Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
Adolescent idiopathic scoliosis refers to spinal deformity that develops from just before the onset of puberty until the completion of skeletal growth, and the primary goal of treatment is to achieve a well-balanced spine. In the late 1990s, advances in the anatomical understanding of the spine and the development of fixation instruments made posterior pedicle screw insertion feasible, thereby enabling the transmission of powerful corrective forces for deformity correction. Over the subsequent decades, accumulated clinical experience and outcomes have provided a deeper understanding of scoliotic curves and led to the establishment of effective principles for determining the extent of spinal fusion. However, these treatment principles are based on the unique biomechanics and procedural characteristics of scoliosis correction surgery, which can make them difficult to understand without sufficient explanation. In this review, we aim to describe these established treatment principles and surgical processes in detail using schematic illustrations and images. Although these principles will continue to undergo new challenges and validation over time, they will remain a meaningful reference point for those exploring alternative strategies.
Purpose To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
Methods An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
Background Neurogenic bladder dysfunction is a common and serious consequence of traumatic conus medullaris syndrome (T-CMS). Despite its clinical importance, predictive data for bladder outcomes after T-CMS remain limited. This study aimed to identify predictors of neurogenic bladder dysfunction at ≥2 years post-injury.
Methods We retrospectively reviewed 39 patients with acute T-CMS treated at a single level I trauma center from 2004–2017 who underwent spinal surgery and had ≥2 years of follow-up. Bladder function at 2 years was categorized as complete dysfunction, incomplete dysfunction, or normal. Potential predictors included demographic factors, injury mechanisms, ASIA Impairment Scale grades, MRI timing, fracture level and type, canal diameter, occupying ratio, conus signal change (normal, edema, or edema with hemorrhage), edema length, time to surgery, and surgical approach. Univariate and multivariate analyses were performed.
Results At final follow-up, 14 patients (35.9%) had complete bladder dysfunction, 12 (30.8%) had incomplete dysfunction, and 13 (33.3%) had normal function. Multivariate analysis identified edema with hemorrhage in the conus medullaris as the only independent predictor of bladder dysfunction.
Conclusions Bladder dysfunction is highly prevalent after T-CMS. Hemorrhagic edema in the conus medullaris significantly increases the risk of long-term neurogenic bladder dysfunction.
Purpose Metabolic syndrome is a multifactorial condition associated with increased risks of cardiovascular disease and type 2 diabetes. This study aims to evaluate whether combining AI-based abdominal CT metrics with traditional InBody analysis enhances the prediction of metabolic syndrome.
Materials and Methods This retrospective study included 977 adults who underwent both abdominal CT and InBody assessments. AI-derived measurements were obtained using a deep-learning V-Net model trained to segment seven body tissue types. InBody measurements included BMI, body fat percentage, fat mass, and waist-hip ratio. Metabolic syndrome was defined by NCEP-ATP III criteria. Logistic regression and ROC analyses were used to evaluate the predictive performance of AI-derived metrics, InBody metrics, and their combination.
Results Body fat percentage and waist-hip ratio from InBody analysis were strong predictors of metabolic syndrome (AUC 0.82). AI-derived visceral fat was also significantly associated with metabolic syndrome (AUC 0.61). Combining both AI and InBody metrics slightly improved predictive performance (AUC 0.83), indicating a complementary diagnostic value.
Conclusions While InBody metrics remain superior in predicting metabolic syndrome due to their close association with metabolic processes, AI-derived body composition metrics, particularly visceral fat, offer structural insights. The modest improvement in prediction when combined suggests the potential of an integrated diagnostic model in clinical practice.
Purpose To report an uncommon case of Opalski syndrome following traumatic C4–C5 facet dislocation with vertebral artery dissection, and to discuss its diagnostic and therapeutic implications.
Materials and Methods A 60-year-old woman presented after a motor vehicle collision with bilateral upper limb weakness. Cervical X-ray, CT, MRI, and CT angiography revealed C4–C5 facet dislocation and left vertebral artery occlusion. Urgent anterior cervical discectomy and fusion were performed, and the postoperative course was monitored.
Results Immediate postoperative improvement to 4/5 strength in both arms was noted; however, new left facial numbness appeared at 12 hours and left lower limb weakness with gait ataxia at 48 hours. Brain MRI confirmed left lateral medullary infarction, and aspirin therapy was initiated. At one month, left arm strength recovered to 4/5, but ataxia persisted.
Conclusions In cervical trauma patients with C4–C5 facet dislocation and vertebral artery injury on initial imaging, the possibility of delayed lateral medullary infarction—particularly Opalski syndrome—should be considered. Prompt brainstem imaging and tailored antithrombotic therapy are essential when new neurologic deficits arise.
Purpose To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
Material and Methods: This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Purpose The impact of skeletal muscle mass and bone mineral density (BMD) on frailty after osteoporotic vertebral fractures (OVFs) remains unclear. This study aimed to assess the interplay between frailty, skeletal muscle mass, and bone mineral density in OVFs.
Materials and Methods A total of 66 patients with osteoporotic vertebral compression fractures were enrolled. We collected clinical and radiological data, including age, body mass index (BMI), frailty index, and parameters such as lumbar lordosis, thoracic kyphosis, skeletal muscle mass, and BMD. We then analyzed the relationships between frailty and these variables.
Results The mean age, BMI, BMD T-score, skeletal muscle mass, and frailty index were 78.0±7.8 years, 22.3±3.3 kg/ m², -3.59±0.96, 37.84±6.24 kg, and 2.59±1.08, respectively. Of the 66 patients, 14 (21.1%) were frail prior to fracture, while 37 (56.1%) were frail after fracture, indicating a worsening frailty status. Specifically, 23 patients (34.8%) transitioned from pre-frail to frail following their fracture and had both lower BMD (T-score: -3.7±0.93) and lower skeletal muscle mass (35.74±3.83 kg). Frailty was negatively correlated with BMD (r=-0.28, p=0.02), while BMD was positively correlated with skeletal muscle mass (r=0.29, p=0.02). OVFs were positively correlated with frailty (r=0.33, p=0.01), especially in terms of fatigue (r=0.31, p=0.01) and ambulation (r=0.21, p=0.01).
Conclusions In patients with osteoporotic vertebral fractures, decreased muscle mass and low BMD appear to exacerbate frailty. Furthermore, frailty may be both a contributing and a resulting factor in the development of osteoporotic vertebral fractures.
Advanced imaging technologies have revolutionized the diagnosis and management of spinal pathologies by providing superior precision and efficiency. Modalities such as PET-CT, SPECT, diffusion tensor imaging (DTI), and magnetic resonance spectroscopy (MRS) offer unique insights into the metabolic, structural, and functional aspects of spinal diseases, enabling better differentiation of lesions, improved surgical planning, and early detection of pathological changes. Furthermore, the integration of artificial intelligence (AI) has enhanced imaging workflows by enabling automated analysis, prediction of clinical outcomes, and segmentation of spinal structures. Despite these advancements, challenges such as technical limitations, high costs, and ethical concerns, including issues of data privacy and AI-generated inaccuracies, hinder widespread adoption. This review explores the clinical applications, limitations, and future directions of these emerging technologies, highlighting the need for multidisciplinary collaboration and large-scale research to standardize protocols and optimize patient outcomes. The seamless integration of advanced imaging and AI represents a transformative potential for improving diagnostic accuracy and treatment efficacy in spinal care.
Objective To investigate the utility of a deep learning model in diagnosing traumatic lumbar fractures on computed tomography (CT) images.
Summary of Background Data: CT scans are widely used as the first choice for detecting spinal fractures in patients with severe trauma. Although CT scans have high diagnostic accuracy, fractures can occasionally be missed.
Recently, deep learning has been applied in various fields of medical imaging.
Methods CT images from 480 patients (3695 vertebrae) who visited a level-one trauma center with lumbar fractures were retrospectively analyzed. The diagnostic results were confirmed by two experienced musculoskeletal radiologists and one experienced spine surgeon using magnetic resonance imaging (MRI). Deep learning networks were employed for diagnosis, with 425 cases used for training and 55 cases for testing. Sensitivity, specificity, accuracy, and the area under the receiver operating characteristic curve (AUROC) were calculated to evaluate diagnostic performance.
Results The model successfully identified 107 out of 129 vertebrae with fractures, achieving a sensitivity of 82.95%, a specificity of 93.24%, an AUROC of 0.936, and an overall accuracy of 88.45%.
