1)Department of Orthopaedic Surgery, Yonsei Wonju University College of Medicine, Wonju, Korea
2)Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea
Corresponding author: Ki-Youn Kwon, M.D. Department of Orthopedic Surgery, Yonsei Wonju University College of Medicine, 20, Ilsan-ro, Wonju-si, Gangwon-do, 26426 Korea TEL: +82-33-741-1356, FAX: +82-33-741-1365 E-mail: 1stskwon@naver.ac.kr
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background
Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
Material and Methods
This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results
Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions
Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.
본 연구는 급성 골다공증성 척추 압박 골절 환자에서 로모소주맙 기반 보존 치료와 경피적 척추성형술의 3개월 단기 치료 결과를 비교하고자 하였다.
배경
경피적 척추성형술은 급성 골다공증성 압박 골절에서 신속한 통증 완화를 제공하지만, 시멘트 누출, 인접 분절 골절 등의 합병증 위험이 존재한다. 로모소주맙은 골형성을 촉진하고 골흡수를 억제하는 항스클레로스틴 단일클론항체로, 골절 예방 효과가 입증되었으나 급성 척추 골절에서의 치료 효과는 아직 명확히 밝혀지지 않았다.
재료 및 방법
본 후향적 연구는 2022년 1월부터 2024년 12월까지 MRI로 급성 OVCF가 확진된 환자 84명을 대상으로 하였다. 로모소주맙 피하 주사를 매달 1회 투여받은 군(n=52)과, 척추성형술 후 알렌드로네이트를 매주 복용한 군(n=32)으로 나누어 분석하였다. 모든 환자는 칼슘(500 mg) 및 비타민 D3(1,000 IU)를 매일 복용하였다. 임상적 결과는 VAS 및 ODI를 통해 평가하였으며, 방사선학적 결과는 전방 척추체 높이 변화를 기준으로 치료 전, 치료후 1개월, 3개월 시점에서 측정하였다.
결과
두 군 모두 치료 1개월 및 3개월 시점에서 VAS 및 ODI 점수의 유의미한 개선을 보였으며, 두 군 간 점수 변화에는 통계적으로 유의한 차이가 없었다. 전방 척추체 높이 변화 또한 두 군 간 유사하였다.
결론
로모소주맙 기반 보존적 치료는 급성 골다공증성 압박 골절 환자에서 척추성형술과 유사한 단기 임상적 및 방사선학적 효과를 보이며, 비침습적이고 효과적인 대안 치료법으로 고려될 수 있다.
Osteoporosis is a common condition in the elderly, characterized by reduced bone mass and microarchitectural deterioration, which predispose individuals to fragility fractures.1,2) Among these, osteoporotic vertebral compression fractures (OVCFs) are the most prevalent and are associated with significant pain, functional impairment, and increased morbidity and mortality.3,4)
Conservative management—including analgesics, short-term bed rest, and spinal orthosis—is the first-line treatment for most acute OVCFs.5,6) However, in cases where pain persists or vertebral collapse progresses despite adequate pain control, conservative approaches may be insufficient.7,8) Such patients are at increased risk of chronic pain, nonunion, and even long-term disability.9,10) In some instances, surgical intervention may become necessary.11)
Percutaneous vertebroplasty (PVP), with or without kyphoplasty, has been widely employed for the rapid alleviation of pain and early mobilization in patients with acute OVCFs.12-14) However, recent high-level evidence has questioned its long-term efficacy, with some randomized controlled trials reporting no significant benefit compared to sham procedures.15,16) Moreover, cement augmentation procedures carry risks such as cement leakage, pulmonary embolism, adjacent vertebral fractures, and infection.17)
Romosozumab is a humanized monoclonal antibody that inhibits sclerostin, a negative regulator of bone formation. By simultaneously promoting bone formation and suppressing bone resorption via the Wnt/β-catenin signaling pathway, romosozumab has been shown to rapidly increase bone mass and reduce fracture risk in osteoporotic patients.18-20) Despite its growing use, the role of romosozumab in the acute phase of OVCFs remains unclear, and concerns regarding cardiovascular safety and cost-effectiveness persist.21,22)
In this study, we aimed to evaluate and compare the clinical and radiographic outcomes of romosozumab-based conservative therapy and percutaneous vertebroplasty in patients with acute OVCFs over a 3-month period.
