infection was made at 282.0±106.1 (180~410) days in group I and 209±118.4 (75~335) days in group II after the PLIF. All cases had neither general fever nor local manifestations like heating and redness etc.
All patients had back pain, however, only 2 cases of group II had neurological symptoms. C-reactive protein (CRP) level was elevated at 2 weeks from the PLIF in all cases (p<0.001). All cases had implant loosening at the time of their diagnosis. There was no failure of infection control. All cases showed normalization of CRP and radiological interbody fusion. The final Oswestry disability index (ODI) showed no difference between the two groups. ODI improved from 54.6±11.5 to 42.2±6.8 in group I (p=0.095) and from 63.6±6.9 to 44.8±11.7 in group II (p=0.025).
Conclusion For the surgical treatment of spondylitis that were developed in PLIF, a comprehensive one stage operation that comprised all implants removal, drainage and curettage followed by simultaneous intebody bone graft with metal cages and pedicle screw re-fixation was useful to control the infection.
Objective To investigate the association of quantitative paraspinal muscle measurements to the Oswestry disability index (ODI) in patients with lumbar spondylolisthesis.
Materials and Methods Ninety two patients (mean age, 61.6 years; male, mean age, 71.8 years ; female; mean body mass index [BMI], 24.9 kg/m2 ) who had undergone lumbar fusion due to spondylolisthesis with available selfcompleted postoperative ODI were included. The total cross-sectional area (CSA) and functional CSA (FCSA; i.e., area containing only lean muscle tissue) of the paraspinal muscle group (multifidus and erector spinae muscles) and the psoas muscles were measured at L2–L3, L3–L4, and L4–L5 disc levels each on preoperative magnetic resonance imaging (MRI) and the sum of areas at each level served as representative values for each muscle. The FCSA/total CSA ratio and the skeletal muscle index (SMI=muscle area [cm2 ]/patient height2 [m2 ]) were calculated.
Pearson’s correlation analyses were performed to evaluate the relationship between preoperative paraspinal muscle measurements and postoperative ODI.
Results Quantitative values of low paraspinal muscle showed significant correlation with high ODI values. As a result of this study, the preoperative paraspinal muscle was quantified in the group of patients undergoing spinal fusion.
Patients with low value in CSA and FCSA of paraspinal muscle could observe the tendency to transition to low clinical outcomes. Therefore, quantitative values of surrounding muscles are factors affecting clinical outcomes of patients undergoing spinal surgery Conclusion: Smaller muscle bulk (total CSA) of psoas muscles and lean muscle mass (FCSA) of paraspinal muscle group and psoas muscles combined on preoperative MRI were associated with significant postoperative disability based on ODI in patients with lumbar spondylolisthesis.
Objectives to report a surgical site infection from Aspergillus after a lumbar discectomy.
Aspergillus is ubiquitous fungus. People with normal immunity are usually not infected by it, however, surgical site infection from it often developed even in normal population.
Materials and Methods The diagnostic and therapeutic experience of 55-year-old male patient who underwent L45 discectomy who had surgical site infection from Aspergillus was reviewed.
Results He had 4 times surgical treatment and empirical antibiotic therapy due to progressive extension of infection without microbiologic confirmation. Aspergillus flavus was identified at 5th operation and he was cured by adding an anti-fungal agent.
Conclusions An Aspergillus infection after an operation can be developed even in normal immunity population.
If a surgical site infection patient without fever and draining sinus does not improve by conventional treatment, Aspergillus infection should be considered.
Purpose To analyze the risk of a fall in patients with cervical spondylotic myelopathy (CSM) and its clinical significance.
Materials and methods 40 patients with CSM who visited to our hospital From May 2014 to April 2015 were enrolled in this study. After confirmation of CSM based on MRI and Physical examination, patients were divided into three groups according to m-JOA score (Group A; severe; score <8, Group B; moderate; score 8-12, Group C; mild score >13). All patients enrolled in this study performed 4 functional assessment test including Alternative-Step Test (AST), Six-MeterWalk Test (SMT), Sit-to-Stand test (STS), and Timed Up and Go test (TUGT) to assess the risk of a falls (ROF).
