Purpose This retrospective study investigated the distinct clinical and radiographic drivers of early- versus late-onset proximal junctional kyphosis (PJK) following multilevel thoracolumbar (TL) fusion.
Methods After applying the exclusion criteria (spinal infection, neuromuscular disease, age <50 years), the analysis included 136 patients who underwent ≥4-level TL fusion and were followed up for a minimum of 2 years. PJK was classified as early (≤6 months) or late (>6 months) onset. Patient-related factors, surgical variables, sagittal spinopelvic parameters, and preoperative magnetic resonance imaging findings were analyzed using multivariate logistic regression to identify independent predictors of early PJK.
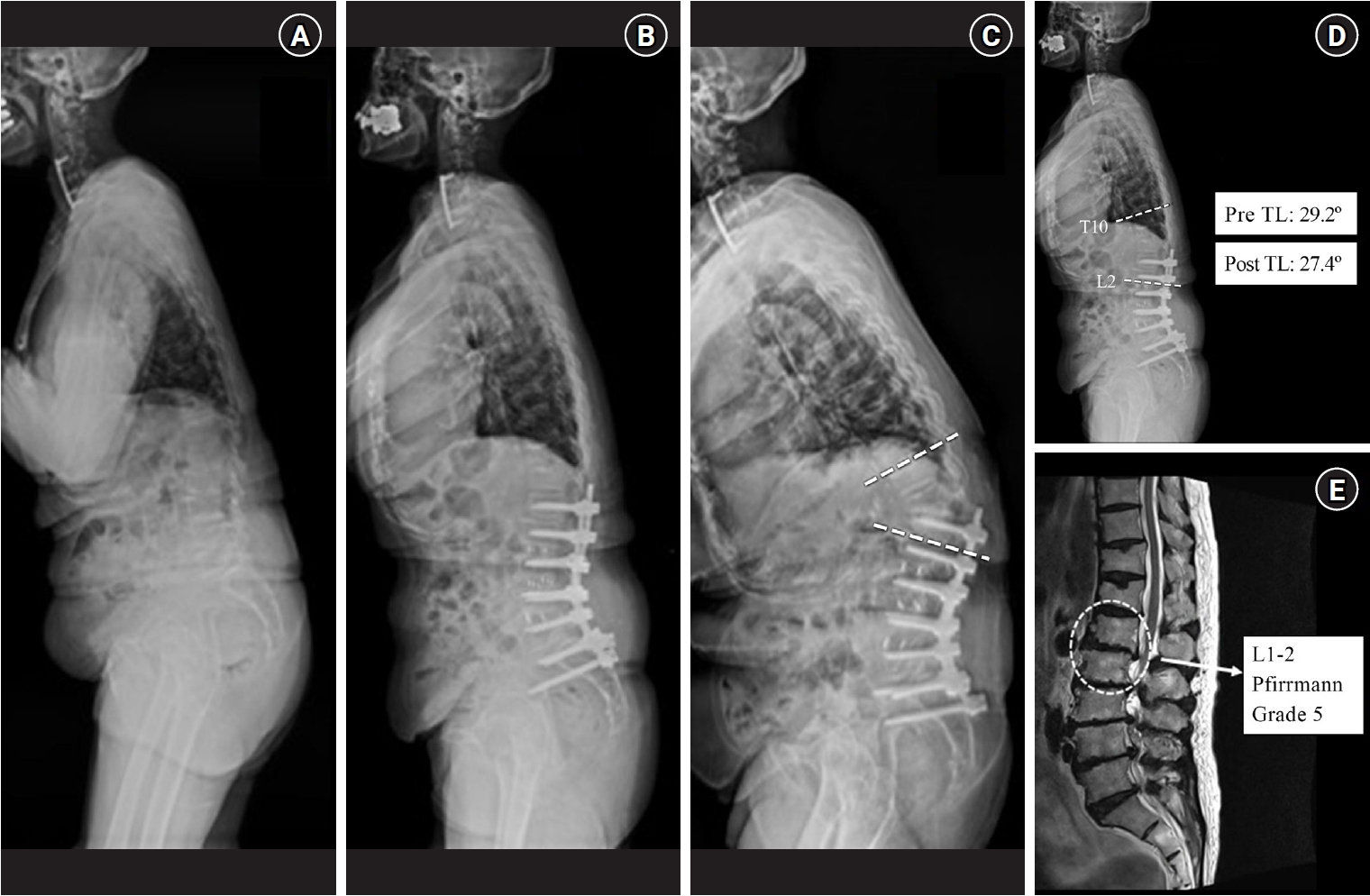
Results Among 24 patients (17.6%) who developed PJK, the early and late-onset groups included 13 and 11 patients, respectively. The early PJK group exhibited significantly greater preoperative and postoperative TL angles compared with the late group (preoperative: 23.03±13.83° vs. 9.67±9.67°, p=0.024; postoperative: 19.6±6.95° vs. 6.95±6.35°, p<0.001). The Pfirrmann grade of the L1–2 intervertebral disc was significantly higher in the early PJK group (3.92±0.95 vs. 2.81±0.60, p=0.006). No surgical variables differed significantly between the groups. Multivariate analysis confirmed greater postoperative TL angle and more advanced L1–2 disc degeneration as independent predictors of early PJK.
