This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Primary glioblastoma of the spinal cord is a rare and aggressive tumor, comprising less than 1.5% of spinal neoplasms. It typically affects young adult males and arises in the cervical or thoracic regions. We report an unusual case of intradural extramedullary spinal glioblastoma in a 62-year-old man with prior lymphoma in remission. The patient presented with a 7-month history of progressive lower limb weakness, numbness, and radiating pain. MRI revealed a contrast-enhancing mass at the T6–7 level, initially suspected as lymphoma. Surgical resection via total laminectomy was performed, and en-bloc tumor removal achieved. Histopathological analysis confirmed WHO grade IV glioblastoma, IDH-wildtype, without Histone H3 mutation. This case highlights an atypical radiologic and anatomical presentation, complicating preoperative diagnosis. Histopathologic and molecular studies were essential for confirmation. Postoperative treatment included adjuvant radiotherapy and temozolomide, though their efficacy remains uncertain in spinal glioblastoma due to limited evidence and spinal cord radiosensitivity. Early biopsy and a multimodal diagnostic approach are critical for managing rare spinal tumors presenting with nonspecific clinical and imaging features.
척수에서 발생하는 원발성 교모세포종은 드물고 공격적인 종양으로, 전체 척수 신생물의 1.5% 미만을 차지한다. 일반적으로 젊은 성인 남성에게 발생하며, 경추 또는 흉추 부위에서 흔히 나타난다. 본 보고에서는 관외 림프종 완해 병력이 있는 62세 남성에게 발생한 경막내 척수외 원발성 교모세포종의 드문 증례를 소개한다.
환자는 7개월에 걸쳐 점진적인 하지 근력 약화, 감각 저하, 방사통 증상을 보이며 내원하였다. MRI 검사에서 T6-7 수준에 조영 증강되는 종양이 발견되었으며, 초기에는 림프종으로 의심되었다. 후궁 절제술을 통해 종양을 일괄 절제하였고, 조직검사 결과 IDH-wildtype이며 Histone H3 돌연변이가 없는 WHO 등급 IV 교모세포종으로 진단되었다.
이 증례는 영상학적·해부학적으로 비전형적인 양상을 보여 수술 전 진단에 어려움이 있었으며, 확진을 위해 조직병리학적 및 분자 생물학적 검사가 필수적이었다. 수술 후 치료로 방사선 치료와 테모졸로마이드가 시행되고 있으나, 척수 교모세포종에 대한 이들의 치료 효과는 제한적인 근거와 척수의 방사선 민감성으로 인해 여전히 불확실하다.
비특이적인 임상 증상과 영상 소견을 보이는 드문 척수 종양의 진단과 치료를 위해서는 조기 생검과 다학제적 진단 접근이 중요하다.
Primary glioblastoma of the spinal cord is an exceedingly rare entity, accounting for approximately 1.5% of all spinal cord tumors and 1% to 5% of all glioblastomas.1,2) It most commonly affects young adult males3) and is predominantly located in the cervical and thoracic regions.4) Despite aggressive treatment, the prognosis remains poor, with reported average survival ranging from 10 to 14 months following diagnosis.5) Due to its extreme rarity, comprehensive studies on spinal cord glioblastoma are scarce, with most of the literature consisting of isolated case reports.
In this report, we describe a rare case of glioblastoma arising in the intradural extramedullary space of the thoracic spinal cord in an elderly patient with a prior history of lymphoma. The case illustrates the diagnostic challenges and therapeutic considerations involved in managing such an unusual presentation and underscores the importance of integrating histopathology, immunohistochemistry, and next-generation molecular testing in establishing an accurate diagnosis.
Case Presention
A 62-year-old male patient presented to our outpatient clinic with a 7-month history of bilateral leg numbness and motor weakness. He had a past medical history of lymphoma, which had been deemed in complete remission.
Neurological examination revealed generalized bilateral lower extremity weakness graded as motor grade IV, along with radiating pain. Both knee and ankle jerks were hyperreflexive.
