Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
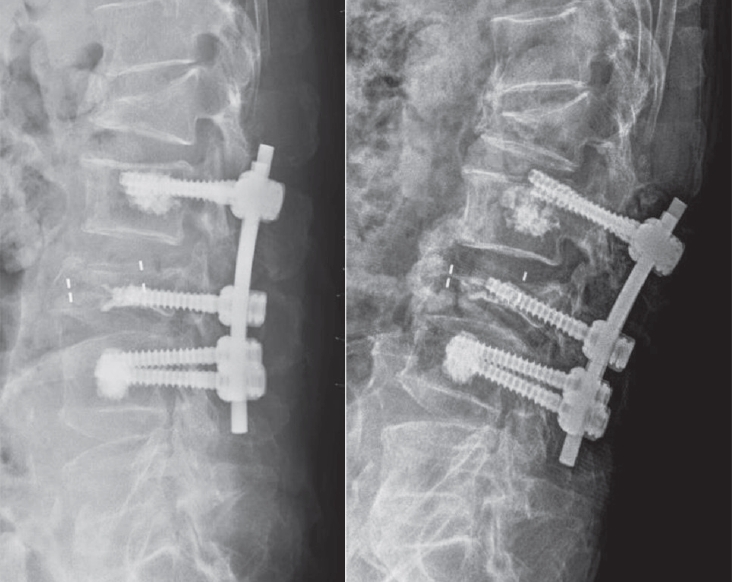
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.

 First
First Prev
Prev