Materials and Methods
1. Study design and population
this retrospective study included patients diagnosed with acute osteoporotic vertebral compression fractures (OVCFs) between January 1, 2022, and December 31, 2024. Acute OVCFs were confirmed using magnetic resonance imaging (MRI), with findings of low signal intensity on T1-weighted images and high signal intensity on fat-suppressed T2-weighted images. Bone mineral density (BMD) of the lumbar spine and femoral neck was assessed using dual-energy X-ray absorptiometry (DEXA), and osteoporosis was defined as a T-score below −2.5, according to the World Health Organization criteria.
Patients with Kummell’s disease, neurological deficits, burst fractures involving the middle or posterior column, previous spinal surgery or percutaneous vertebroplasty, spinal tumors, or active infection were excluded. Among 106 patients initially reviewed, 22 were excluded due to loss to outpatient follow-up. Patients who discontinued oral alendronate were not considered dropouts. Ultimately, 84 patients were included in the final analysis.
This study was approved by the Institutional Review Board (IRB) of Wonju Severance Christian Hospital, Yonsei University (IRB No. CR325037). The requirement for informed consent was waived due to the retrospective nature of the study.
2. Treatment Protocol
Patients were categorized into two groups: the romosozumab group (n=52), which received monthly subcutaneous injections of romosozumab (210 mg), and the vertebroplasty group (n=32), which underwent percutaneous vertebroplasty under local lidocaine anesthesia followed by weekly oral administration of alendronate (70 mg). All patients received daily oral supplementation of calcium (500 mg) and vitamin D₃ (1,000 IU). For pain control, combination analgesics (acetaminophen 325 mg+tramadol hydrochloride 37.5 mg) were prescribed twice daily as needed. Patients self-modulated their use of analgesics and physical activity based on perceived pain levels.
3. Clinical and Radiographic Assessment
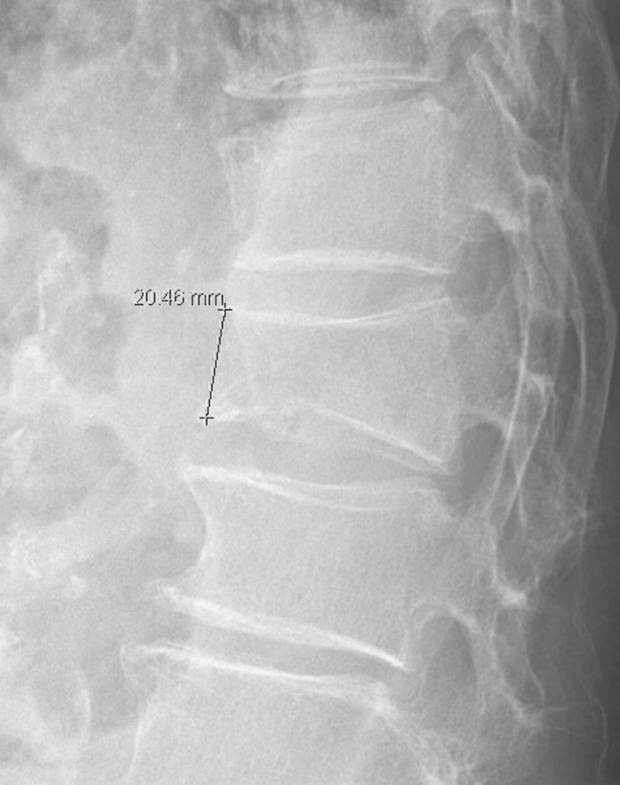
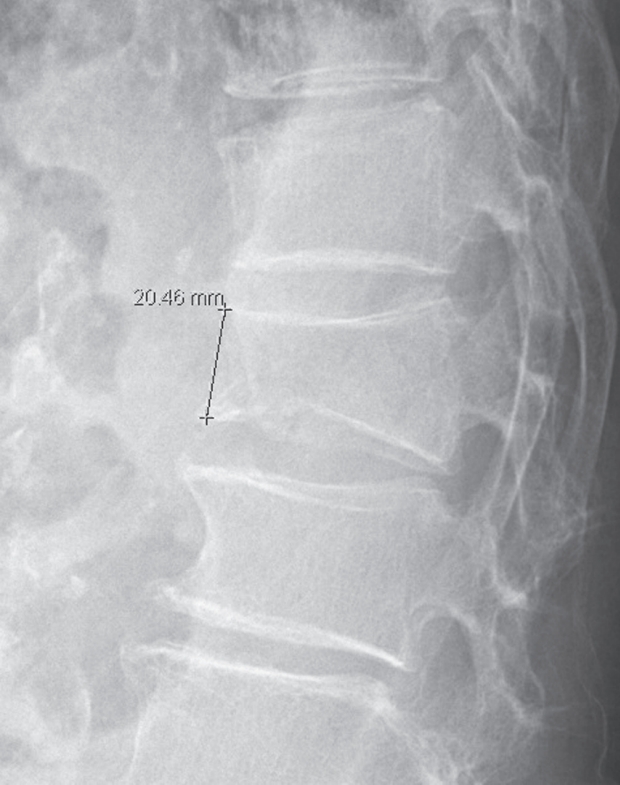
Clinical evaluations were performed at baseline, 1 month, and 3 months after treatment. Pain and disability were assessed using the Visual Analogue Scale (VAS) and the Oswestry Disability Index (ODI), both validated and widely used tools in spinal research. Radiographic assessment included measurement of anterior vertebral body height on lateral spine radiographs obtained at each time point. The height was measured by drawing a perpendicular line from the superior endplate to the inferior endplate at the anterior margin of the fractured vertebral body, as illustrated in Fig. 1.
4. Statistical Analysis
