Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
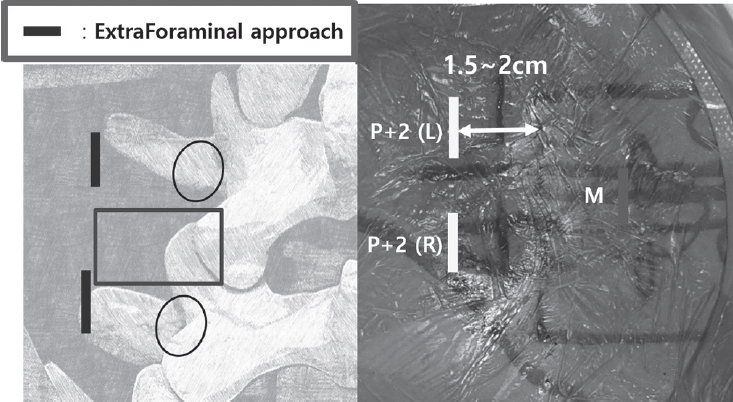
The foramen of L5-S1 can develop several degenerative diseases such as extraforaminal lumbar disc herniation, foraminal stenosis with disc height collapse, degenerative or spondylolytic spondylolisthesis, and far-out syndrome.
The floating technique in biportal endoscopic spine surgery (BESS) keeps a certain distance between instruments and spinal structures. 1) This key point makes the floating technique different from conventional endoscopic surgery, which uses the Kambin’s safe triangle as a work zone. The floating view can enable the surgeon to see the structures panoramically, under high magnification: consequently, fine discrimination of their margin and safe manipulation of neural structures can be guaranteed. A certain gap between the floating scope and lesion can permit various instruments, generally used in open spine surgery, to be inserted from the sides with fewer limitations. Extraforaminal or foraminal lesions under the lamina can be reached by avoiding the iliac crest, and total facetectomy, which has the potential of iatrogenic instability, is not required to explore the foraminal structures. However, the floating view can be obstructed by small bleeds from laminectomized bone and/or surrounding vessels. This present article describes the technique and provides tips on how to perform BESS with floating technique safely and successfully for various lesions at the L5-S1 foramen.
Purpose The purpose of the study was to investigate the effect of obesity on the accuracy of percutaneous pedicle screw placement.
Materials and Methods We performed a retrospective analysis on the first 89 patients undergoing minimally invasive lumbar fusion with percutaneous pedicle screw placements for the treatment of degenerative lumbar spinal disorder.
Based on patient’s body mass index (BMI), patients were divided into 3 groups: group 1 – normal weight (BMI<25, 38 patients, 157 screws); group 2 – overweight (25≤BMI<30, 29 patients, 124 screws); group 3 – obese (BMI≥30, 22 patients, 89 screws). Using postoperative computed tomography (CT) scans, the position of placed screws to the pedicle or anterior body perforation was evaluated using the following grading method: Grade A, completely in the range without pedicle cortex violation; Grade B, pedicle wall violation<2 mm; Grade C, pedicle wall violation 2 to 4 mm; and Grade D, pedicle wall violation>4 mm.
Results Among the 370 pedicle screws, 308 screws (83%) were perfectly placed within the pedicle. Among the 62 misplaced screws, 45 screws were grade B pedicle breaches (73%, 45/62), and 45 screws were misplaced in lateral direction (73%, 45/62). 36 screws (10%) perforated the anterior vertebral cortex. Twenty eight screws were misplaced in overweight group, 12 screws in obese group, and 22 screws in normal weight group. With the number of screws available, subgroup analysis did not reveal a significant difference in the grade (p=0.10) or the direction (p=0.97) of pedicle breaches among groups.
Conclusion Our data suggest that obesity does not affect the accuracy of percutaneous pedicle screw placement. We do not hesitate or deny the surgery because of patient’s heavy body habitus, which seems to be a apparent benefit of minimally invasive spinal surgery.
Summary of Background Data Recently, minimal invasive spine surgery has been used and spine surgeons are prone to the radiation exposures.
Objectives: To determine the radiologic hazard to the spine surgeon.
Methods We searched the PUBMED, MEDLINE with Mesh term from MIS, radiation exposure.
Results We reviewed the radiation exposure in different disease and surgery. There exist significant dose of radiation exposures in MIS Discectomy, MIS or open pedicle screw fixation, and kyphoplasty.
Conclusion Surgeons should aware of the radiation exposure of the spine surgery and should do efforts on minimize it.
Discectomy or fusion have been a gold standard of the treatment for discogenic back pain. Since mid 1950s, spine surgeons have introduced the concept of arthroplasty for the management of low back pain. The current technologies are total disc replacement (TDR), posterior dynamic stabilization (PDS), interspinous process. Although many studies have reported their efficacy and safety, there are still lacking high-quality evidence. It is also not proven that these technologies are superior to spinal fusion in preventing the adjacent segment disease.
Second generation TDR is newly developed technology. The current TDR could allow the motion of flexionextension and lateral bending, but it did not have the capacity to bear the axial compressive force. Second generation TDR placed the shock-absorption materials that can endure the compressive force. The current TDR was performed through the anterior approach, which is invasive and necessitates the removal of anterior longitudinal ligament. To
overcome these disadvantages, TDR through lateral approach was developed. Various type of nucleus replacement technologies have been introduced with theoretical advantages over TDR such as less invasiveness, stable segmental motion and preservation of disc height. However, some of them had critical problems such as the migration and subsidence of implanted prosthesis. Total facet replacement arthroplasty was developed to overcome both the
adjacent segment disease after fusion and the instability after posterior decompression. Because most of reports about total facet replacement arthroplasty are based on the results from the animal or cadaveric study, the long-term human trial is required.
New technologies regarding motion preservation spinal surgery have been introduced, shifting paradigm in spinal care. Even though various attempts have been made in the field of spine surgery, the fact is that all of these attempts do not succeed due to paucity of better clinical outcomes. Thus, well designed long-term studies are required to prove their safety and efficacy, showing “superiority”, not just “no inferiority” to the traditional treatments.

 First
First Prev
Prev