Conclusions This study demonstrated that the deep learning model showed high accuracy in diagnosing traumatic lumbar fractures. This approach has the potential to assist spine specialists, radiologists, and trauma care experts.
Further validation is needed to determine its effectiveness in clinical settings.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Objective To investigate stiffness-related disability (SRD) following surgical treatment in adolescent idiopathic scoliosis (AIS) patients particularly with respect to the lowest instrumented vertebra (LIV).
Summary of Background Extensive spinal fusion inevitably results in loss of mobility which may induce SRD during activities of daily living. Few studies have examined SRD after surgical correction for AIS.
Methods Patients who underwent surgical correction for AIS between 2014 and 2021 and were followed up for two years were included. The degree of SRD was evaluated using the Stiffness-Related Disability Index (SRDI) which consists of four categories, each containing three questions, giving a total of 12 components of the questionnaire.
The SRDI scores were compared according to the (LIV) levels. Correlation analysis was performed to examine the relationship between the SRDI and legacy health-related quality of life (HRQOL) measurements.
Results This study included 174 patients (47 males, 127 females) with a mean age of 13.8 years. Among the 12 items of the SRDI, the scores of nine items showed a significant increase after surgery. The total sum of the SRDI scores also significantly increased after surgery. Pearson correlation analysis showed that the SRDI scores were significantly correlated with ODI (Oswestry disability index), nearly all domains, and the total sum of SRS-22 (Scoliosis Research Society-22 questionnaire), and SF-36 (Short Form 36 health questionnaire). No differences in the SRDI score were found among cases with the LIV between T12 and L3. However, The SRDI scores of patients with LIV at L4 were significantly higher than those of patients with other LIV levels. .
Conclusions Various degree of SRD occurred after spinal fusion for AIS. The SRDI significantly correlated with the HRQOL measures. The SRDI score was highest in patients with the LIV at L4 compared to those with other LIV levels.
Background This study aims to assess the clinical and radiographic outcomes of biportal endoscopic lumbar discectomy compared to microscopic lumbar discectomy in obese patients with lumbar herniated discs. Previous research has established a positive correlation between operation time and estimated blood loss in obese patients undergoing microscopic lumbar discectomy, based on an increase in body mass index. However, no studies have specifically examined the outcomes of biportal endoscopic lumbar discectomy in this patient population. Therefore, this study seeks to fill this research gap and provide valuable insights into the effectiveness of these two surgical approaches for obese patients with lumbar herniated discs.
Methods This retrospective multicenter study analyzed and compared clinical and radiological data from 48 obese patients with a body mass index (BMI) greater than 30 kg/m2 who underwent either microscopic or biportal endoscopic lumbar discectomy. The study assessed clinical outcomes using the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores. Radiological data were obtained through magnetic resonance imaging (MRI) scans.
Results The study included a total of 48 patients, with 31 patients undergoing microscopic discectomy and 17 patients undergoing biportal endoscopic discectomy. Both groups showed improvements in VAS, ODI, and EQ-5D scores following surgery compared to preoperative scores. However, there was no significant difference in these outcome measures between the two surgical techniques. Although there was a no significant difference in the occurrence of recurrent disc herniation confirmed by postoperative MRI, there was significant difference in the number of patients requiring additional surgery between the two groups.
Conclusions For obese patients with lumbar disc herniation that did not respond to conservative treatment, this study found no significant differences in clinical or radiological outcomes between microscopic and biportal endoscopic surgery methods. However, it is worth noting that the biportal group had a lower incidence of reoperation compared to the microscopic group.
Objective Proximal junctional fracture (PJFx) at the uppermost instrumented vertebra (UIV) or UIV+1 is the most common mechanism of PJF. There are few studies assessing the radiographic progression after PJFx development.
Therefore, this study sought to identify the risk factors for radiographic progression of PJFx in surgical treatment for ASD.
Methods In this retrospective study, among 317 patients aged > 60 years who underwent ≥5-level fusion from the sacrum, 76 with PJFx development were included. According to the change in proximal junctional angle (PJA), two groups were created: Group P (change ≥10°) and Group NP (change <10°). Patient, surgical, and radiographic variables were compared between the groups to demonstrate risk factors for PJFx progression using uni- and multivariate analysis. The receiver operating characteristic (ROC) curve was used to calculate cutoff values. Clinical outcomes, such as visual analog scale (VAS) scores for back and leg pain, the Oswestry Disability Index (ODI) score, and the Scoliosis Research Society (SRS)-22 score, and revision rate were compared between the two groups.
Results The mean age at the index surgery was 71.1 years, and there were 67 women enrolled in the study (88.2%).
There were 45 patients in Group P and 31 in Group NP. A mean increase of PJA was 15.6° (from 23.2° to 38.8°) in Group P and 3.7° (from 17.2° to 20.9°) in Group NP. The clinical outcomes were significantly better in Group NP than Group P, including back VAS score, ODI value, and the SRS-22 scores for all items. Revision rate was significantly greater in group P than in group NP (17.8% vs. 51.6%, p=0.001). Multivariate analysis revealed that overcorrection relative to the age-adjusted ideal pelvic incidence (PI)–lumbar lordosis (LL) target at the index surgery (odds ratio [OR]=4.484, p=0.030], PJA at the time of PJFx identification (OR=1.097, p=0.009), fracture at UIV versus UIV+1 (OR =3.410, p=0.027) were significant risk factors for PJFx progression. The cutoff value of PJA for PJFx progression was calculated as 21° using the ROC curve.
Conclusions The risk factors for further progression of PJFx were overcorrection relative to age-adjusted PI–LL target at the index surgery, PJA > 21° at initial presentation, and fracture at the UIV level. Close monitoring is warranted for such patients not to miss the timely revision surgery.
After posterior cervical arthrodesis, many problems can arise, including adjacent segment degeneration and the related adjacent segment disease (ASD). As indicated by studies on the causes of ASD, posterior cervical arthrodesis can produce biomechanical and kinematic changes in adjacent unfused segments due to inappropriate forces.
Several studies have been conducted to determine the appropriate lowest instrumented vertebra, specifically regarding whether to cross the cervicothoracic junction via extension of long-segment posterior cervical fusion. We searched for relevant articles in electronic databases including PubMed, the Cochrane Registry, Embase, and Ovid.
Five meta-analyses were reviewed on this topic. Among these, Goyal et al. (2019), Rajjoub et al. (2022), and Chang et al. (2022) argued that ending instrumentation at the cervical level was associated with higher rates of ASD and reoperation. However, Truumees et al. (2022) and Coban et al. (2022) found no statistically significant differences between cases of instrumentation ending at the cervical and thoracic levels in the rates of ASD and requirement of revision surgery. Cervicothoracic junction breakage is a known possibility after cervical spine surgery because of the anatomical fragility of the junction. Terminating at the thoracic level reduces the stress on the cervicothoracic junction, thereby decreasing complications such as cervicothoracic junction breakage and lowering the frequency of reoperation. Based on the findings published to date, instrumentation across the cervicothoracic junction can be reasonably recommended in cases of multilevel posterior cervical fusion based on the lower reoperation and higher fusion rate.
Background The Selective thoracic fusion (STF) may be associated with risk of postoperative coronal decompensation, lumbar decompensation and adding-on phenomenon, which can lead to persistence of the lumbar curve and consequently to deviation of the trunk. Therefore, the STF is the most debatable issue as the optimal surgical correction in adolescent idiopathic scoliosis with Lenke 1C curves.
Methods A total of 30 patients with adolescent idiopathic scoliosis with Lenke 1C curves who underwent STF between 1996 and 2017 were included. Minimum follow-up duration was five years. We analyzed the incidence of coronal decompensation, lumbar decompensation, distal adding-on phenomenon and trunk shift in these patients for radiographic adverse event. Clinical outcome was assessed by using the Scoliosis Research Society (SRS)-22r scores.
Results The mean age at the time of surgery was 13.8±2.9 years. The mean follow-up duration was 80.4±12.3 months.
The Cobb’s angle for main thoracic curve improved by 59.6% (p<0.001), and also The Cobb’s angle for thoracolumbar/ lumbar curve improved by 40.5% comparing preoperative and postoperative values (p<0.001). There was significant improvement in the Cobb’s angle for main thoracic and Thoracolumbar/lumbar curve comparing preoperative and last follow-up values (p<0.001). At last follow-up, the coronal balance was 10.3 ± 9.1 that significant improved from the immediate postoperative value (p=0.033). The incidence of coronal decompensation, lumbar decompensation, adding-on and trunk shift in our cohort was 16.7%, 10.0%, 13.3% and 10.0% respectively. The average SRS score at last follow-up in patients with radiographic adverse events was 4.3±0.5. That of patients without adverse events was 4.4±0.6. All domains between patients with and without adverse events had no statistical significance difference.