Statistical analyses were conducted using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean±standard deviation, and categorical variables as frequencies and percentages. Between-group differences in continuous variables were assessed using Student’s t-tests, and categorical variables were analyzed using chi-square tests. A p-value <0.05 was considered statistically significant.
Results
A total of 84 patients were included in the final analysis, with 52 in the romosozumab group and 32 in the vertebroplasty group. Four patients in the vertebroplasty group discontinued alendronate after 1 month but were retained in the analysis. There were no statistically significant differences in baseline characteristics—including age, sex, body mass index (BMI), bone mineral density (BMD) T-score, prior use of osteoporosis medication, and history of vertebral fracture—between the two groups. Baseline Visual Analogue Scale (VAS) scores, Oswestry Disability Index (ODI) scores, and anterior vertebral body height were also not significantly different between the groups (Table 1).
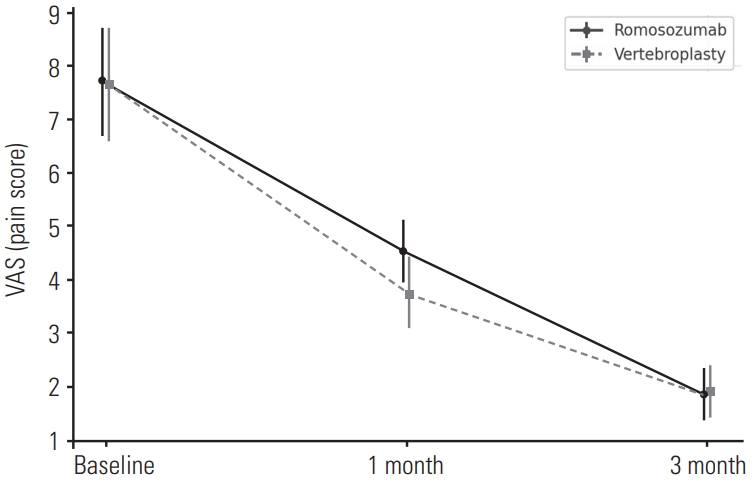
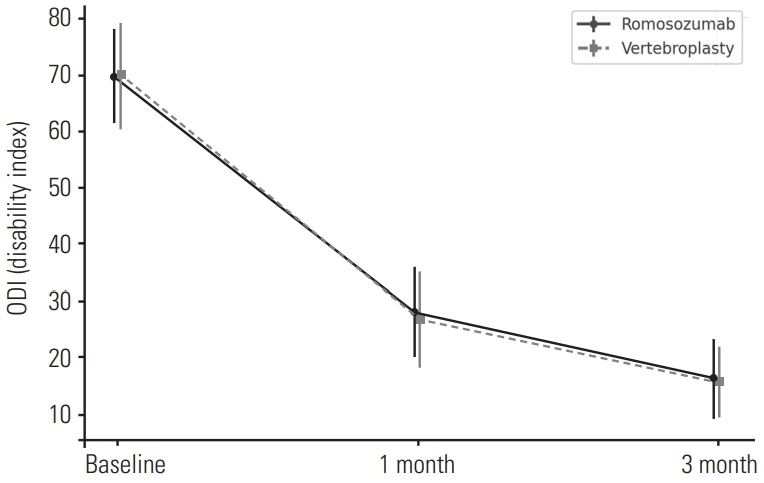
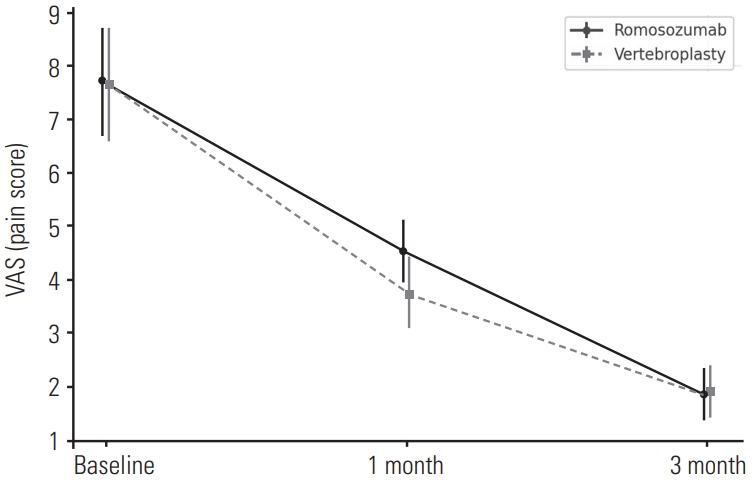
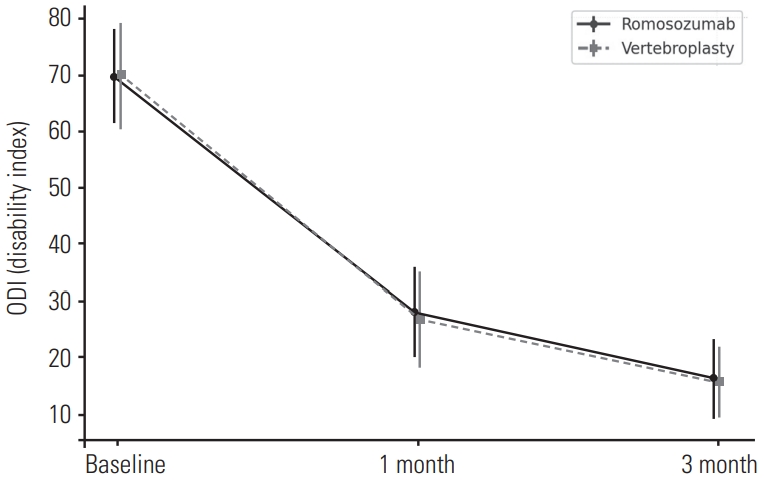
Both groups demonstrated statistically significant improvements in VAS and ODI scores at 1 and 3 months compared to baseline (within-group p<0.05), with no significant differences between the groups at any time point (Table 2). These temporal changes in clinical scores are graphically illustrated in Fig. 2 (VAS) and Fig. 3 (ODI), showing similar downward trends in both groups.