Results There were statistical significance between m-JOA score and ROF except for SMT. Average time (seconds) for STST was 26.12±5.60, 20.99±5.92 and 15.37±3.41 in group A, B, C, respectively (p=0.001), Although average time(s) for AST was 16.81±3.83, 14.39±4.05 and 12.37±3.95 in group A, B, C with no statistical significance (p=0.106), there was a significance between the value of Group A and C (p=0.047). Average time(s) for TUGT was 31.86±17.05, 15.09±4.59,18.04±9.32 in group A, B, C, respectively, showed statistical significance (p=0.000).
Conclusion According to its severity of myelopathy, it took more time to carry out each ROF assessment tests. Among 4 functional assessment tests of ROF, STST showed the most highest correlation with mJOA socre. Careful attention of ROF will be needed in patients with myelopathy.
Purpose Total en bloc spondylectomy (TES) is one of curative surgical methods used for solitary spinal tumors, if indicated. However, TES is a complex technique and prudent preparation is mandatory. However, elective TES is not always possible for patients with neurological and mechanical spinal instability. In such situations, percutaneous pedicle screw fixation, with the purpose of stabilizing the spine and gaining time before TES, may be used.
Methods The first patient was a 29-year-old female who visited the emergency room (ER) due to progressive paraparesis (motor grade III/V) and back pain. Magnetic resonance imaging (MRI) showed compression of the spinal cord by a tumor and a collapsed L1 body. The second patient was a 23-year-old female who came to the ER with severe back pain. MRI revealed compression of the spinal cord by a collapsed T11 vertebral body and a tumor.
In both cases, neurological and mechanical instabilities were caused by a primary vertebral tumor. For both patients, TES was an optimal surgical technique, but TES was not possible on an emergency basis.
Results In both patients, percutaneous pedicle screw fixation, distraction, and biopsy were performed on an emergency basis. Subsequently, weakness and/or pain improved in both patients. Elective TES operations were successfully performed 3 weeks or 1 month later.
Conclusions If TES is indicated, but preparation time is insufficient, tentative spinal stabilization with a percutaneous technique may be utilized before TES. However, considering the need for additional surgery, skin incision, and cost, this surgical strategy should be selectively applied.
Purpose There is an increasing recognition of the clinical importance of the sagittal balance after lumbar fusion surgery. The purpose of this study to review the etiology of sagittal imbalance after lumbar fusion surgery and report the radiographic and clinical results of surgical treatment of these patients.
Materials and Methods Retrospective review of revision spine surgery due to sagittal imbalance in 35 patients.
Various surgical methods such as posterior–anterior–posterior (PAP) sequential approach, Smith–Peterson osteotomy (SPO), pedicle subtraction osteotomy (PSO), and vertebral column resection (VCR) were performed to restore lumbar lordosis. The outcome variables included preoperative, postoperative, and follow-up radiographic films, and a clinical assessment using Oswestry Disability Index (ODI), SRS 22, and a review of postoperative complications.
Results The mean age of the patients was 62 years (age range, 49–74), and mean follow-up duration was 31 months (range, 24–37) for clinical and radiographic outcome variables. The mean preoperative LL/PI (lumbar lordosis/ pelvic incidence) ratio was different from postoperative value (P< 0.0001). Twenty one out of 35 patients showed perioperative complications including proximal junctional kyphosis or infection. All functional outcomes measures improved postoperatively (P < 0.0001).
Conclusion Most common causes of revision spine surgery due to sagittal imbalance include failure to enhance lumbar lordosis, proximal vertebral collapse, and junctional kyphosis. LL/PI ratio was considered as one of the valuable spinopelvic parameter for evaluation of sagittal imbalance. Following surgical treatment, sagittal balance was generally improved with good to excellent clinical outcomes and high patient satisfaction, although the perioperative complication rates are high.

 First
First Prev
Prev