Conclusions Selective thoracic fusion in Lenke 1C curves have acceptable risk of coronal decompensation, lumbar decompensation, distal adding-on, trunk shift. However, no revision surgery was required in these patients after long term follow-up. Therefore, STF in Lenke 1C curves seems to be enough.
Background It is well reported that the patient’s age plays an important role associated with proximal junctional failure (PJF) development. Various characteristics of adult spinal deformity (ASD) patients were different between younger and older age groups. We hypothesized that the radiographic risk factors for PJF would different according to younger and older age groups. This study aimed to evaluate different radiographic risk factor of PJF according to the two age groups undergoing thoracolumbar fusion for ASD.
Methods ASD patients aged ≥ 60 years who underwent thoracolumbar fusion from low thoracic level (T9~T12) to sacrum were included. The minimum follow-up duration was two years. PJF was defined as proximal junctional angle (PJA) ≥ 20°, fixation failure, fracture, myelopathy, or necessity of revision surgery. Using various radiographic risk factors including age-adjusted ideal pelvic incidence (PI)-lumbar lordosis (LL), univariate and multivariate analyses were performed separately according to the two age groups : <70 years and ≥70 years.
Results A total of 186 patients were enrolled (mean age=68.5 years old, 90.3% female). Mean follow-up duration was 67.4 months. PJF developed in 98 patients (32.0%). There were fracture in 53 patients, PJA ≥ 20° in 26, fixation failure in 12, and myelopathy in 6. PJF developed more frequently in patients older than 70 years than in younger than 70 years. In patients aged less than 70 years, preoperative LL, PI-LL and change in LL were significant risk factors in univariate analysis. Multivariate analysis showed only change in LL was significant for PJF development (Odds ratio [OR]=1.025, p=0.021). On the other hand, in patients older than 70 years, postoperative LL, postoperative PILL, overcorrection relative to conventional PI-LL target (within ±10°) as well as age-adjusted ideal PI-LL target were significant. On multivariate analysis, only overcorrection of PI-LL relative to age-adjusted ideal target was a single significant factor to cause PJF (OR=5.250, p=0.024).
Conclusions In patients younger than 70 years, greater change in LL was associated with PJF development regardless of PI-related value. However, in older patients, overcorrection of PI-LL relative to the age-adjusted PI-LL target was important to cause PJF.
Background When obese patients underwent lumbar discectomy using a microscope, a correlation was found between the operation time and an increase in estimated blood loss according to the increase in body mass index.
However, except for minor complications, there was no difference in postoperative outcomes between obese and normal-weight patients. These are the results of microscopic lumbar discectomy in obese patients, but there are no studies on biportal endoscopic lumbar discectomy. The aim of this study was to compare the clinical and radiographic outcomes of microscopic and endoscopic discectomy in obese patients.
Methods Clinical and radiological data were compared and analyzed in 23 obese patients with a body mass index of >30 kg/m2 who underwent microscopic and biportal endoscopic lumbar discectomy. Clinical data on the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores were measured, and radiological data were measured using magnetic resonance imaging (MRI).
Results In total, 13 patients who underwent microscopic discectomy and 10 who underwent biportal endoscopic discectomy were enrolled in this study. The VAS, ODI, and EQ-5D scores in both groups improved after surgery compared with those before surgery, although there was no difference between the two groups. Although there was a difference in the incidence of recurrent disc herniation confirmed by MRI after surgery, there was no difference in the number of patients requiring surgery between the two groups.
Conclusions There were no significant clinical or radiological differences in outcomes between microscopic and biportal endoscopic surgery methods.
Background Percutaneous-short segment screw fixation (SSSF) without bone fusion has proven to be a safe and effective modality for thoracolumbar spine fractures (TLSFs). When fracture consolidation is confirmed, pedicle screws are no longer essential, but clear indications for screw removal following fracture consolidation have not been established.
Methods In total, we enrolled 31 patients with TLSFs who underwent screw removal following treatment using percutaneous-SSSF without fusion. Plain radiographs, taken at different intervals, measured local kyphosis using Cobb’ angle (CA), vertebra body height (VBH), and the segmental motion angle (SMA). A visual analogue scale (VAS) and the Oswestry disability index (ODI) were applied pre-screw removal and at the last follow-up.
Results The overall mean CA deteriorated by 1.58º (p<0.05) and the overall mean VBH decreased by 0.52 mm (p=0.001). SMA preservation was achieved in 18 patients (58.1%) and kyphotic recurrence occurred in 4 patients (12.9%). SMA preservation was statistically significant in patients who underwent screw removal within 12 months following the primary operation (p=0.002). Kyphotic recurrence occurred in patients with a CA ≥20º at injury (p<0.001) with a median interval of 16.5 months after screw removal. No patients reported worsening pain or an increased ODI score after screw removal.
Conclusion Screw removal within 12 months can be recommended for restoration of SMA with improvement in clinical outcomes. Although, TLSFs with CA ≥20º at the time of injury can help to predict kyphotic recurrence after screw removal, the clinical outcomes are less relevant.
Purpose Minimally invasive technique in spinal surgery have evolved including cortical bone trajectory (CBT) screw technique which is s new lumbar pedicle screw path, as an alternative fixation technique for lumbar spine.
Theoretical advantage is that it provides enhanced screw torque and has biomechanical characteristics, also it minimizes approach-related damages. Midline lumbar fusion (MIDLF) has appeared with CBT screw technique.
Many studies of CBT screw reported the effectiveness of MIDLF. We adopted this technique for lumbar degenerative spondylolisthesis and evaluated early radiological outcomes.
Materials and Methods From May 2014 to March 2015, 17 patients (mean age 65.6±7.5 years; 4 males, 13 females) underwent MIDLF procedures for the treatment of single level lumbar spondylolisthesis. Average follow-up period was 8.8±2.7 months. Initial and last follow-up X-ray and computed tomography (CT) were evaluated for screw malposition, detection of peri-screw halo, loosening of the construct, or signs of spinal instability.
Results The average bone mineral density (BMD) was -1.9±0.8. Eleven patients were fused at L4-5, 5 were at L3-4, and 1 was at L2-3. Five CBT screws were converted into pedicle screws due to intraoperative misposition of screws, so total 63 CBT screws were evaluated for peri-screw halo and malposition. There were no findings of screw pull-out or breakage in all screws. Four out of 63 (6.3%) screws were judged as peri-screw halo, and 20 (41.2%) screws were judged as malposition (1 medial; 2 superior; 17 lateral pedicle violation). But, there were no screw related nerve root injury. In all cases, interbody bony mass were identified. Four out of 17 (23.6%) patients were detected more than 2 degrees motions on flexion-extension lateral X-rays at final follow-up, and 1 out of these 4 patients was identified loss of reduction. There was no operation related complication.
Conclusion There is no doubt that MIDLF with CBT screw is the minimally invasive method. Many numbers of screw malposition identified in our series were thought to be due to our earlier experience of trying free hands technique.
We recommend the use of intraoperative fluoroscopy, which achieve accuracy. Although MIDLF with CBT has theoretical strengths, we must evaluate further long-term clinical follow-up and measure outcome.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Background Oblique and anterior lumbar interbody fusion have been widely performed in the lumbar spinal disease but we cannot get a direct decompression effect with these procedure.
Objective: The purpose of this study is to report clinical and imaging outcomes of microscope assisted direct decompression combined with oblique lumbar interbody fusion (OLIF) or anterior lumbar interbody fusion (ALIF).
Methods Twelve patients who received microscope assisted direct decompression during OLIF or ALIF for lumbar spinal stenosis were enrolled. The OLIF was performed for the lesion upper than the L4-5 or in the case of multisegmental disease. The ALIF was performed for the lesion at the L5-S1. After anterior-approaching surgery, percutaneous fixation of pedicle screw was performed and we did not perform an additional decompression posteriorly in all cases. For the clinical outcomes, we evaluated short form 36 (SF-36), Oswestry disability index (ODI) score and visual analog scale (VAS) pain score. For the imaging outcomes, we obtained postoperative lumbar magnetic resonance imaging (MRI).