Conclusion Early-onset PJK following multilevel TL fusion is primarily driven by regional biomechanical vulnerabilities, specifically residual postoperative TL kyphosis and advanced adjacent L1–2 disc degeneration, rather than by surgical variables. Meticulous evaluation of regional TL alignment and adjacent disc health during surgical planning is critical for risk stratification and prevention of early junctional failure.
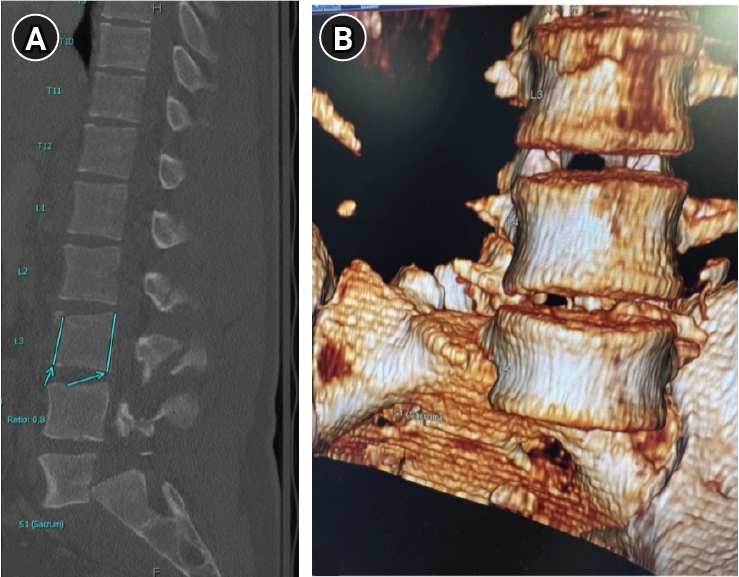
Traumatic lumbar spondyloptosis is a rare entity associated with high-velocity mechanisms and is the most severe form of lumbar spondylolisthesis. Operative management is often required; however, the relative merits of reduction versus in situ fusion remain debated, largely owing to the technical difficulty of attaining satisfactory fracture reduction. In this report, we describe external femoral traction as a novel technique for closed reduction of traumatic lumbar spondyloptosis. A 27-year-old man presented after a tree he was cutting fell on him and was found to have T3–7 AO Spine (AOS) A1 fracture, L3 AOS B2 fracture, and L5 AOS C fracture. Neurologic exam was consistent with multilevel nerve root injury. Definitive treatment included bilateral femoral traction, open reduction, and combined anterior/posterior fixation. A multidisciplinary team including orthopedic surgery, plastic surgery, vascular surgery, and neurosurgery were involved. Complete reduction was obtained, and the patient experienced near-complete resolution of neurologic symptoms. This technique offers a unique solution to the challenge of traumatic lumbar spondyloptosis. Further study and follow-up are needed to confirm the utility and durability of this technique and the cranial extent of injury for which this technique might be applied.