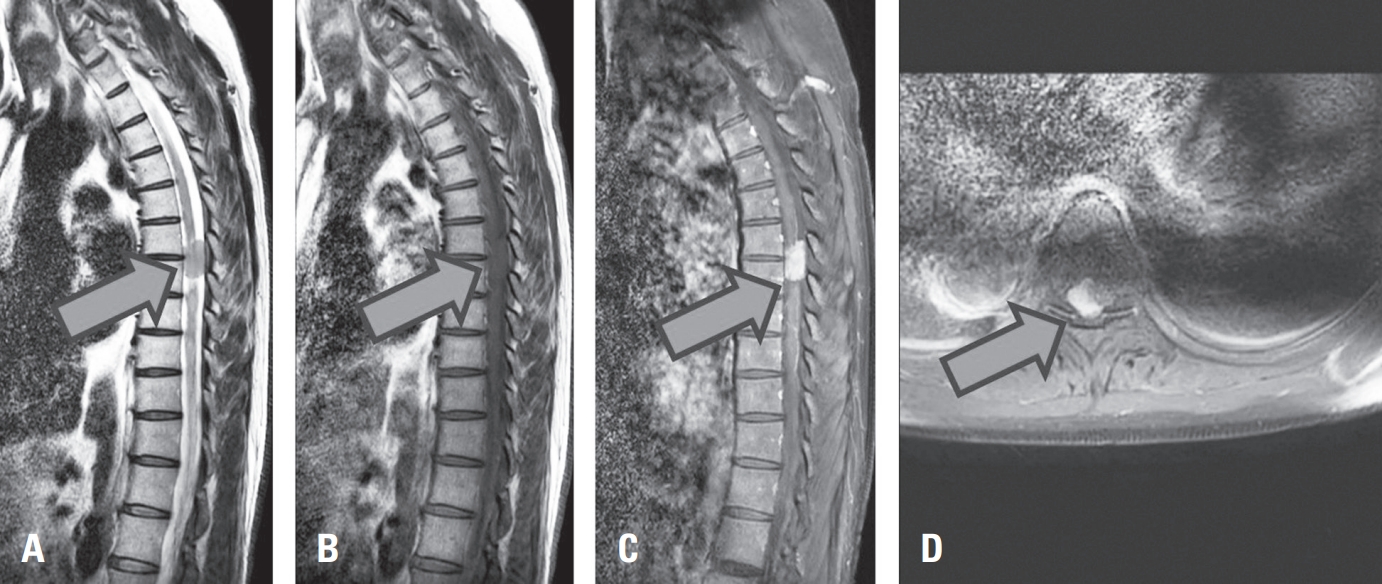
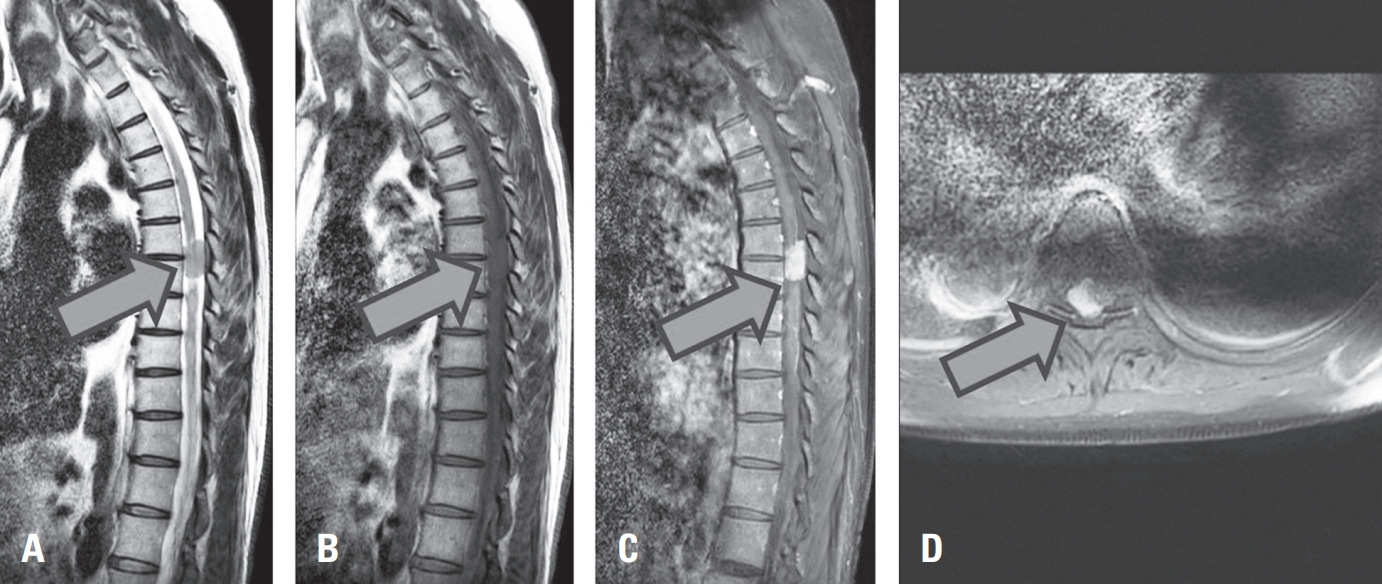
Initial thoracic spine X-ray and CT scans did not show any suspicious findings indicative of a tumor. However, thoracic spine MRI revealed an intradural extramedullary tumor measuring approximately 0.9×1.4×2.5 cm at the T6–7 level. The lesion appeared iso- to hypointense on T2-weighted images, isointense on T1-weighted images, and showed homogeneous enhancement on contrast-enhanced T1-weighted images. It was located at the posterolateral aspect of the spinal cord (Fig. 1. A-D).