Results The OLIF was performed for 9 patients and the ALIF was performed for 3 patients. In the clinical outcomes, SF-36 was improved from 25.40 to 69.83 and ODI score was also improved from 69.83 to 16.50. VAS pain score of back was improved from 4.3 to 1.6 and VAS pain score of leg was improved from 7.5 to 2.2. In the imaging outcomes, all patients had severe stenosis before surgery. After surgery the severity of the stenosis was reduced to mild state in 9 cases and moderate state in 3 cases postoperatively.
Conclusions We could obtain the good clinical outcomes and effective decompression through microscope assisted direct decompression during OLIF or ALIF.
Purpose The current study aims to report the results of analyzed factors that ultimately undergo surgical treatment after selective nerve root block in patients with spinal structural pathology that cause lower back pain and radiating pain in the lower extremities.
Material and methods: A retrospective study was performed on 537 patients diagnosed with spinal canal stenosis or disc herniation among patients who underwent selective nerve root block at our hospital for five years from May 2015 to December 2017. The patients were divided into Group A (patients with an only selective spinal nerve root, n=99) and Group B (patients with surgical treatment, n=20). We evaluated the primary demographic factors, including age, sex, onset, symptom duration, diabetes mellitus, hypertension, angina, osteoporosis. The clinical variables included in the analysis were the preoperative visual analog scale (VAS) pain score, the Korean version of the Oswestry Disability Index (K-ODI), and the Roland-Morris disability questionnaire (RMDQ).
Results The average symptom duration was 22.6±1.2 weeks in group A, and 35.7±0.9 in group B. Of a total of 20 patients (16.8%), four males (20%) and 16 females (80%) were underwent surgical procedures because there was no improvement in symptoms. Group B had a significantly higher proportion of female patients and longer symptom duration than group A. And there were no statistically significant differences between groups in other variables.
Conclusions Although the frequency of surgical treatment decreased after selective nerve root block, the longer symptom duration and the female gender might be related to the risk factors for surgical treatment.
Objective This study aimed to compare the efficacy of unilateral biportal endoscopic decompression (UBE) and percutaneous endoscopic lumbar discectomy (PELD) in reducing muscle injury by measuring serum levels of creatine phosphokinase (CK) and lactate dehydrogenase (LDH).
Materials and Methods Thirty patients with degenerative lumbar stenosis or a herniated lumbar disc underwent decompression surgery. Among them, 12 patients underwent UBE (experimental group, n=12) and 18 underwent PELD (control group, n=18). CK and LDH were determined at admission and 1, 3, and 5 days after surgery. Pain was measured with a visual analogue scale (VAS).
Results The mean age was significantly higher in the UBE group than the PELD group (63.33±13.50 vs. 49.94±14.79, p<0.035). Mean CK levels were not significantly different at admission. However, at both 3 and 5 days after surgery, CK levels were higher in the UBE group (308.44±153.93 vs. 70.43±40.15, p=0.002; 157.11±91.41 vs. 47.62±23.13, p=0.007). The mean LDH level was higher in the PELD group at 1 day after surgery (152.55±34.69 vs. 199.87±53.78, p=0.027). The operation time was significantly shorter in the PELD group (90.67±39.59 vs. 49.43±14.11, p=0.003).
Conclusions The UBE group had higher CK levels at 3 and 5 days after surgery. The PELD group had a higher LDH level at 1 day after surgery. Therefore, neither procedure is clearly superior in terms of muscle damage.
Background S2-alar-iliac (S2AI) screws are one of the options for spinopelvic fixation to improve stability across the lumbosacral junction. The S2AI screws cross the cortical surfaces of the sacroiliac joint, which can increase the biomechanical strength of the instrumentation.
Objective: To investigate the durability and failure types of S2AI screw by finite element model (FEM) analysis.
Methods Through the FEM, complex material and geometrical properties of the biological system can be evaluated, and various physical variables, such as stress, and fracture, can be analyzed. We examined the biomechanical stress distribution at the set screw and screw head by using a FEM. Von Mises (V.M.) stress (MPa) is derived from 3-dimensional status of stress. The finite element software Abaqus® version 6.5 (ABAQUS Inc., Johnston, RI, USA) was used to create a FEM.
Results We quantified the peak V.M. stress applied to the set screw and screw head when rod to S2AI screw trajectory angle was 30º angled and perpendicular. In FEM analysis, at an angle of 30 degrees rather than perpendicular, the stress increased further around the area where the screw head and rod contacted and the displacement distribution of set screw also increased.
Conclusion S2AI screw fixation has several drawbacks such as screw fracture and dislodgement of the set screw. This FEM analysis can support the result.
Vertebral compression fracture is one of the most common osteoporotic fractures along with hip fractures. In some patients, pain was improved through conservative treatment including pharmaceuticals, bracing and physiotherapy. But it has been reported that conservative therapy is insufficient in many patients with vertebral compression fracture. Accordingly, interest in vertebroplasty has increased and many studies have been reported that vertebroplasty have therapeutic effects in acute vertebral compression fracture. On the other hand, some studies have been reported that the effect of vertebroplasty was not significant. So whether vertebroplasty is useful or not is still controversial. Therefore, in this review article, we will review open-label randomized controlled trials and blinded randomized controlled trials that provide high-level evidence and provide an opinion on which patients it is appropriate to perform vertebroplasty.
Spinal subdural hematoma (SDH) is a rare complication after spinal surgery. Only a few cases are reported on spinal SDH following open lumbar spinal decompression or fusion surgery. Moreover, there has been no case report on spinal SDH following percutaneous transforaminal endoscopic lumbar discectomy. We report a case of spinal SDH following endoscopic discectomy, review the literature of this complication and discuss the etiology to it and methods to prevent it. A 63-year-old woman presented with severe radiating pain. Pain was not improved with conservative management. Lumbar magnetic resonance imaging (MRI) was checked and revealed right L3-4 ruptured disc with severe L4 root compression. Percutaneous transforaminal endoscopic decompression was performed and the pain subsided promptly after the endoscopic procedure. On 7th post-operative day, pain on Rt. buttock, anterior thigh was deteriorated severely, more than in pre-operatively. Deteriorated pain was not controlled by oral medications and epidural block. Repeat MRI showed no definite recurrence of disc herniation at decompressed level but spinal SDH, severely compressing cauda equina was seen on T12-sacral area. Spinal SDH is a rare complication following spine surgery, including percutaneous endoscopic surgery. A spine surgeon should be aware of the possibility of spinal subdural hematoma, having severe sequel.
Background Proximal junctional kyphosis (PJK) following long instrumented fusion is a well-recognized complication that does not negatively affect the clinical outcomes. However, there were few studies with regard to the long-term consequences of PJK.
Objective: To investigate the long-term clinical and radiographic consequences of proximal junctional kyphosis (PJK) following the long instrumented fusion for elderly patients with sagittal imbalance.
Methods Patients older than 60 years who underwent ≥4 fusion including the sacrum for sagittal imbalance were followed up longer than five years. PJK was defined as proximal junctional angle (PJA) >10° without any bony compromise or myelopathy. The radiographic and clinical outcomes were compared between PJK and non-PJK groups. Clinical outcome measures included visual analog scale (VAS) for back and leg, Oswestry disability index (ODI), and Scoliosis Research Society (SRS)-22 scores.
Results A mean age was 69.2 years. An average follow-up duration was 92.4 months. There were 30 patients in PJK group and 43 in non-PJK group. At the final follow-up, pelvic incidence-lumbar lordosis mismatch, pelvic tilt, and sacral vertical axis were not different between the two groups. In PJK group, PJA significantly increased from 6.5° postoperatively to 21.2° at the final follow-up. At the final follow-up, clinical outcomes were worse in PJK group than in non-PJK group with regard to VAS for back, ODI, and SRS-22 scores except satisfaction domain. Three (10%) of 30 patients underwent a revision surgery for PJK progression.
Conclusions PJK progressed with time and negatively affect the clinical outcomes in a long-term follow-up after ASD surgery.
Numerous improvements in minimally invasive spine surgery (MISS) have been made during the past decade.
Classic treatment methods have reserved surgical intervention for trauma patients with neurological compromises or instability. When used in thoracolumbar spine trauma management, MISS should achieve the similar results as classic treatment with less morbidity.(1) In the past decade, minimally invasive surgical (MIS) techniques for spine surgery have been increasingly used. The goal of minimally invasive surgery is to decrease surgical morbidity through decreased soft-tissue dissection providing similar structural stability as classic techniques. An increasing number of studies is reporting good clinical and radiographic outcomes with MIS techniques. However, the literature is lacking high-quality evidence comparing these newer techniques to classic treatments. In the future, development of techniques can expand the indications and treatment possibilities in spine trauma treatment. We reviewed the current literatures to clarify the indications of minimally invasive techniques with spinal trauma.
