This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods
A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results
Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions
Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
본 연구의 목적은 흉요추부 골다공증 환자에서 시멘트 보강 척추경 나사못의 기계적 안정성을 평가하고, 비보강 나사못 고정술과 비교하여 기계적 실패를 감소시키는 효과를 분석하는 데 있다.
대상 및 방법
2011년부터 2022년까지 흉요추 유합술을 시행받은 119명의 환자를 대상으로 후향적 분석을 시행하였다. 시멘트 보강 척추경 나사못을 사용한 군과 보강을 시행하지 않은 군을 비교하여, 나사 이탈(pull-out), 나사 풀림(screw loosening), 케이지 돌출(cage protrusion)을 포함한 기계적 실패의 발생률을 분석하였다.
결과
시멘트 보강은 전체 기계적 실패 발생률을 유의하게 감소시키는 것과 연관되었다. 전체 기계적 실패의 발생률은 시멘트 보강군에서 비보강군에 비해 유의하게 낮았다(20.4% vs. 41.4%, p=0.018). 개별 합병증인 나사 이탈, 케이지 돌출, 나사 풀림은 모두 시멘트 보강군에서 발생 빈도가 낮았으나, 각각의 차이는 통계적으로 유의하지 않았다. 그러나 전체 기계적 실패의 감소는 통계적으로 유의하였다. 유합률은 시멘트 보강군에서 비보강군보다 높았으나, 그 차이는 통계적으로 유의하지 않았다(79.6% vs. 70.0%, p=0.337). 반면, 기계적 실패가 발생하지 않은 환자군은 실패가 발생한 환자군에 비해 유의하게 높은 유합률을 보였다(82.5% vs. 56.41%, p=0.0048).
결론
시멘트 보강 척추경 나사못은 골다공증 환자의 흉요추 유합술에서 기계적 실패의 위험을 유의하게 감소시킨다. 기계적 안정성은 유합 성공에 중요한 영향을 미치며, 이는 수술 결과를 최적화하기 위해 기계적 실패를 예방하는 것이 중요함을 시사한다. 본 연구 결과는 시멘트 보강이 척추경 나사못 고정의 내구성을 향상시키는 효과적인 전략임을 뒷받침하며, 골다공증 환자에서의 수술 계획 수립 시 고려되어야 할 방법임을 시사한다.
Pedicle screw fixation is a cornerstone of spinal fusion surgery, particularly in patients with osteoporosis, where bone fragility presents unique challenges.1) These screws provide essential stabilization within the spinal construct; however, their effectiveness is reduced in osteoporotic vertebrae because diminished bone density increases the risk of hardware failure, including screw loosening or pull-out.2)
Cement augmentation, which involves injecting polymethylmethacrylate into the pedicle to improve screw fixation, has emerged as a promising technique to increase pedicle screw pull-out strength.3) Although laboratory and limited clinical studies indicate that cement augmentation can substantially enhance fixation strength, robust real-world data on its long-term clinical effectiveness and durability remain limited. This knowledge gap hinders the widespread adoption of cement augmentation in clinical practice, particularly for managing spinal deformities and instabilities in patients with osteoporosis.
Existing biomechanical studies have primarily examined the pull-out strength of pedicle screws with cement augmentation. For example, one study comparing cannulated and solid screws reported that cement augmentation significantly increased pull-out strength compared with uncemented screws, with no meaningful difference between the two screw types.4) Another study assessed various screw shapes and thread profiles and similarly found that cement augmentation consistently improved pull-out strength, regardless of these design factors.5) However, these investigations were largely conducted using synthetic bone or cadaveric models, focusing on mechanical performance under controlled conditions. In contrast, our study evaluates clinical outcomes in patients, specifically addressing complications such as screw loosening, screw pull-out, and cage protrusion.
This study focuses on the mechanical failures associated with pedicle screw fixation, a critical issue given the substantial loads these screws must withstand during normal activities and postoperative physiotherapy. Mechanical failures— including screw loosening, pull-out, and the resulting spinal instability—can cause severe pain, reduced mobility, and often necessitate revision surgery, thereby significantly worsening patient outcomes.6,7)
Given these challenges, our study aims to rigorously assess the incidence of mechanical failures in two groups of patients undergoing thoracolumbar spinal fusion: those treated with cement-augmented pedicle screws and those treated without augmentation. By comparing these groups, we seek to quantify the protective effect of cement augmentation against mechanical failure. In addition, we aim to identify patient-related factors—such as bone mineral density, age, sex, and fusion level—as well as surgical variables that may influence failure risk.8) This comprehensive approach is intended to clarify the interplay between surgical techniques, patient characteristics, and clinical outcomes.