Given the patient’s prior medical history, the possibility of lymphoma was considered. However, to relieve symptoms and obtain a definitive diagnosis, a near-total laminectomy at the T6–7 level was performed, followed by a longitudinal midline dural and pial incision.
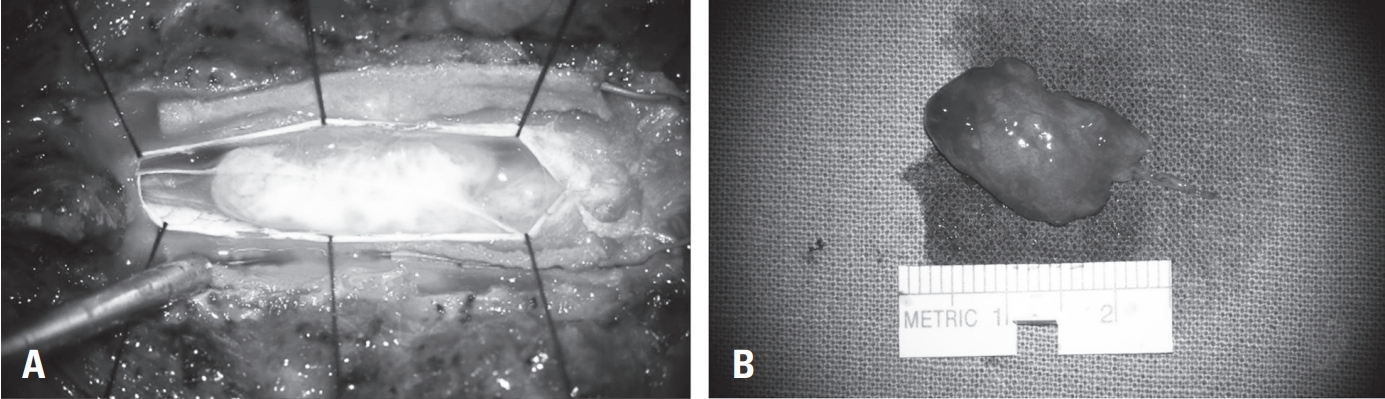
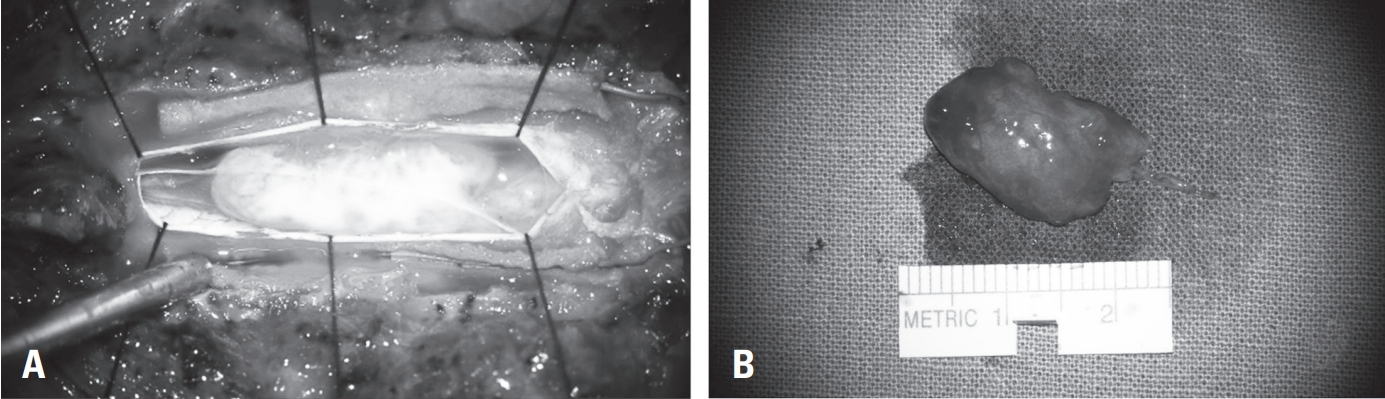
A yellowish, fragile tumor mass with a clearly defined margin from the medullary portion was exposed and subsequently removed en bloc (Fig.2. A, B).