Objectives to report a surgical site infection from Aspergillus after a lumbar discectomy.
Aspergillus is ubiquitous fungus. People with normal immunity are usually not infected by it, however, surgical site infection from it often developed even in normal population.
Materials and Methods The diagnostic and therapeutic experience of 55-year-old male patient who underwent L45 discectomy who had surgical site infection from Aspergillus was reviewed.
Results He had 4 times surgical treatment and empirical antibiotic therapy due to progressive extension of infection without microbiologic confirmation. Aspergillus flavus was identified at 5th operation and he was cured by adding an anti-fungal agent.
Conclusions An Aspergillus infection after an operation can be developed even in normal immunity population.
If a surgical site infection patient without fever and draining sinus does not improve by conventional treatment, Aspergillus infection should be considered.
Introduction We describe the complications that can occur after percutaneous vertebroplasty using bone cement for osteoporosis vertebral compression fracture.
Main subject: The most common complication of percutaneous vertebroplasty is the leakage of bone cement.
Leakage of bone cement has been reported variously and could leak into the spinal or neural foramen, adjacent intervertebral disc and soft tissues around the spine, and venous systems. The most serious complications are neurologic symptoms due to spinal cord and nerve root compression and complications associated with death due to heart and pulmonary embolism. In addition, recompression fracture or adjacent vertebral compression fracture might occur and various treatment methods have been proposed.
Conclusion The complications that can occur after percutaneous vertebroplasty have been reported variously, including neurologic deficits due to the leakage of bone cement and lung and heart embolism. In addition, there is a possibility of recompression fracture or adjacent compression fracture. Therefore, you should be careful about percutaneous vertebroplasty. Finally, patients with many risk factors regarding complications of vertebroplasty would need close observation and follow-up.
Cervical ossification of posterior longitudinal ligament (OPLL) can cause cord compression which can lead to myelopathy. Operative management including anterior fusion or laminoplasty is needed in these cases.
Understanding the progression course of OPLL, risk factors of progression, and risk factors of myelopathy caused by OPLL is essential to determine the necessity, timing and method of operation. Therefore, we will review the previous study results regarding characteristics and progression course of OPLL. Furthermore, the results of study about risk factors and progression course of OPLL undergoing conservative management will be discussed.
When conservative treatment fails in the treatment of osteoporotic vertebral compression fractures, a minimally invasive procedure, such as percutaneous balloon kyphoplasty or vertebroplasty is performed. Among these, balloon kyphoplasty is known as an advantageous method for lower risk of cement leakage and greater correction effect of kyphosis and better sagittal balance correction. However, there are reports of various complications during and after procedure, and sometimes result in serious consequences. This paper reviews with previous literatures about the complications related to balloon kyphoplasty.
Objectives The primary surgical goals when treating a spinal metastasis are usually pain relief and preservation of ambulatory function. Minimally invasive techniques have become popular, being associated with less morbidity and mortality than conventional open surgeries.
Materials and Methods Between April 2012 and September 2016, 15 consecutive patients underwent percutaneous pedicle screw fixation (PPSF) to treat spinal metastases. We retrospectively analyzed prospectively collected data, including visual analog scale (VAS) pain scores, Frankel scale scores, and complications.
Results Fifteen patients (8 males, 7 females; mean age 61 years) underwent surgery under general anesthesia. PPSF was performed on all patients, and two with poor bone quality underwent cement augmentation of the manipulated vertebra(e) just prior to pedicle screw insertion. Seven patients underwent fixation plus distraction (indirect decompression via ligamentotaxis) and two laminectomies (direct decompression) of the spinal cord. Two patients developed screw pullout requiring revision surgery. One patient died 7 days after surgery from liver cirrhosis and sepsis. All patients reported that pain was reduced after surgery. After surgery, 12 patients regained ambulatory capacity. Nine patients died during follow-up; the mean overall survival time was 14.1 months.
Conclusions PPSF is a safe and minimally invasive palliative surgery option for patients with spinal metastases.
Purpose To evaluate and analyze the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor between recurrence and non-recurrence group, and to assess the merits of minimally invasive spinal surgery.
Overview of Literature: No large registry study has so far investigated the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor.
Methods From July 2003 to April 2011 we retrospectively studied a consecutive series of 156 patients who underwent lumbar microdiscectomy using minimally invasive tubular retractor. The following data were collected: clinical outcomes, operative time, intraoperative blood loss, recurrence, and complications. The clinical outcomes were measured using a visual analog scale (VAS) and assessed by the modified MacNab criteria.
Results Minimally invasive tubular microdiscectomy was performed in 156 patients. The clinical outcomes assessed by MacNab criteria were excellent in 63 patients (40%), good in 71 patients (45%). VAS scores of low-back pain decreased from a mean of 6.7 prior to surgery to 2.5 after surgery, and that of leg pain decreased from 7.2 to 2.1. The average operative time was 68 minutes (range, 25 to 180 minutes). The average blood loss was 42 mL (range, 0 to 500 mL). None of the patients needed blood replacement. One patient had wound infection problem but there was no dural tear case. Twenty-two patients had recurrence. Average time to recurrence was about 42 months. Seventeen cases recurred at the same level and five cases recurred at the adjacent level. Eleven cases in 22 patients with recurrence were contained disc type and the others were non-contained disc type. Eighteen cases in 22 patients with recurrence were paracentral disc herniation type and the others were far lateral type. Average body mass index (BMI) of recurrence cases was 24.7 (range, 17.5 to 31.3) and that of non-recurrence cases was 24.5 (range, 16.3 to 39.2).
Conclusions Lumbar microdiscectomy using tubular retractor can offer a useful modality for the treatment of lumbar herniated disc with the merits of minimally invasive spinal surgery. Further randomized, prospective investigations are needed to fully evaluate the impact of this technique.
Interspinous process devices for spinal surgery are designed to keep the spine in a flexed position, to achieve indirect decompression of the mobile segment. Such devices have been fabricated using numerous materials and designs. In this study, the fundamental knowledge required for choosing an appropriate interspinous process device for spinal surgery was reviewed.
Objectives To verify the hypothesis that nerve compression by postoperative spinal epidural hematoma (POSEH) can be reduced by instillation of heparin through suction drains.
Materials and Methods The patients who underwent posterior decompression and instrumentation between Jan. 2016 and Jun 2016 were allocated to study (using heparin) group and control group according to the operation date alternately. There were 61 cases in study group and 60 cases in control group. Two lines of suction drain were used in all cases. Thousand unit of heparin and 5ml of normal saline were instilled through the drain lines into the epidural space just before the wound closure. To prove the homogeneity between the two groups, demographic, patient related, operation related and clotting related data were compared. At day 7 after the operation, their MRIs were examined. The area of thecal sac was measured at the T2 weighted axial image that showed the maximal compression of the thecal sac by epidural hematoma. Two orthopedic doctors who were blinded to this study measured independently and the average values of the two were counted as final measured values.
Results The two groups were homogenous in age, sex, number of fusion segments, whether virgin or revision operation, total blood loss, operation time, blood loss/10 min, whether taking anti-platelet drugs or not, platelet count, PT, aPTT and platelet function analysis. The smallest area of thecal sac in axial MRI was 124.4±49.9 mm2 in study group and 121.7±47.4 mm2 in control group. There was no significant difference (p=0.761)
Conclusions In a posterior spine surgery, thecal sac compression by POSEH was not reduced by instillation of heparin into the epidural space.
Objectives We report the new minimally invasive technique and its clinical results of oblique lumbar interbody fusion (OLIF) combined with central decompression using biportal endoscopic spinal surgery (BESS).
Summary of Literature Review: The OLIF procedure is one of the minimally invasive spine surgeries and is being frequently attempted recently to treat lumbar degenerative disease. It has been reported that it effectively decompresses foraminal stenotic lesions indirectly by inserting a large cage anteriorly, which reduces spondylolisthesis and widens the disc space. However, OLIF has limited effect for severe central canal stenosis, since it cannot achieve direct decompression. Therefore, authors report a new minimally invasive technique of OLIF combined with direct central decompression using BESS for severe central stenosis along with its clinical results as a pilot study.