Materials and Methods
This retrospective study included 119 patients with osteoporosis (bone mineral density T-score <–2.5) who underwent thoracolumbar fusion surgery at a single medical center between 2011 and 2022. Eligible participants were those treated for degenerative conditions or trauma; patients with infections, tumors, or a history of fusion surgery were excluded. The study was approved by the Institutional Review Board of Inha University Hospital (Approval No. 2024-04-033) and classified as minimal risk. Approval was granted on May 7, 2024, with the requirement of annual reviews to ensure ongoing compliance with ethical standards.
1. Surgical Technique
All procedures were performed by a single experienced spine surgeon using an open, conventional technique. Pedicle screws with diameters ranging from 5.5 mm to 6.5 mm and lengths of 45 mm were used for spinal fixation. Cement augmentation was carried out with polymethylmethacrylate to improve screw stability in the osteoporotic vertebral body. The entry point was identified and tapped to determine screw trajectory, after which a Jamshidi needle was inserted. Under C-arm guidance, 2–5 mL of cement was injected while carefully monitoring to prevent leakage. Before the cement hardened, the pedicle screw was placed, and correct positioning was confirmed with imaging. The procedure emphasized meticulous preparation of the vertebral pedicle and controlled cement injection to minimize leakage and achieve secure screw fixation.9)
2. Assessment of Mechanical Failures
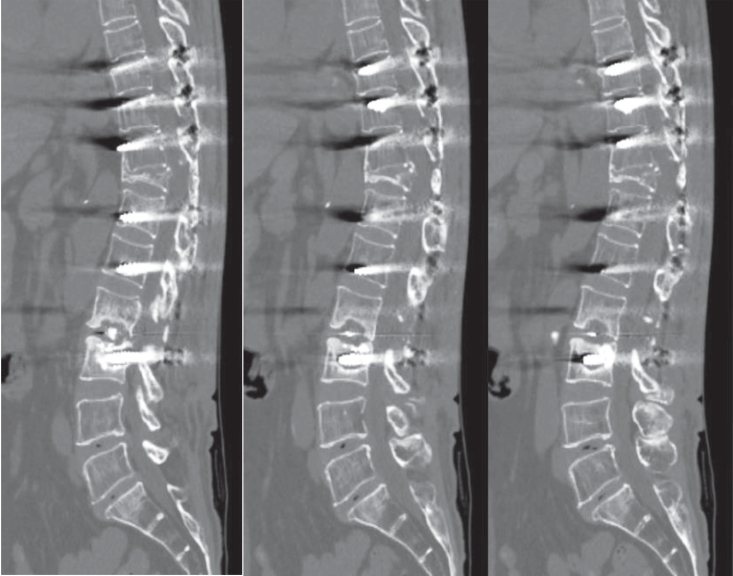
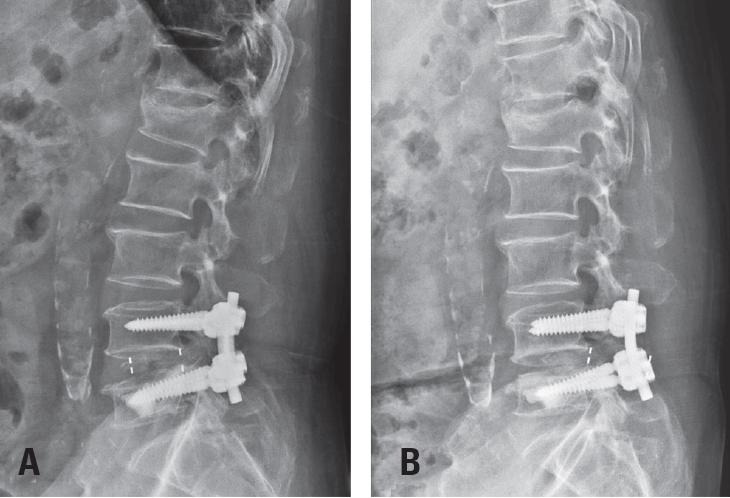
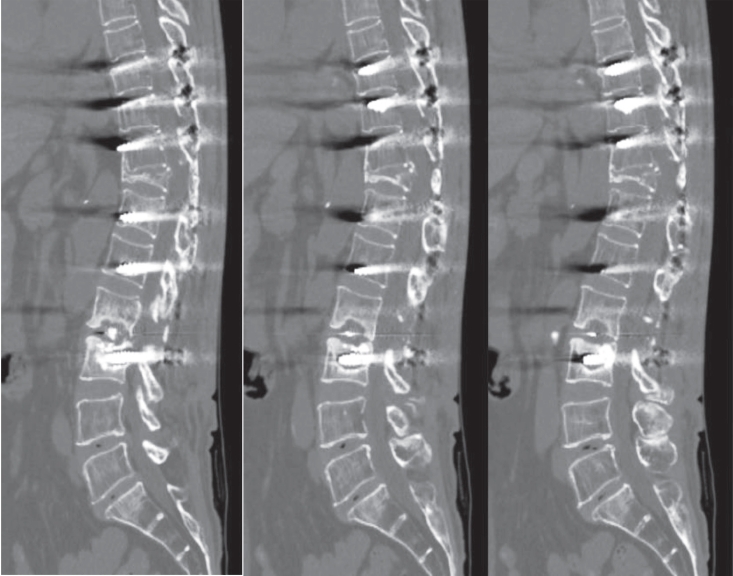
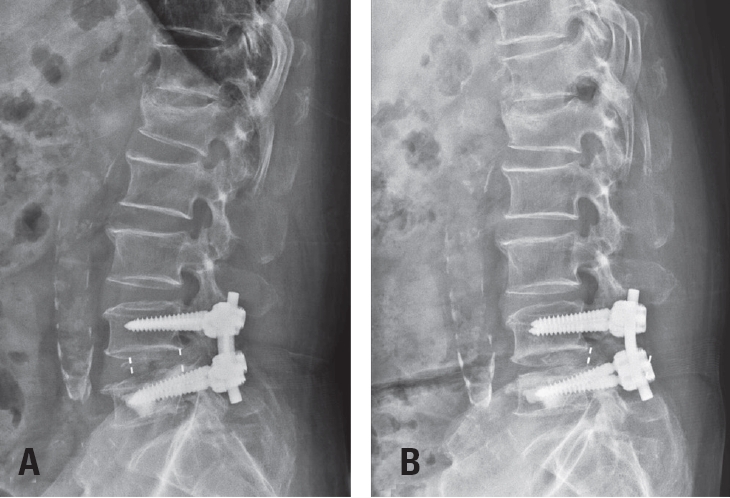
Postoperative imaging was essential for evaluating surgical outcomes. Standard radiographs and computed tomography (CT) scans were used to assess screw position and integrity. Mechanical failures—including pull-out and screw loosening—were identified by the appearance of a halo around the screw, indicating loss of fixation.10)Fig. 1 shows a typical pull-out, where the screw disengages from the vertebral body, whereas Fig. 2 demonstrates screw loosening, identified by the halo sign on CT imaging.