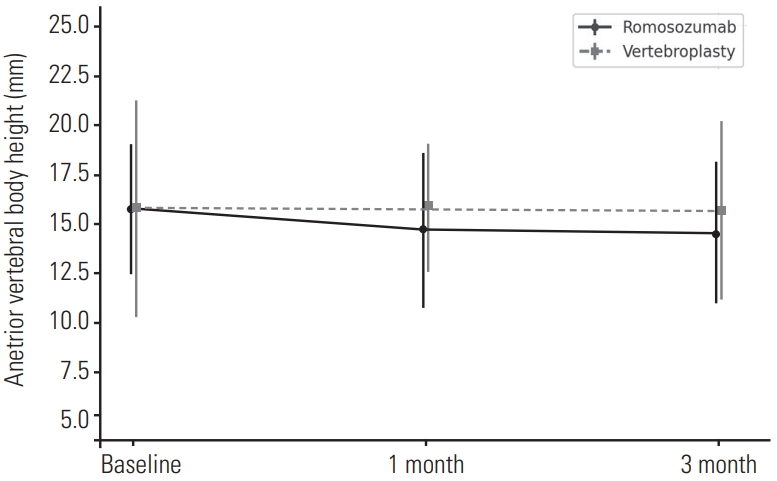
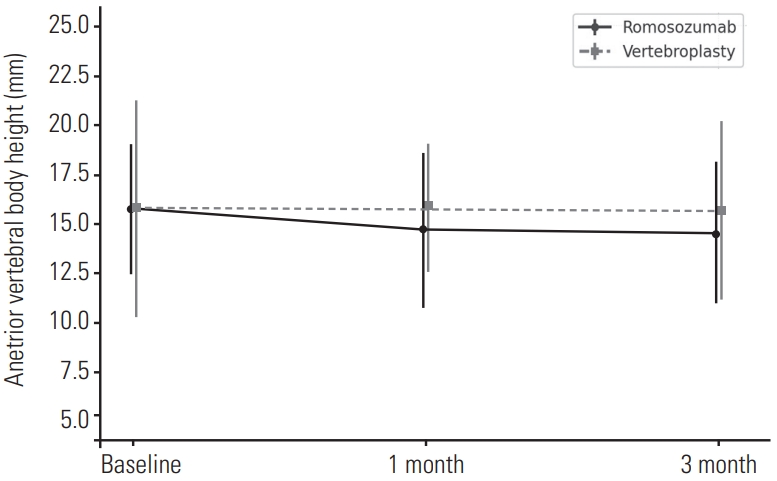
Anterior vertebral body height showed a decreasing trend in the romosozumab group compared to the vertebroplasty group at both 1 and 3 months, but the intergroup differences were not statistically significant (Tables 3 and 4). Fig. 4 illustrates these trends, showing a mild decrease over time without significant intergroup differences. No serious adverse events were reported in either group during the 3-month follow-up period.
Discussion
While multiple approaches exist for managing acute osteoporotic vertebral compression fractures (OVCFs), the optimal strategy remains debated, particularly in balancing efficacy and procedural invasiveness. Vertebroplasty has long been used to achieve rapid pain relief and early mobilization, yet recent studies have questioned its long-term clinical benefit and safety.15,16) Conservative treatment, although widely used, frequently results in residual pain and delayed recovery, especially in elderly patients.9,10)
Romosozumab, an anabolic agent that promotes bone formation while inhibiting resorption via the Wnt/β-catenin signaling pathway, offers a pharmacologic alternative with the potential to enhance early bone healing.18-20) However, its role in the acute phase of vertebral fractures is not yet well established.
In our study, both romosozumab and vertebroplasty demonstrated significant improvements in Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) scores at 1 and 3 months after treatment, with no statistically significant differences between the groups. These findings suggest that romosozumab-based conservative treatment may provide comparable short-term clinical outcomes to vertebroplasty in the management of acute OVCFs. Importantly, this benefit was achieved without exposure to the procedural risks associated with cement augmentation, such as cement leakage, adjacent vertebral fractures, or pulmonary complications.17)
The lack of significant difference in vertebral body height restoration between the two groups further supports the possibility that pharmacologic treatment may help maintain structural integrity without the need for surgical intervention. Given the biologically inert nature of polymethyl methacrylate (PMMA) cement used in vertebroplasty, which does not integrate with bone tissue and may hinder natural healing,23) romosozumab’s potential role in promoting bone regeneration in fractured vertebrae warrants further investigation.
This study has several limitations. First, it was a retrospective analysis with a relatively short follow-up period limited to 3 months. Long-term outcomes, including refracture rates, bone remodeling, and sustained functional recovery, were not evaluated.24) Second, although romosozumab is known to increase bone mass rapidly, the optimal treatment duration and cost-effectiveness in the context of acute fractures remain unclear.22) Finally, this study focused primarily on clinical and radiographic parameters and did not include comprehensive quality of life (QOL) measures such as EQ-5D or SF-36,25,26) which may provide a broader understanding of patient-reported outcomes.
Despite these limitations, our findings highlight romosozumab as a promising non-invasive therapeutic option in the acute management of OVCFs, particularly in patients at higher procedural risk or those unwilling to undergo vertebral augmentation.
Conclusions
Romosozumab-based conservative therapy may offer a non-invasive alternative to vertebroplasty in the treatment of acute osteoporotic vertebral compression fractures.
NOTES
Conflict of Interest Statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members.