Materials and Methods For patients who were candidate for fusion surgery due to spondylolisthesis (more than one segment) or foraminal stenosis, authors performed OLIF and central decompression using BESS simultaneously, when the patients had concomitant severe central canal stenosis. From June to December, 2017, 8 patients (16 levels) were enrolled, the operative time, blood loss, complications and clinical results have been evaluated. The clinical results were analyzed by Visual analog scale (VAS) scores, Oswestry disability index (ODI) and Roland Morris Disability Questionnaire (RMDQ) of preoperative, 1month, 3month postoperative and final follow-up.
Results Mean operative time and blood loss were 238.4 minutes and 173.3ml, respectively. In all cases, there were no operative complications, and mean follow-up period was 7.1 months. The mean back VAS, lower extremity VAS, ODI, and RMDQ at the final follow-up were improved from 5.4±2.4 to 2.0±0.9, 7.0±1.1 to 1.6±1.7, 64.2±11.8 to 44.2±10.6, and from 17.5±4.2 to 12.9±4.0.
Conclusion A new combination technique of OLIF and BESS for direct decompression can be regarded as effective alternative procedure to treat the foraminal and central stenotic lesions of lumbar degenerative disease.
A 77-year-old female suffering from severe degenerative scoliosis, spinal stenosis and lumbar disc herniation underwent Direct lateral lumbar interbody fusion (DLIF) at L2-4. On the 3rd postoperative day, she complained of severe back pain without any trauma history. Simple radiograph revealed L3 vertebral fracture and cage subsidence.
Pain was subsided after conservative treatment including TLSO and medication. Radiographic union was achieved at fractured vertebra after 3 months. Solid fusion was observed at operated level after 6 months. Patient has visited our clinic without any pain. DLIF is one of novel minimally invasive spine procedures available today. It is designed to maximize benefits and minimize risks of other traditional techniques such as anterior approach and posterior approach. However, there can be some risk of cage subsidence and vertebral fracture after DLIF. Therefore, care should be taken to avoid cage subsidence during the operation.
Purpose To evaluate the difference of clinical and radiologic outcomes between Luschka’s joint preservation vs. total uncinatectomy in anterior cervical microforaminotomy.
Materials and Methods From Dec. 2006 to Feb. 2012, 37 patients suffered unilateral cervical radiculopathy due to cervical foraminal disc herniation or spondylotic cervical stenosis underwent anterior cervical microforaminotomy in our hospital. The mean age of patients was 52.9 (range 35 to 72). 27 were men and 10 were women. 19 patients received total uncinatectomy and the other 18 patients received partial uncinatectomy. There was no difference in statistical significance for demographic factors between two groups. Clinical outcomes have been evaluated based on preoperative and postoperative VAS scores for axial pain and radicular pain described on medical records and classified according to modified Odom’s criteria. Postoperative radiologic evaluation was performed through follow
up CT, MRI and plain films. Through this serial studies, postoperative degenerative change was evaluated.
Results Mean follow up period was 44.6 months (from 12 month to 86 months). 6 of 19 patients from total uncinatectomy group suffered chronic postoperative axial neck pain lasting over 3 months after the surgery. In contrast, only 2 of 18 patients in the partial uncinatectomy group complained chronic neck pain. One patient of the partial uncinatectomy group underwent revision surgery due to incomplete decompression. The revision surgical modality was ACDF. Surgical result was classified according to modified Odom’s criteria. But, there was no statistical
differences between outcomes of two groups. During the follow up period, degenerative change was observed in 10 of 19 patients in total uncinatectomy group and 7 of 18 patients in partial uncinatectomy group. But, there was no statistical differences, either (by Kaplan-Meier).
Conclusions Anterior cervical microforaminotomy for unilateral cervical radiculopathy showed favorable results regardless of pathologic lesions, such as disc herniation or stenosis. Total uncinatectomy group seems to cause postoperative chronic axial neck pain, but there was no statistical significance. Anterior cervical microforaminotomy causes early degenerative changes of involved segment. There was no difference in development of degenerative changes between total uncinatectomy group and partial uncinatectomy group
Purpose The purpose of this review is the current understanding of proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) following adult spinal deformity (ASD) surgery.
Materials and Methods We carried out a systematic search of PubMed for literatures published up to September 2016 with “proximal junctional kyphosis” and “proximal junctional failure” as search terms. A total of 57 literatures were searched.
Finally, the 33 articles were included in this review.
Result PJK and PJF are recognized complications after long instrumented posterior fusion in ASD surgery. PJK is multifactorial in origin and likely results from surgical, radiographic, and patient related risk factors. PJF is a progressive form of the PJK spectrum including bony fracture of uppermost instrumented vertebra (UIV) or UIV+1, subluxation between UIV and UIV+1, failure of fixation, neurological deficit, which may require revision surgery for proximal extension of fusion.
Variable risk factors for PJK and PJF have been investigated, and they can be categorized into surgical, radiographic, and patient-related factors. There are several strategies to minimize PJK and PJF. Soft tissue protections, adequate selection of the UIV, prophylactic rib fixation, hybrid instrumentation such as hooks, vertebral cement augmentation at UIV and UIV+1, and age-appropriate spinopelvic alignment goals are worth consideration.
Conclusion The ability to perform aggressive global realignment of spinal deformities has also led to the discovery of new complications such as PJK and PJF. Continuous research on PJK and PJF should be proceeded in order to comprehend the pathophysiology of these complications.
Objective The aim of this study was to analyze significant motion predictors in patients with discogenic and facetogenic back pain confirmed by diagnostic injections and to see confounders which influence motion predictors.
Methods Medial branch block and epidural steroid injection were used for facetogenic and discogenic midline pain.
Transforaminal epidural steroid injection was selected for discogenic lateralized back pain. Positive response was defined as over 75% pain relief. Sixty-four patients (facetogenic pain, 45 bilateral or 9 unilateral, 82% pain relief ), Sixty-three patients (discogenic midline pain, 83%), and twenty-three patients (discogenic lateralized pain, 85%) had been enrolled prospectively in one institution between June 2010 and October 2013. Motion provocation tests were conducted during standing, sitting, flexion, extension, lateral bending, rotation, and extension with rotation for the detection of motion predictors. A self-weighted grade system was applied for pain provocation. Confounders such as age, sex, facet joint degeneration, flexion pain, grade of protrusion, circumferential annular tear, transverse annular tear, and spino-pelvic parameters were assessed to find the influence on motion predictors.
Results In patients with facetogenic pain, pain provocation was prominent during standing (p=0.006), extension (p=0.052), rotation (p=0.000), and extension with rotation (p=0.000). In those with discogenic midline pain, more pain generated during flexion (p=0.000) and sitting (p=0.044). The difference in spino-pelvic parameters between two pain groups was not observed. The difference between discogenic midline and lateralized pain occurred during flexion (midline, p=0.046) and lateral bending (lateralized, p=0.057). Similarly, flexion (p=0.068) and lateral bending (p=0.067) might be also insignificant but helpful predictors to differentiate discogenic lateralized pain from facetogenic lateralized pain. For facetogenic pain, there were significant confounders as follows; standing (facet capsule enhancement, pelvic incidence), sitting (sex), extension (spino-pelvic parameters), lateral bending (pelvic tilt), rotation (age, sex, arthritis, facet capsule enhancement, pelvic tilt). Extension with rotation showed relatively less changes. For discogenic pain, a lake type circumferential tear generated less flexion pain and more extension pain.
A superior transverse tear influenced sitting, extension, and lateral bending. A protrusion without a transverse tear increase flexion pain. Higher pelvic incidence and pelvic tilt generated more extension and extension with rotation pain. Among motions, sitting was not influenced by most probable confounders.
Conclusion Predictors of facetogenic pain were extension with rotation, rotation, standing, extension, and lateral bending in order of probability. Flexion and sitting may be predictors of discogenic midline pain. Flexion and lateral bending may be predictors favoring discogenic lateralized pain compared with facetogenic pain. However, these motions may be vulnerable to parameters such as age, sex, facet arthritis, facet enhancement, circumferential or transverse tear, and spino-pelvic parameters. Considering the confounders’ effect, predictors were likely to be extension with rotation for facetogenic pain, sitting for discogenic midline pain, flexion and lateral bending for discogenic lateralized pain compared with facetogenic pain. These points should be considered in making a diagnosis during the physical examination in the outpatient clinic.