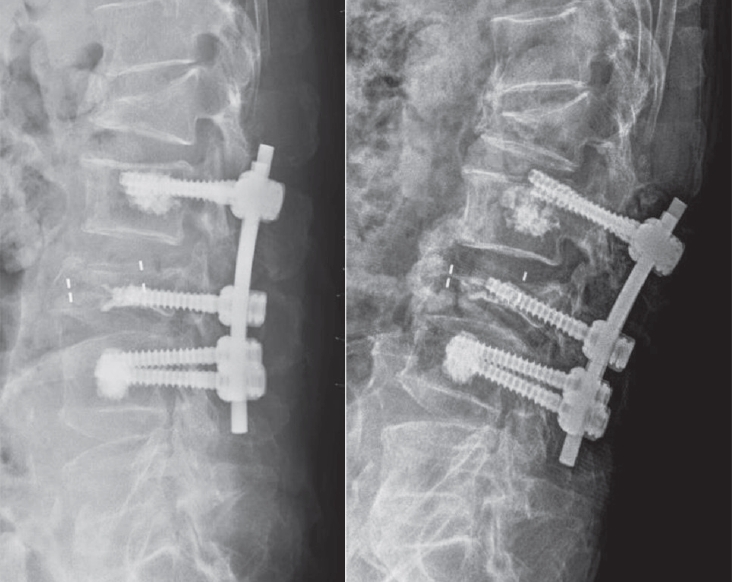
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
Objective To evaluate the efficacy and safety of anorganic bone matrix (ABM)/P-15 compared with local autograft bone in posterior lumbar interbody fusion (PLIF) with pedicle screws for degenerative lumbar diseases.
Methods This is a retrospective analysis of consecutive series of 138 patients undergoing 1 or 2 levels PLIF from 2015 to 2020 in our single institute. Local autograft bone or ABM/P-15 (i-factor, Cerapedics Inc., Westminster, Colorado USA) were used for interbody fusion. The successful fusion was defined as the segmental cobb angle of less than 5 degrees of in flexion/extension X-rays and continuity of the trabecular bony bridging in computed tomography (CT) images.
Results Among a total of 138 patients, total levels of fusion were 202, of which 74 were in 1 level fusion and 128 were in 2 level fusion. And 93 used ABM/P-15 and 109 used local autograft bone. The evaluation time of fusion status was 1 year after surgery. Successful fusion based on X-ray images was achieved 84.1% (90/107) for local autograft bone and 91.3% (84/92) for ABM/P-15 (p=0.127). Based on CT images, 86.9% (93/107) of autograft group and 95.6%(87/91) of AMP/P-15 group showed successful fusion respectively (p=0.034). Occurrence rate of autolysis was 14% (15/107) for local autograft bone and 17.6% (16/91) for ABM/P-15. Subsidence rates were 11.2% (12/107) for local autograft bone and 9.99% (9/91) for ABM/P-15. Hollow formation around pedicle screw was noted in 9.3% (10/107) for local autograft bone and 2.2% (2/91) for ABM/P-15.
Conclusions The use of AMP/P-15 for lumbar interbody fusion surgery can be a good substitute for local autograft bone in terms of better fusion rate and similar complication rate on radiologically.
Extreme lateral interbody fusion (XLIF) and direct lateral interbody fusion (DLIF) are novel minimally invasive transpsoas approaches to the lumbar spine for performing fusions. Advantages of DLIF include easier technique, faster recovery, minimal complication, high fusion rate, and possibility of achieving better alignment. Many previous reports have evaluated outcomes of DLIF. The authors described surgical procedure of DLIF and reviewed clinical outcomes, radiological outcomes, and complications from various literatures. In conclusion, the DLIF seems to be a valuable minimally invasive surgical tool for the fusion in patients with various diseases, including degenerative disc disease, instability, stenosis, scoliosis, tumor, infection, and adjacent segment degeneration.
Protecting cranially located facet joints during pedicle screw placement is one of the modifiable factors that could prevent possible adjacent level problems related with spinal fusion procedure. Placing pedicle screws percutaneously appears to be more challenging in the technical aspect than performing with traditional open technique because of its limited selecting entry point for screw placement. The authors have reported surprisingly higher incidence and risk factors of cranial facet joint violations by percutaneously placed pedicle screws. The purpose of this literature was to illustrate the surgical technique focusing on the tips to avoid cranial facet joint violation during percutaneous placement of pedicle screws.

 First
First Prev
Prev