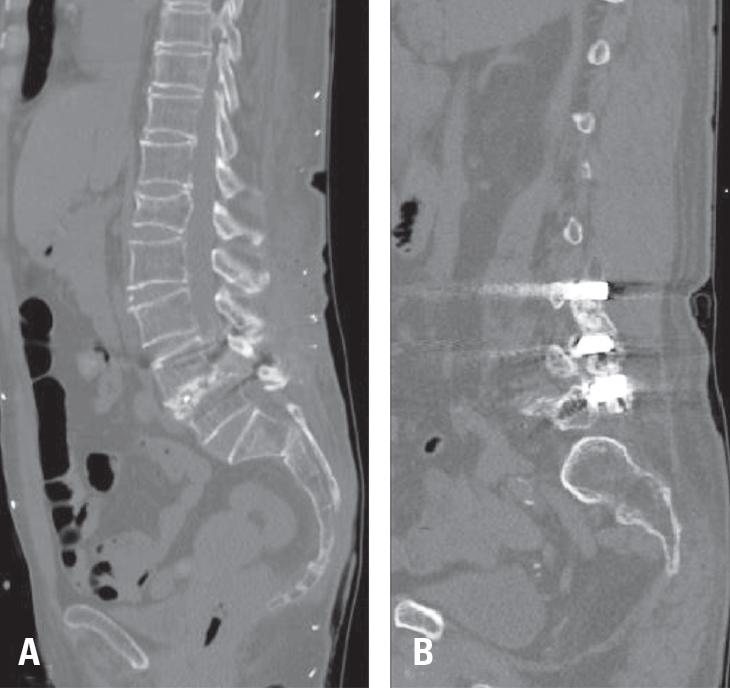
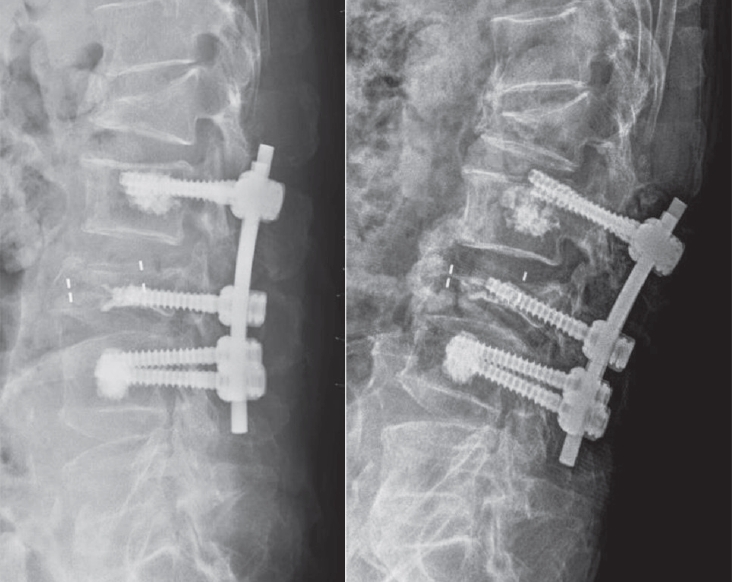
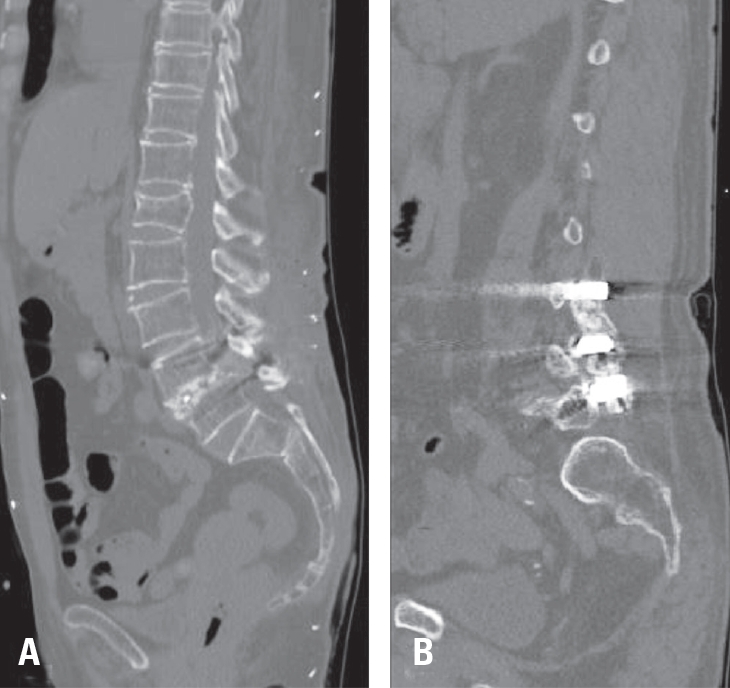
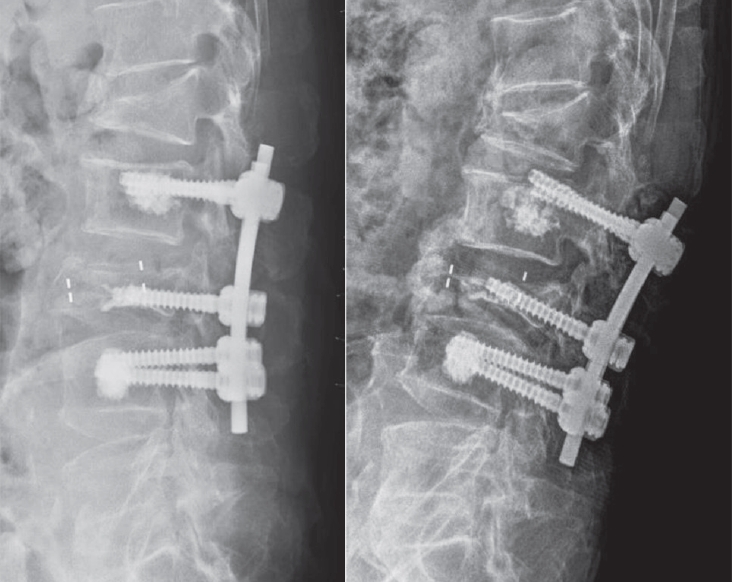
The incidence of mechanical failures was systematically recorded, comparing patients with cement-augmented pedicle screws to those without. Failures were classified into three categories: pull-out, screw loosening, and cage protrusion— the latter defined as displacement of the implanted cage beyond the vertebral body margins (Fig. 3). Fusion status was also evaluated using follow-up radiographs and CT scans. Successful fusion was defined as continuous bone bridging across the intervertebral space without radiolucent lines surrounding the implant. Representative CT images of successful fusion are shown in Fig. 4.
3. Statistical Analysis
Data analysis focused on the incidence of mechanical failures and related complications. Variables including age, sex, fusion level, bone mineral density, and follow-up duration were incorporated into the statistical models to allow comprehensive comparison between the two groups. Categorical variables were analyzed using the chi-squared test, whereas continuous variables were assessed with the t-test. A p-value <0.05 was considered statistically significant.
Results
1. Patient demographics and baseline characteristics
The patient cohort was statistically balanced between those who received cement-augmented pedicle screws and those who did not, ensuring comparability for outcome analysis. Table 1 summarizes the demographics and baseline characteristics of the study participants. The mean age was slightly higher in the cement group (75.16 years) than in the non-cement group (73.45 years), but this difference was not statistically significant (p=0.128). Sex distribution was comparable between groups, and no significant differences were observed in fusion level and bone mineral density, further supporting the similarity of the two cohorts. Both groups had bone mineral density values well below the osteoporosis threshold of –2.5, with a mean T-score of –3.52±0.67 in the cement group and –3.37±0.75 in the non-cement group.