Purpose To evaluate long term efficacy of percutaneous balloon kyphoplasty for osteoporotic compressive vertebral fracture.
Materials and Methods Percutaneous balloon kyphoplasty was performed to 52 vertebral bodies, for 42 patients with compression fracture from March 2003 to October 2007. During observation, 32 patients (39 vertebral bodies) were followed over 5 years except 8 patients (19.0%) who have expired. Pre operational, post operational and final observational radiologic evaluation (vertebral height, compression ratio, kyphotic angle) and clinic evaluation(VAS score) were checked. And correlation with bone cement leakage, fracture of adjacent vertebral body, gender, age, bone mineral density and medication was analyzed.
Result Average age was 71.3 years old and average observation period was 74.3 months. Average interval from injury to operation was 24.1 days. Vertebral compression ratio recovered 29.7% to 17.4% (12.3%), kyphotic angle improved 11.6 degree to 9.0 degree (2.6 degree) and there was no significant change until final observation. VAS score got better 7.60 to 3.57 (4.03) after operation. Bone cement leakage occurred in 5 cases (12.8%) and fracture of adjacent vertebral body occurred in 10 cases (25.6%), there was no correlation between two groups (p=1.000). Fracture of adjacent vertebral body showed meaningful correlation with bone mineral density only.
Conclusion Percutaneous balloon kyphoplasty relieve the pain after compression fracture of vertebral body and is safe and efficient procedure to correct sagittal deformity. After 5 year follow up, the effect of procedure was maintained clinically. Bone cement leakage did not increase risk of fracture of adjacent vertebral body which occurred frequently in low bone mineral density.
Percutaneous vertebroplasty and balloon kyphoplasty are both safe and effective procedures in case of patients with osteoporotic vertebral compression fractures. The authors have already reported a new technique called lordoplasty using polymethylmethacrylate to manage vertebral osteoporotic compression fractures. The purpose and indication of lordoplasty do not differ from that of percutaneous vertebroplasty or balloon kyphoplasty. However, there are advantages of lordoplasty in terms of restoration of the wedge and kyphotic angle and cost-effectiveness compared with the other procedures mentioned above. For the advantages of lordoplasty, authors thereby introduce the detailed procedure of lordoplasty.
Thirty-four-year old female patient visited our clinic for posterior neck pain for 3 days. She had no medical history or traumatic injury. On physical examination, posterior neck pain aggravating with neck motion was seen, there was no neurologic symptom. WBC, ESR and CRP were slightly increased. There was no specific finding on simple cervical radiologic study but, on cervical CT, calcified lesion was seen on the right lateral side of dens.
The symptom got better after medication with NSAIDs, oral and intra venous steroid drugs for 2 days, disappeared after 4 days with NSAIDs and intra venous steroid drug. In following lab study, inflammatory marker decreased.
Crowned Dens Syndrome could be misdiagnosed with meningitis, so cervical CT study is essential for differential diagnosis. Symptoms can be treated with NSAIDs and steroid drug.
Purpose Osteoporosis is an age-related systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone contents, with a consequent increase in bone fragility. In severe osteoporosis progressive collapse of multiple vertebrae is and unsolved problem. Medical treatment appears to be too slow to prevent the course. Recently, there are some reports on the results of the percutaneous vertebroplasty (VP) in treating the multi-level osteoporotic vertebral compression fractures (VCFs). we reviewed painful multi-level osteoporotic VCFs treated by percutaneous VP and assess the efficacy and safety of multiple percutaneous cement VP in the treatment of multi-level osteoporotic VCFs.
Materials and Methods From January 2008 to August 2010, the clinical cases and radiographic records were reviewed retrospectively for 28 patients treated for the multi-level painful osteoporotic VCFs by percutaneous cement VP.
Initially radiography and MRI of the spine were performed. Spine radiographs were repeated at post-operation, 1,3 months and final follow-up. The patient’s outcomes of demographic, clinical, radiologic and procedural data were analyzed and assessed using self-report and physiological measures. A t-test was used for means of VAS, anterior vertebral height and kyphotic angle. Statistical analysis was performed with the SPSS(Version 15.0.1, Chicago, Illinois). The p-values of < 0.001 were deemed significant.
Results The back pain recorded using the VAS improved significantly in all cases, from 7.7±1.0(6-10), points preoperatively to 2.0±0.7(1-3) points postoperatively (p<0.001) and then 2.8±0.8(1-4) points at the follow-up (p<0.001).
The anterior heights increased from 17.40±4.98 to 21.02±5.36 after VP procedures (p<0.001) and finally 19.49±5.28 (p<0.001). The kyphotic angle was 12.58º preoperatively and improved to 4.39º postoperatively, but kyphotic deformities became worse in 12.80º.
Conclusion The vertebroplasty for patients with multiple osteoporotic vertebral compression fractures may improve pain and can be effective for preventing adjacent fractures, restoration of vertebral height and maintenance of sagittal alignment. Patients with multiple osteoporotic compression fractures have many comorbidity, the surgeon should be conscious to all procedure.
Purpose Pull-out of pedicle screw in posterior pedicle fixation for thoracic and lumbar burst fractures causes delayed rehabilitation, persistant pain, and imblance of sagittal plane. In this study we try to analyse the factors that cause the pull-out of pedicle screw.
Materials and Methods From March 01, 2006 to December 31, 2009, we assorted into two group; Group I for pullout pedicle, Group II for control. Plane lateral x-ray view film of thoracolumbar spine was taken on preoperation, postoperation, the first time when screw was pulled out and last follow up. we measure inserted angle for the upper endplate of screw, convergency angle and change of body height loss and kyphotic angle. We analysed corelation between these measuring values and pedicle screw pull-out by Mann-Whitney test and T-test.
Results Pull-out of pedicle screw was found at mean 5weeks among nine cases. For inserted pedicle screws, which place in upper and lower vertebral body of fractured one, Value of inserted angle for upper end plate and convergency angle was found non-significant(p>0.05, Mann-Whitney test). Restoration of height loss and kyphotic angle of fractured vertebral body was statically significant(p<0.05, T-test).
Conclusion In posterior pedicle fixation for thoracic and lumbar burst fractures, sufficient restoration of height loss and kyphotic angle is important factor for prevention of screw pull-out than inserted angle for upper end plate and convergency angle at a short period of time. Therefore we think that sufficient anterior fixation of vertebral body and restoration of kyphotic angle have a decisive effect on prognosis of patients.
Purpose To evaluate the method of inserting cortical bone trajectory pedicle screws (cortical screws) and potential complications when performing lumbar fusion.
Methods Lumbar fusion with cortical screw fixation in the hard cortical bone of the pars interarticularis of vertebrae was introduced to replace conventional pedicle screws. We review the literature on the biomechanics of cortical screw insertion and on the clinical outcomes.
Results In vitro biomechanical testing has shown that cortical screws have greater pullout strength than traditional pedicle screws due to the strong bone–screw interface in cortical bone. Cortical screws have the advantages of requiring minimal muscle dissection and shortening the surgery. However, early screw loosening and loss of reduction have been reported.
Conclusions When inserting cortical screws, the entry point and trajectory of the screws are important and a meticulous surgical technique is needed to prevent potential screw-related complications.
Although metastatic lung adenocarcinoma in the spinal cord is rare, it can be diagnosed by positron emission tomography and computed tomography (PET/CT) scan with high sensitivity during the early disease stage. A clinical and radiographic review was performed to present a rare case of an intradural intramedullary adenocarcinoma metastasis in the spinal cord with a negative PET/CT scan. A 75-year-old man with a diagnosis of lung cancer without metastasis confirmed by a negative PET/CT scan with no spinal symtoms (conducted 6 weeks previously) presented with progressive paralysis of both lower extremities and accompanying bowel and bladder symptoms. He underwent radical lobectomy of left lung under diagnosis of lung cancer without distant metastasis 6 weeks ago. Emergent MRI was performed, and MRI revealed a large intradural intramedullary mass compressing the spinal cord and extending from T12 to L1 with anterior compression of the spinal cord. Surgical decompression and tumor resection from T12 to L1 by lumbar laminectomy and durotomy were performed under a microscope. And, a diagnosis of adenocarcinoma to the spinal cord was made based on histopathologic findings. Postoperatively, the patient’s neurologic status was not significantly improved. Despite a negative PET/CT scan finding with no neurologic symptoms or pain, surgeons should not exclude the possibility of a spinal metastatic lesion with lung cancer.