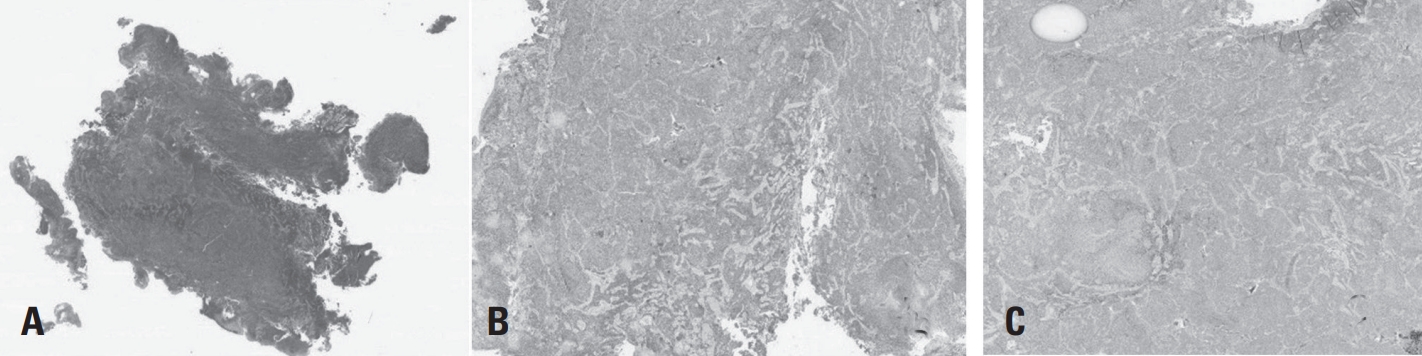
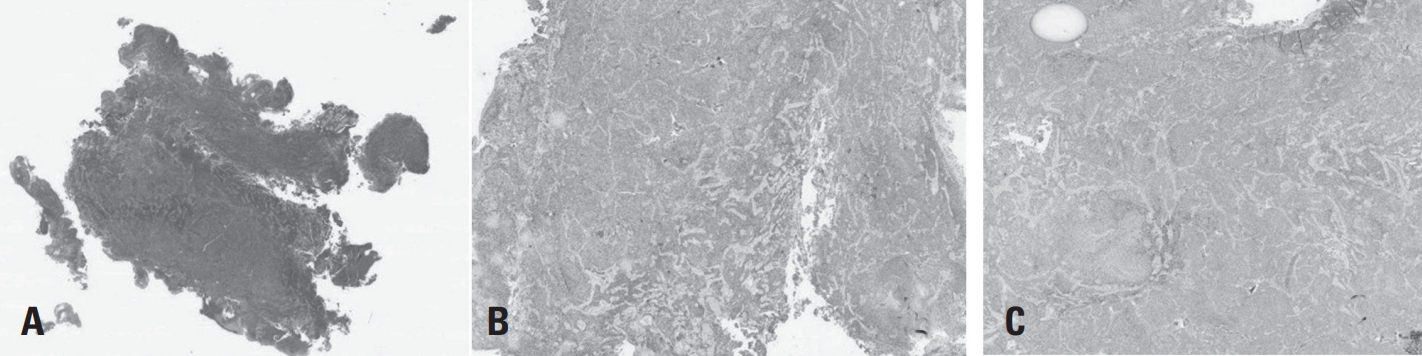
Histopathological examination revealed microvascular proliferation and necrosis on hematoxylin and eosin (H&E) staining. Immunohistochemical analysis confirmed a diagnosis of WHO grade IV glioblastoma, characterized by IDH wild-type status and absence of Histone H3 mutation (Fig. 3 A-C).