2. Incidence of mechanical failures
A primary objective of this study was to compare the incidence of mechanical failures, defined as pull-out, cage protrusion, and screw loosening. Table 2 summarizes the distribution of these complications between the two groups. Overall, the cement-augmented group demonstrated a lower incidence of mechanical failures. Pull-out occurred in 4.1% of patients in the cement group compared with 7.1% in the non-cement group, although the difference was not statistically significant (p=0.698). Cage protrusion was also less frequent in the cement group (4.1% vs. 12.9%), with a trend toward reduction that did not reach statistical significance (p=0.122). Although these findings did not achieve statistical significance, they suggest that cement augmentation may enhance the stability of spinal constructs and merit further investigation. Fusion rates were higher in the cement-augmented group (79.6%) than in the nonaugmented group (70.0%), but again, the difference was not statistically significant (p=0.337).
2. Comparative analysis of outcomes
Table 3 presents the comparative analysis of outcomes, with significant findings regarding mechanical failures. Patients in the cement-augmented group had a markedly lower rate of mechanical failures (20.4%) compared with the non-augmented group (41.4%), a difference that was statistically significant (p=0.027). This supports a protective effect of cement augmentation in maintaining screw fixation, particularly in patients with osteoporosis. Fusion rates were also significantly higher in the group without mechanical failure (82.5%) compared with the group that experienced failure (56.41%, p=0.0048). Although fusion was more frequent in the cement-augmented group than in the nonaugmented group (79.6% vs. 70.0%), the difference did not reach statistical significance (p=0.337).