Ethical Review Committee Statement
This study was approved by Yonsei Wonju University College of Medicine Institutional Review Board and Ethics Committee, which issued a waiver regarding the need for informed consent (CR325037). All studies were performed in accordance with relevant guidelines and regulations.
Fig. 1.
Measurement of anterior vertebral body height.
Fig. 2.
Change in VAS scores from baseline to 3 months.
Fig. 3.
Change in ODI scores from baseline to 3 months.
Fig. 4.
Change in anterior vertebral body height from baseline to 3 months.
Table 1.
Demographic, clinical and radiographic data
Romosozumab (N=52)
Vertebroplasty (N=32)
p-value
Age
72.38±8.26
74.82±7.80
0.404
Sex
0.792
Female
33(63.5%)
19(59.4%)
Male
19(36.5%)
13(40.6%)
BMI
26.86±2.80
25.88±2.20
0.111
BMD
-2.96±0.35
-3.04±0.40
0.564
Osteoporosis medication
35(67.3%)
19(59.4%)
0.512
OVCF history
20(47.6%)
19(55.9%)
0.486
Level of vertebral fracture
0.461
TL
35(67.3%)
19(59.4%)
Non-TL
17(32.7%)
13(40.6%)
Back pain VAS
7.70±1.01
7.65±1.06
0.782
ODI
69.70±8.42
69.80±9.46
0.988
Height of anterior vertebral body
15.70±3.34
15.82±5.57
0.902
BMI: body mass index, BMD: bone mineral density, OVCF: Osteoporotic vertebral compression fracture, TL: Thoracolumbar spine (T11-L2), non-TL: nonthoracolumbar spine (T5-T10 or L3-L5), VAS: Visual Analogue Scale, ODI: Oswestry Disability Index, Data are expressed as means±standard deviations.
*Indicates significance.
Table 2.
Clinical outcomes between groups
Romosozumab (N=52)
Vertebroplasty (N=32)
p-value
Back pain VAS
Before treatment
7.70±1.01
7.65±1.06
0.782
1-month after treatment
4.55±4.58
3.75±1.32
0.314
3-month after treatment
1.85±1.08
1.90±1.04
0.818
ODI
Before treatment
69.70±8.42
69.80±9.46
0.988
1-month after treatment
28.10±7.91
26.70±8.54
0.406
3-month after treatment
16.30±7.10
15.70±6.18
0.617
VAS; visual analogue scale, ODI; oswestry disability index, Data are expressed as means±standard deviations.
*Indicates significance.
Table 3.
Intergroup analysis of anterior vertebral body height
Romosozumab (N=52)
Vertebroplasty (N=32)
p-value
Height of anterior vertebral body
Before treatment
15.70±3.34
15.82±5.57
0.902
1-month after treatment
14.84±4.01
15.85±3.35
0.228
3-month after treatment
14.45±3.62
15.70±4.52
0.179
Data are expressed as means±standard deviations.
*Indicates significance
Table 4.
Longitudinal changes in anterior vertebral body height
Height of anterior vertebral body
Before treatment
1-month after treatment
3-month after treatment
p-value
Romosozumab
15.70±3.34
14.84±4.01
0.182
15.70±3.34
14.45±3.62
0.082
Vertebroplasty
15.82±5.57
15.85±3.35
0.940
15.82±5.57
15.70±4.52
0.905
Data are expressed as means±standard deviations.
*Indicates significance.
References
1. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001;285(6):785-95.
5. Suzuki N, Ogikubo O, Hansson T. The prognosis for pain and disability in patients with conservative treatment of acute osteoporotic vertebral fractures. Eur Spine J 2008;17(10):1380-5.
6. Kim SH, Kang KC, Shin SH, et al. Conservative treatment of acute osteoporotic vertebral compression fracture: a prospective study. J Korean Med Sci 2017;32(11):1734-40.
8. Lamy O, Burlet N, Aubry-Rozier B, et al. Underuse of osteoporosis treatment in elderly patients with recent vertebral fracture. Arch Osteoporos 2020;15(1):1-8.
9. Jung HJ, Kim MH, Kim HJ, et al. Quality of life in patients with osteoporotic vertebral compression fractures. J Bone Metab 2017;24(3):187-96.
11. Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 2009;361(6):557-68.
12. Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009;361(6):569-79.
13. Clark W, Bird P, Gonski P, et al. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicenter, randomized, double-blind, placebo-controlled trial. Lancet 2016;388(10052):1408-16.