Discussion
Primary spinal cord tumors are anatomically classified into three categories: intradural intramedullary, intradural extramedullary, and extradural.6) Among adult cases, approximately 80% of spinal cord tumors are extramedullary.7) Of the intramedullary tumors, low-grade gliomas account for approximately 50% to 88%. As of 2018, fewer than 200 cases of intramedullary glioblastoma have been reported in the literature.8)
Unlike intracranial glioblastomas, spinal glioblasomas tend to occur more frequently in males and are most commonly observed in individuals in their 20s to 30s.9) In contrast, the present case involves a 62-year-old male with a prior history of lymphoma, who was diagnosed with a glioblastoma located in the intradural extramedullary compartment—a highly atypical presentation.
Spinal glioblasomas are known to arise in the cervicothoracic region in approximately 70% of cases,1,2,4) and lesions confined to the thoracic spine have been reported to be associated with a relatively better prognosis.10) The clinical manifestations of spinal glioblasomas vary depending on tumor location, with pain being the most commonly reported symptom.11)
In our case, the patient presented with a 7-month history of progressive motor weakness and radiating pain. Magnetic resonance imaging is considered the gold standard for diagnosis, with typical findings including hyperintensity on T2-weighted images and heterogeneous enhancement on contrast-enhanced T1-weighted images.9) However, in this case, the lesion appeared isointense on both T2- and T1- weighted images and exhibited homogeneous enhancement post-contrast, making preoperative suspicion of glioblastoma difficult. This highlights the necessity of histopathological confirmation for accurate diagnosis.
Only one previously reported case of glioblastoma arising in an intradural extramedullary spinal location exists in the literature, and that case also involved contrast enhancement along the cranial nerves. In that report, the authors were unable to determine whether the spinal glioblastoma represented the true site of origin or whether it was a metastatic lesion resulting from leptomeningeal spread.12) In our case as well, due to the nonspecific location and extreme rarity of the disease, diagnosis required the aid of histopathological evaluation, immunohistochemical analysis, and next-generation sequencing.
Glioblastoma is a high-grade astrocytic tumor that typically arises within the intramedullary compartment of the spinal cord, where glial cells reside. However, in this case, the tumor was radiologically and intraoperatively localized to the intradural extramedullary space, which is an exceptionally rare and anatomically incongruent site for glioblastoma. Several potential explanations should be considered for this discrepancy.
First, certain intramedullary gliomas may exhibit exophytic growth patterns, extending through the pial surface and appearing extramedullary on imaging or during surgery. In such cases, the tumor remains of glial origin but displaces the cord in a manner that mimics extramedullary tumors. Second, although unlikely in this case, leptomeningeal spread from an undetected primary lesion could result in secondary involvement of the extramedullary space. However, extensive imaging and pathological work-up in our case did not identify an alternative primary site.
The primary goal in the treatment of intradural extramedullary spinal tumors is the preservation and improvement of neurological function.13) Accordingly, the most critical surgical objectives are complete tumor resection and meticulous preservation of baseline neurological function. Intraoperative neurophysiological monitoring, including somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs), is particularly valuable in this context. Furthermore, preserving as much of the spinal bony structures and ligamentous elements as possible is essential for maintaining postoperative spinal stability and improving overall outcomes.13)
As a post-surgical treatment strategy, adjuvant radiotherapy combined with temozolomide—similar to the standard regimen for intracranial glioblastoma—is currently considered. Following concurrent chemoradiotherapy (CCRT), maintenance therapy with temozolomide is generally recommended.14) However, in spinal glioblastoma, the efficacy of this treatment approach has not been clearly established, and due to the radiosensitivity of the spinal cord, dose-limiting toxicity must be carefully considered.15)
Conclusions
This case highlights an extremely rare presentation of primary spinal cord glioblastoma arising in the intradural extramedullary compartment of the thoracic spine in an elderly patient. The atypical imaging features and the unusual tumor location made preoperative diagnosis difficult, requiring a comprehensive diagnostic approach including histopathology, immunohistochemistry, and molecular testing. Although treatment strategies often parallel those used for intracranial glioblastoma, their efficacy in spinal glioblastoma is not well established, and careful consideration must be given to the radiosensitivity of the spinal cord when planning adjuvant therapy. This report emphasizes the need for early tissue diagnosis and a multimodal treatment strategy in cases of rare spinal neoplasms, particularly when clinical and radiographic findings are inconclusive.