3. Multivariate logistic regression analysis
To identify factors associated with mechanical failure, a multivariate logistic regression model was applied. As summarized in Table 4, cement augmentation was found to significantly reduce the risk of mechanical failure (OR 0.279, p=0.006). In contrast, higher fusion levels were associated with a greater risk of mechanical failure (p=0.002), suggesting that more extensive surgical interventions may require additional stabilization measures such as cement augmentation.
These findings highlight the clinical value of cement augmentation in spinal surgery for patients with osteoporosis, supporting its role as a strategic approach to improve the durability of pedicle screw fixation.
Discussion
Numerous studies have consistently reported that patients with osteoporosis face a higher risk of suboptimal fusion outcomes and postoperative complications compared with patients without osteoporosis.11,12) Prior research has demonstrated increased rates of postoperative complications, including screw loosening and mechanical failure, and a greater need for reoperation in patients with osteoporosis, along with longer hospital stays and greater healthcare costs. Approximately 22.4% of these patients require additional fixation methods, which further elevate complication and reoperation rates.13) These disparities highlight the need for advanced fixation strategies, such as cement augmentation, to improve surgical outcomes in this vulnerable population.
Supporting the rationale for this study, a biomechanical investigation demonstrated that cement augmentation significantly increases the pull-out strength of pedicle screws in osteoporotic vertebrae. This study compared solid and fenestrated pedicle screws, with and without cement augmentation, and found that cement-augmented screws had significantly higher mean failure loads than non-augmented screws (p≤0.001). No significant difference in pull-out strength was observed between solid and fenestrated cemented screws. These results highlight the ability of cement augmentation to enhance screw stability in osteoporotic bone, thereby improving surgical outcomes in patients with compromised bone quality.14)
The findings of this study strengthen the understanding of cement augmentation as a means of enhancing the durability of pedicle screw fixation in osteoporotic thoracolumbar spines. Our analysis showed that cement-augmented pedicle screws significantly reduced the risk of mechanical failures, including screw loosening and cage protrusion—key concerns in spinal surgery for patients with osteoporosis. Fusion rates did not differ significantly between the cementaugmented and non-augmented groups. However, patients without mechanical failures demonstrated markedly higher fusion rates than those with failures, highlighting the importance of stable fixation in achieving successful fusion.
The lower incidence of mechanical failures in the cementaugmented group, even when some differences did not reach statistical significance, indicates a consistent trend toward improved surgical outcomes. This finding is particularly relevant in the context of an aging population and the rising prevalence of osteoporosis and its complications. The enhanced fixation provided by cement augmentation may lead to fewer postoperative complications, a reduced need for revision surgery, and ultimately better long-term outcomes for patients.
Although not all differences in mechanical failure rates reached statistical significance, the observed trends remain clinically meaningful. For instance, the non-significant reduction in pull-out rates in the cement group (4.1% vs. 7.1%, p=0.698) suggests a potential protective effect of cement augmentation. These findings highlight the need for larger, multicenter studies to confirm these trends and better define their implications for clinical practice.
The significant reduction in overall mechanical failures among patients with cement-augmented screws highlights the importance of accounting for patient-specific factors— such as bone quality and surgical history—when planning spinal fusion procedures. These findings support a tailored surgical approach in which the benefits of adjunctive measures like cement augmentation are carefully balanced against potential risks and complications.15) Importantly, no cases of cement leakage were observed in this study, reinforcing the safety of cement augmentation when performed with meticulous technique and intraoperative imaging guidance.
Moreover, the association between higher fusion levels and increased risk of mechanical failure highlights the complexity of surgical decision-making in patients with advanced osteoporosis. These findings suggest that more extensive procedures demand meticulous planning and may benefit from innovative strategies to improve spinal construct stability.
Despite its valuable insights, this study has several limitations. Its retrospective design and relatively small sample size may restrict the generalizability of the findings. Moreover, all procedures were performed by a single surgeon, which could limit broader applicability. The analysis also did not account for whether patients received osteoporosis treatment before or after surgery, a factor that may influence outcomes. In addition, the potential for selection bias and inability to fully control for confounding variables warrant caution when interpreting the results.
