Study Design A retrospective comparative study.
Purpose This study aimed to evaluate the reliability of the external auditory meatus (EAM) as a reference point for determining the cranial center in patients with sagittal spinal deformity. Specifically, we assessed the radiographic visibility and spatial relationship of the EAM relative to the midpoint of the nasion-inion line (MNI) and compared it with the sella turcica.
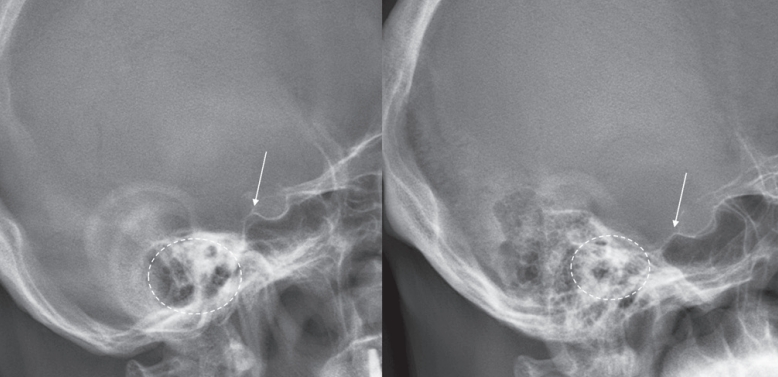
Overview of Literature: The cranial center is commonly defined as the midpoint of the nasion-inion line (MNI). The EAM has been widely used as an approximate surrogate of the MNI; however, its radiographic clarity and consistency are often limited. In contrast, the sella turcica is a singular anatomical structure that is more distinctly visualized on radiographic imaging.
Methods A total of 71 patients who underwent corrective surgery for spinal deformity between 2021 and 2024 were included. Preoperative full-spine radiographs were analyzed to evaluate the spatial relationship between both the EAM and the sella turcica relative to the MNI. Radiographic visibility was classified into three categories: single-point and clear, duplex but distinguishable, and unclear.
Results The EAM was located, on average, 1.1 mm posterior and 17.1 mm inferior to the MNI, whereas the sella turcica was located 13.8 mm anterior and 2.0 mm superior to the MNI. Relative to the femoral head axis, angular analysis revealed that the EAM exhibited a mean posterior tilt of 0.2°, while the sella turcica showed a mean anterior tilt of 1.3°. The sella turcica was clearly identifiable in 84.5% of cases, whereas the EAM was clearly visualized in only 14.1%, with the majority being either duplicated or indistinct (p<0.001).
Conclusions Although the EAM is anatomically closer to the MNI, its radiographic visibility and consistency are inferior to those of the sella turcica, thereby reducing its reliability as a cranial reference point. Further studies are needed to determine whether the sella turcica can serve as a more reliable alternative reference.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
Background Percutaneous-short segment screw fixation (SSSF) without bone fusion has proven to be a safe and effective modality for thoracolumbar spine fractures (TLSFs). When fracture consolidation is confirmed, pedicle screws are no longer essential, but clear indications for screw removal following fracture consolidation have not been established.
Methods In total, we enrolled 31 patients with TLSFs who underwent screw removal following treatment using percutaneous-SSSF without fusion. Plain radiographs, taken at different intervals, measured local kyphosis using Cobb’ angle (CA), vertebra body height (VBH), and the segmental motion angle (SMA). A visual analogue scale (VAS) and the Oswestry disability index (ODI) were applied pre-screw removal and at the last follow-up.
Results The overall mean CA deteriorated by 1.58º (p<0.05) and the overall mean VBH decreased by 0.52 mm (p=0.001). SMA preservation was achieved in 18 patients (58.1%) and kyphotic recurrence occurred in 4 patients (12.9%). SMA preservation was statistically significant in patients who underwent screw removal within 12 months following the primary operation (p=0.002). Kyphotic recurrence occurred in patients with a CA ≥20º at injury (p<0.001) with a median interval of 16.5 months after screw removal. No patients reported worsening pain or an increased ODI score after screw removal.
Conclusion Screw removal within 12 months can be recommended for restoration of SMA with improvement in clinical outcomes. Although, TLSFs with CA ≥20º at the time of injury can help to predict kyphotic recurrence after screw removal, the clinical outcomes are less relevant.

 First
First Prev
Prev