15. Rousing R, Andersen MO, Jespersen SM, et al. Percutaneous vertebroplasty compared to conservative treatment in patients with painful osteoporotic vertebral body fractures: a randomized controlled trial. Spine 2009;34(13):1349-54.
16. Staples MP, Kallmes DF, Comstock BA, et al. Effectiveness of vertebroplasty using individual patient data from two randomized trials: meta-analysis. BMJ 2011;343:d3952.
19. Saag KG, Petersen J, Brandi ML, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis. N Engl J Med 2017;377(15):1417-27.
20. Langdahl BL, Libanati C, Crittenden DB, et al. Romosozumab vs teriparatide in postmenopausal women with osteoporosis transitioning from bisphosphonate therapy: a randomized trial. Lancet 2017;390(10102):1585-94.
23. Graeff C, Timm W, Nickelsen TN, et al. Monitoring structural changes in the lumbar spine in a randomized trial comparing teriparatide and risedronate. J Bone Miner Res 2007;22(10):1426-33.
Comparative Evaluation of Romosozumab and Vertebroplasty in Acute Osteoporotic Vertebral Compression Fractures
Fig. 1. Measurement of anterior vertebral body height.
Fig. 2. Change in VAS scores from baseline to 3 months.
Fig. 3. Change in ODI scores from baseline to 3 months.
Fig. 4. Change in anterior vertebral body height from baseline to 3 months.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Comparative Evaluation of Romosozumab and Vertebroplasty in Acute Osteoporotic Vertebral Compression Fractures
Romosozumab (N=52)
Vertebroplasty (N=32)
p-value
Age
72.38±8.26
74.82±7.80
0.404
Sex
0.792
Female
33(63.5%)
19(59.4%)
Male
19(36.5%)
13(40.6%)
BMI
26.86±2.80
25.88±2.20
0.111
BMD
-2.96±0.35
-3.04±0.40
0.564
Osteoporosis medication
35(67.3%)
19(59.4%)
0.512
OVCF history
20(47.6%)
19(55.9%)
0.486
Level of vertebral fracture
0.461
TL
35(67.3%)
19(59.4%)
Non-TL
17(32.7%)
13(40.6%)
Back pain VAS
7.70±1.01
7.65±1.06
0.782
ODI
69.70±8.42
69.80±9.46
0.988
Height of anterior vertebral body
15.70±3.34
15.82±5.57
0.902
Romosozumab (N=52)
Vertebroplasty (N=32)
p-value
Back pain VAS
Before treatment
7.70±1.01
7.65±1.06
0.782
1-month after treatment
4.55±4.58
3.75±1.32
0.314
3-month after treatment
1.85±1.08
1.90±1.04
0.818
ODI
Before treatment
69.70±8.42
69.80±9.46
0.988
1-month after treatment
28.10±7.91
26.70±8.54
0.406
3-month after treatment
16.30±7.10
15.70±6.18
0.617
Romosozumab (N=52)
Vertebroplasty (N=32)
p-value
Height of anterior vertebral body
Before treatment
15.70±3.34
15.82±5.57
0.902
1-month after treatment
14.84±4.01
15.85±3.35
0.228
3-month after treatment
14.45±3.62
15.70±4.52
0.179
Height of anterior vertebral body
Before treatment
1-month after treatment
3-month after treatment
p-value
Romosozumab
15.70±3.34
14.84±4.01
0.182
15.70±3.34
14.45±3.62
0.082
Vertebroplasty
15.82±5.57
15.85±3.35
0.940
15.82±5.57
15.70±4.52
0.905
Table 1. Demographic, clinical and radiographic data
BMI: body mass index, BMD: bone mineral density, OVCF: Osteoporotic vertebral compression fracture, TL: Thoracolumbar spine (T11-L2), non-TL: nonthoracolumbar spine (T5-T10 or L3-L5), VAS: Visual Analogue Scale, ODI: Oswestry Disability Index, Data are expressed as means±standard deviations.
Indicates significance.
Table 2. Clinical outcomes between groups
VAS; visual analogue scale, ODI; oswestry disability index, Data are expressed as means±standard deviations.
Indicates significance.
Table 3. Intergroup analysis of anterior vertebral body height
Data are expressed as means±standard deviations.
Indicates significance
Table 4. Longitudinal changes in anterior vertebral body height