Future research should prioritize prospective studies with rigorous variable control and randomization to more clearly establish the causal relationship between cement augmentation and surgical outcomes. Long-term follow-up beyond the periods examined in this study is also needed to provide stronger evidence on the durability and safety of this technique.
Conclusions
In conclusion, this study demonstrates that cement augmentation significantly reduces the incidence of mechanical failures—including pull-out, cage protrusion, and screw loosening—in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical failures were significantly associated with non-augmented cases and longer fusion levels. Moreover, achieving stable fixation proved essential, as patients without mechanical failures had markedly higher fusion rates. Given the compromised bone quality in patients with osteoporosis, cement augmentation should be carefully considered, particularly in long-level fusions, to improve surgical outcomes and advance patient care in spinal surgery.
Fig. 1.
Postoperative radiograph demonstrating screw pull-out from the vertebral body.
Fig. 2.
Computed tomography scan showing screw loosening, identified by a visible halo around the screw. The arrow highlights the halo sign.
Fig. 3.
(A) Immediate postoperative radiograph showing pedicle screw and cage placement. (B) Follow-up radiograph at two months demonstrating cage protrusion, with the cage extending beyond the vertebral body margins.
Fig. 4.
Representative computed tomography images of successful spinal fusion. (A) Intervertebral space fusion with continuous bone bridging across the disc space. (B) Posterolateral fusion with bone formation along the posterolateral aspect of the spine.
Table 1.
Baseline characteristics of study participants
Variable
Cement-augmented group (n=49)
Control group (n=70)
p-value
Age (years)
75.16±6.74
73.45±5.36
0.128
Sex (M:F)
6:43
10:60
0.792
Fusion level (mean)
2.59±1.25
2.35±1.02
0.265
BMD (T-score)
–3.52±0.67
–3.37±0.75
0.291
Follow-up period (months)
27.38±24.36
28.81±20.88
0.733
*p<0.05.
M:F: male-to-female ratio, BMD: bone mineral density.
Table 2.
Comparison of complications and fusion rates according to cement augmentation
1. Bono CM, Lee CK. Critical analysis of trends in fusion for degenerative disc disease over the past 20 years: influence of technique on fusion rate and clinical outcome. Spine 2004;29:455-63.
2. Chen LH, Tai CL, Lee DM, Lai PL, Lee YC, Niu CC, et al. Pullout strength of pedicle screws with cement augmentation in severe osteoporosis: a comparative study between cannulated screws with cement injection and solid screws with cement pre-filling. BMC Musculoskelet Disord 2011;12:33.
3. Corona-Cedillo R, Saavedra-Navarrete MT, Espinoza-Garcia JJ, Mendoza-Aguilar AN, Ternovoy SK, Roldan-Valadez E. Imaging assessment of the postoperative spine: an updated pictorial review of selected complications. Biomed Res Int 2021;9940001, 2021.
4. Fan Z, Yan X, Li B, Shen E, Xu X, Wang H, et al. Prevalence of osteoporosis in spinal surgery patients older than 50 years: a systematic review and meta-analysis. PLoS One 2023;18:e0286110.
5. Kanno H, Onoda Y, Hashimoto K, Aizawa T, Ozawa H. Innovation of surgical techniques for screw fixation in patients with osteoporotic spine. J Clin Med 2022;11:2577.
6. Leichtle CI, Lorenz A, Rothstock S, Happel J, Walter F, Shiozawa T, et al. Pull-out strength of cemented solid versus fenestrated pedicle screws in osteoporotic vertebrae. Bone Joint Res 2016;5:419-26.
7. Liu MY, Tsai TT, Lai PL, Hsieh MK, Chen LH, Tai CL. Biomechanical comparison of pedicle screw fixation strength in synthetic bones: effects of screw shape, core/thread profile and cement augmentation. PLoS One 2020;15:e0229328.
8. Nishida K, Park H, Ogiri M, Rossi A. Clinical and economic outcomes of patients with osteoporosis undergoing spine fusion surgery in Japan. Spine Surg Relat Res 2023;8:163-70.
9. Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE. Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine 2004;29:1938-44.
10. Renner SM, Lim TH, Kim WJ, Katolik L, An HS, Andersson GBJ. Augmentation of pedicle screw fixation strength using an injectable calcium phosphate cement as a function of injection timing and method. Spine 2004;29:E212-E6.
