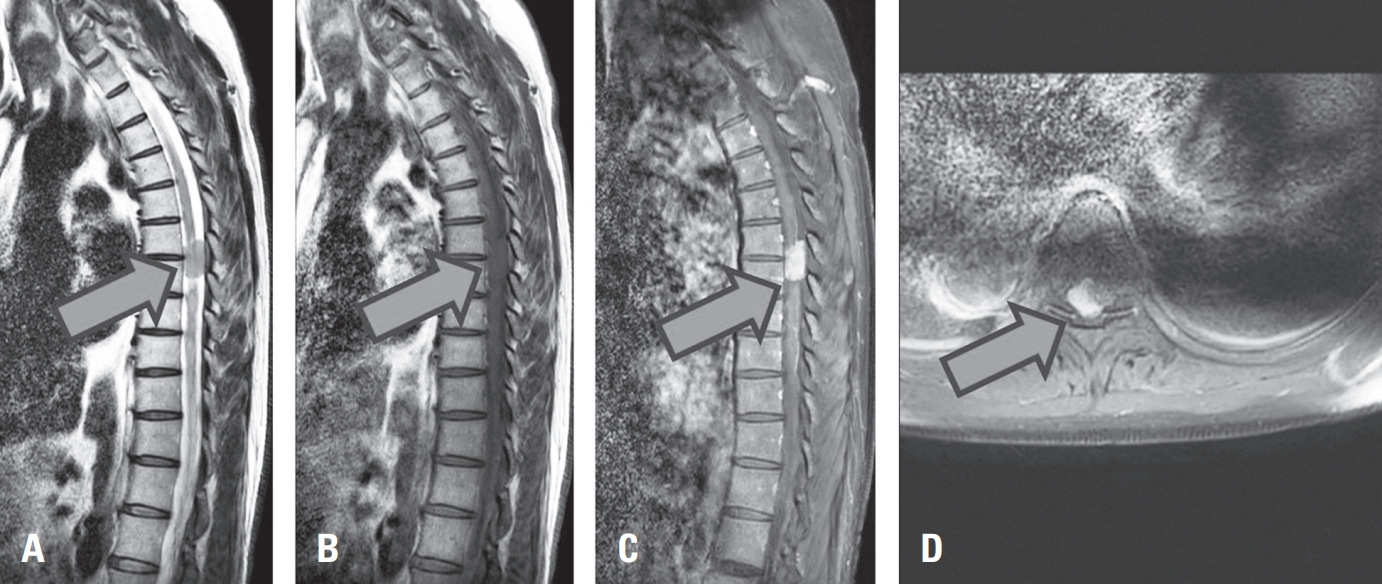
Primary glioblastoma of the spinal cord is a rare and aggressive tumor, comprising less than 1.5% of spinal neoplasms. It typically affects young adult males and arises in the cervical or thoracic regions. We report an unusual case of intradural extramedullary spinal glioblastoma in a 62-year-old man with prior lymphoma in remission. The patient presented with a 7-month history of progressive lower limb weakness, numbness, and radiating pain. MRI revealed a contrast-enhancing mass at the T6–7 level, initially suspected as lymphoma. Surgical resection via total laminectomy was performed, and en-bloc tumor removal achieved. Histopathological analysis confirmed WHO grade IV glioblastoma, IDH-wildtype, without Histone H3 mutation. This case highlights an atypical radiologic and anatomical presentation, complicating preoperative diagnosis. Histopathologic and molecular studies were essential for confirmation. Postoperative treatment included adjuvant radiotherapy and temozolomide, though their efficacy remains uncertain in spinal glioblastoma due to limited evidence and spinal cord radiosensitivity. Early biopsy and a multimodal diagnostic approach are critical for managing rare spinal tumors presenting with nonspecific clinical and imaging features.

 First
First Prev
Prev