Fig. 1.
Preopertive MRI showing an intradural extramedullary tumor at the T6-7 level. (A) The lesion appears iso- to hypointense on T2WI (B) Isointense on T1W1 and (C, D) shows homogeneous enhancement on contrast-enhanced T1W1.
Fig. 2.
Intraoperative findings and gross apprearance of the tumor. (A) Intraoperative view showing the exposed yellowish, fragile tumor material following dural and pial incision. (B) The tumor mass was removed en bloc, demonstrating its soft and well-demarcated appearance.
Fig. 3.
(A) Hematoxylin and eosin (H&E) staining shows microvascular proliferation and necrosis, consistent with high-grade glioma. (B) Immunohistochemistry for IDH-1 reveals wild-type expression. (C) Immunohistochemistry for Histone H3 shows no mutation, supporting the diagnosis of IDH-wildtype glioblastoma.
2. Shen C.X., et al. Primary spinal glioblastoma multiforme: A case report and review of the literature. Medicine (Baltimore) 2017;96(16):p.e6634.
3. Yang K., et al. Clinical Features and Outcomes of Primary Spinal Cord Glioblastoma: A Single-Center Experience and Literature Review. World Neurosurg 2020;143:e157-e65.
5. Beyer S., et al. A Systematic Review on the Characteristics, Treatments and Outcomes of the Patients with Primary Spinal Glioblastomas or Gliosarcomas Reported in Literature until March 2015. PLoS One 2016;11(2):p. e0148312.
10. Raco A., et al. High-grade intramedullary astrocytomas: 30 years’ experience at the Neurosurgery Department of the University of Rome “Sapienza”. J Neurosurg Spine 2010;12(2):p. 144-53.
11. Farzin M., et al. Mixed malignant glioblastoma and schwannoma in spinal cord with metachronous ependymoma: A case report. Clin Case Rep 2021;9(6):p. e04162.
12. Shelton WJ, et al. A rare case of atypical intradural extramedullary glioblastoma diagnosed utilizing next-generation sequencing and methylation profiling: illustrative case. J Neurosurg Case Lessons 2024;7(16.
13. Arnautovic K., Arnautovic A.. Extramedullary intradural spinal tumors: a review of modern diagnostic and treatment options and a report of a series. Bosn J Basic Med Sci 2009;9 Suppl 1(Suppl 1):p.S40-s5.
15. Mallick S., Madan R., Julka P.K.. Primary spinal glioblastoma treated with adjuvant radiation and temozolomide: Report of two cases. J Cancer Res Ther 2015;11(3):p.654.
A Rare Case of Primary Spinal Glioblastoma Presenting as an Intradural Extramedullary Tumor in an Elderly Patient
Fig. 1. Preopertive MRI showing an intradural extramedullary tumor at the T6-7 level. (A) The lesion appears iso- to hypointense on T2WI (B) Isointense on T1W1 and (C, D) shows homogeneous enhancement on contrast-enhanced T1W1.
Fig. 2. Intraoperative findings and gross apprearance of the tumor. (A) Intraoperative view showing the exposed yellowish, fragile tumor material following dural and pial incision. (B) The tumor mass was removed en bloc, demonstrating its soft and well-demarcated appearance.
Fig. 3. (A) Hematoxylin and eosin (H&E) staining shows microvascular proliferation and necrosis, consistent with high-grade glioma. (B) Immunohistochemistry for IDH-1 reveals wild-type expression. (C) Immunohistochemistry for Histone H3 shows no mutation, supporting the diagnosis of IDH-wildtype glioblastoma.
Fig. 1.
Fig. 2.
Fig. 3.
A Rare Case of Primary Spinal Glioblastoma Presenting as an Intradural Extramedullary Tumor in an Elderly Patient