11. Rohlmann A, Zander T, Bergmann G. Effects of fusionbone stiffness on the mechanical behavior of the lumbar spine after vertebral body replacement. Clin Biomech (Bristol, Avon) 2006;21:221-7.
12. Schmidt T, Ebert K, Rolvien T, Oehler N, Lohmann J, Papavero L, et al. A retrospective analysis of bone mineral status in patients requiring spinal surgery. BMC Musculoskelet Disord 2018;19:53.
13. Song Z, Zhou Q, Jin X, Zhang J. Cement-augmented pedicle screw for thoracolumbar degenerative diseases with osteoporosis: a systematic review and meta-analysis. J Orthop Surg Res 2023;18:631.
14. Tang YC, Guo HZ, Guo DQ, Luo PJ, Li YX, Mo GY, et al. Effect and potential risks of using multilevel cementaugmented pedicle screw fixation in osteoporotic spine with lumbar degenerative disease. BMC Musculoskelet Disord 2020;21:274.
15. Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood EA, Hanscom B, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 2008;358:794-810.
Reduction of Mechanical Failures After Thoracolumbar Fusion in Patients with Osteoporosis: The Role of Cement-Augmented Pedicle Screw
Fig. 1. Postoperative radiograph demonstrating screw pull-out from the vertebral body.
Fig. 2. Computed tomography scan showing screw loosening, identified by a visible halo around the screw. The arrow highlights the halo sign.
Fig. 3. (A) Immediate postoperative radiograph showing pedicle screw and cage placement. (B) Follow-up radiograph at two months demonstrating cage protrusion, with the cage extending beyond the vertebral body margins.
Fig. 4. Representative computed tomography images of successful spinal fusion. (A) Intervertebral space fusion with continuous bone bridging across the disc space. (B) Posterolateral fusion with bone formation along the posterolateral aspect of the spine.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Reduction of Mechanical Failures After Thoracolumbar Fusion in Patients with Osteoporosis: The Role of Cement-Augmented Pedicle Screw
Variable
Cement-augmented group (n=49)
Control group (n=70)
p-value
Age (years)
75.16±6.74
73.45±5.36
0.128
Sex (M:F)
6:43
10:60
0.792
Fusion level (mean)
2.59±1.25
2.35±1.02
0.265
BMD (T-score)
–3.52±0.67
–3.37±0.75
0.291
Follow-up period (months)
27.38±24.36
28.81±20.88
0.733
Cement-augmented group (n=49)
Control group (n=70)
p-value
Mechanical failure
10 (20.4%)
29 (41.4%)
0.018*
Pull-out
2 (4.1%)
5 (7.1%)
0.698
Loosening
2 (4.1%)
9 (12.9%)
0.122
Cage protrusion
6 (12.2%)
15 (21.4%)
0.229
Infection
1 (2.0%)
0 (0%)
0.412
Cement leakage
0 (0%)
0 (0%)
Fusion rate (total)
39 (79.6%)
49 (70.0%)
0.337
Variable
No mechanical failure (n=80)
Mechanical failure (n=39)
p-value
Age (years)
73.87±5.89
74.74±6.27
0.462
Sex (M:F)
10:70
6:33
0.776
Cement augmentation
39/80 (48.8%)
10/39 (25.6%)
0.018*
Fusion level
2.25±1.09
2.87±1.08
0.004*
BMD (T-score)
–3.37±0.74
–3.56±0.64
0.17
Follow-up period (months)
25.93±18.93
32.92±27.65
0.109
Fusion rate
66 (82.5%)
22 (56.41%)
0.0048*
Risk factor
p-value
Odds ratio
95% CI
Cement group
0.006*
0.279
0.111–0.7
Fusion level
0.002*
1.786
1.239–2.574
Table 1. Baseline characteristics of study participants
p<0.05.
M:F: male-to-female ratio, BMD: bone mineral density.
Table 2. Comparison of complications and fusion rates according to cement augmentation
p<0.05.
Table 3. Comparative analysis of mechanical failure
p<0.05.
M:F: male-to-female ratio, BMD: bone mineral density.
Table 4. Outcomes of the multivariate logistic regression model