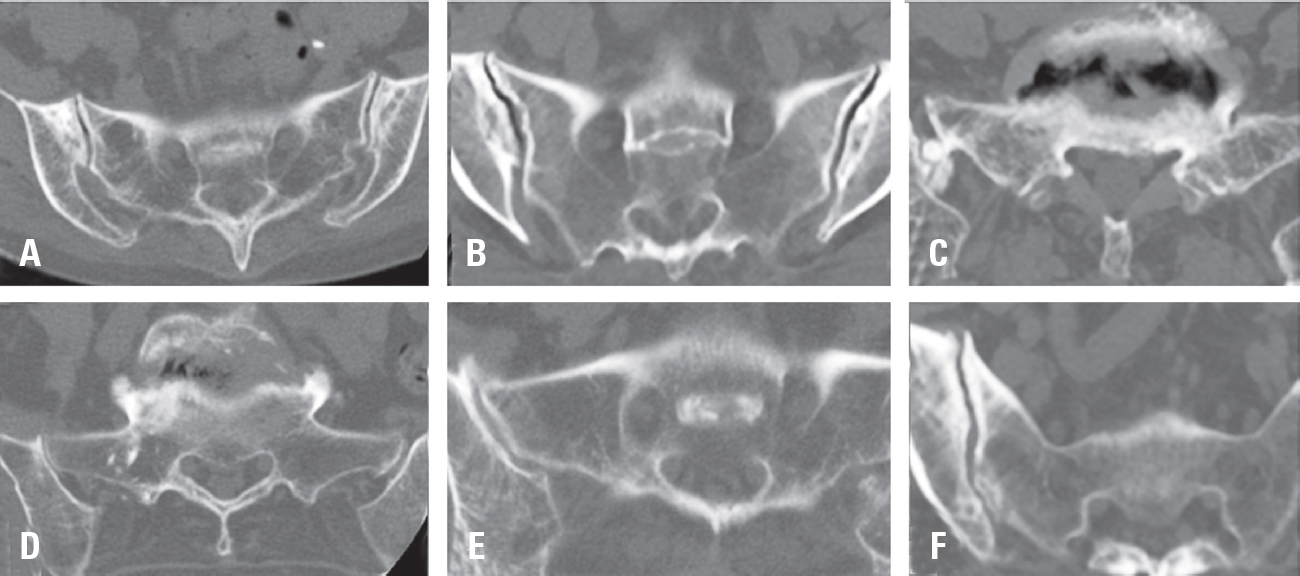
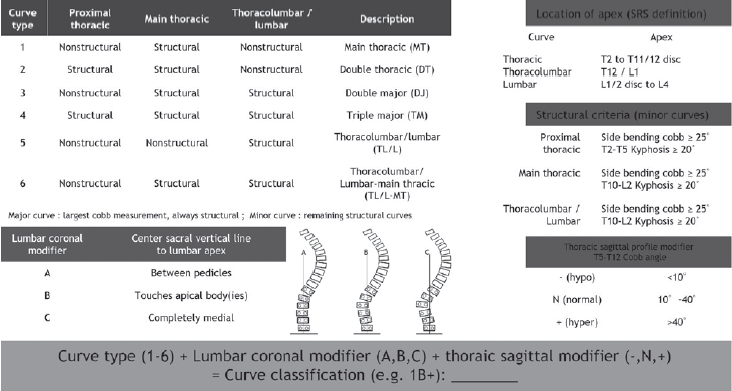
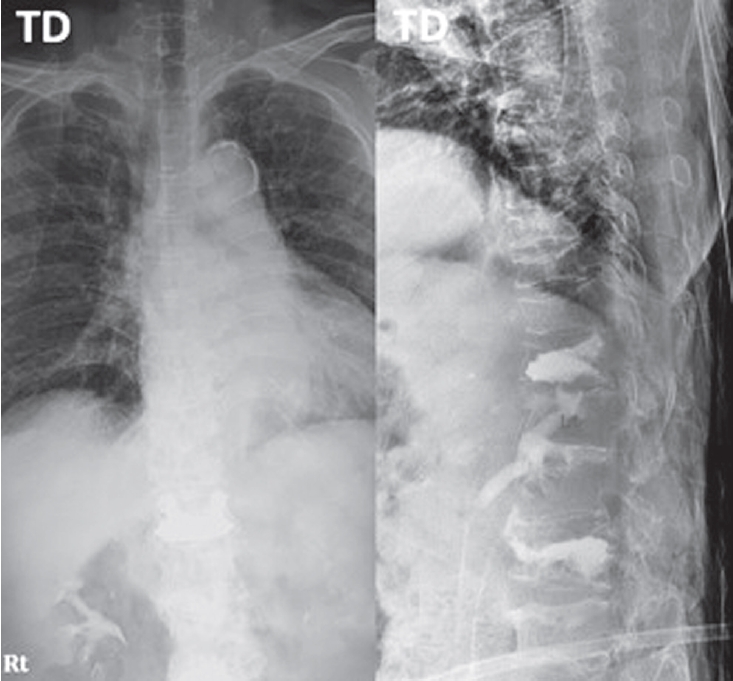
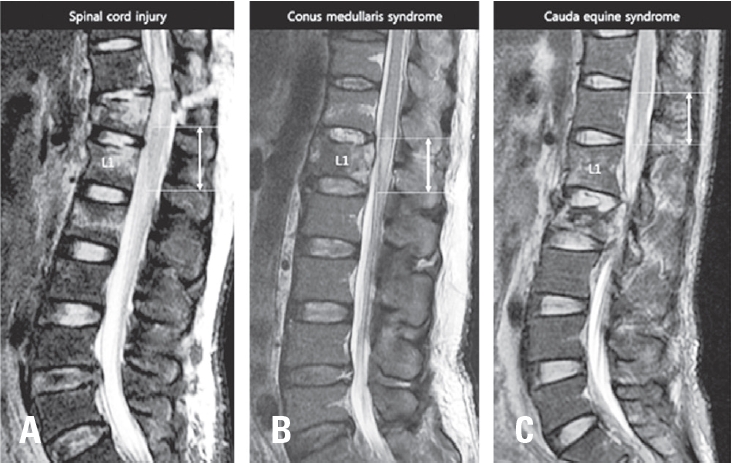
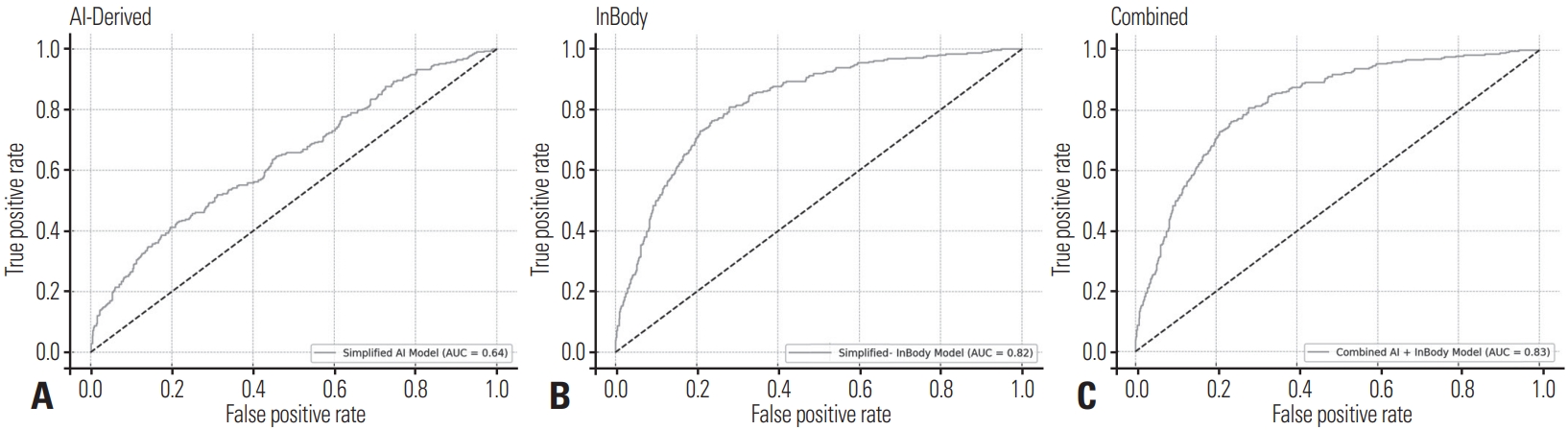
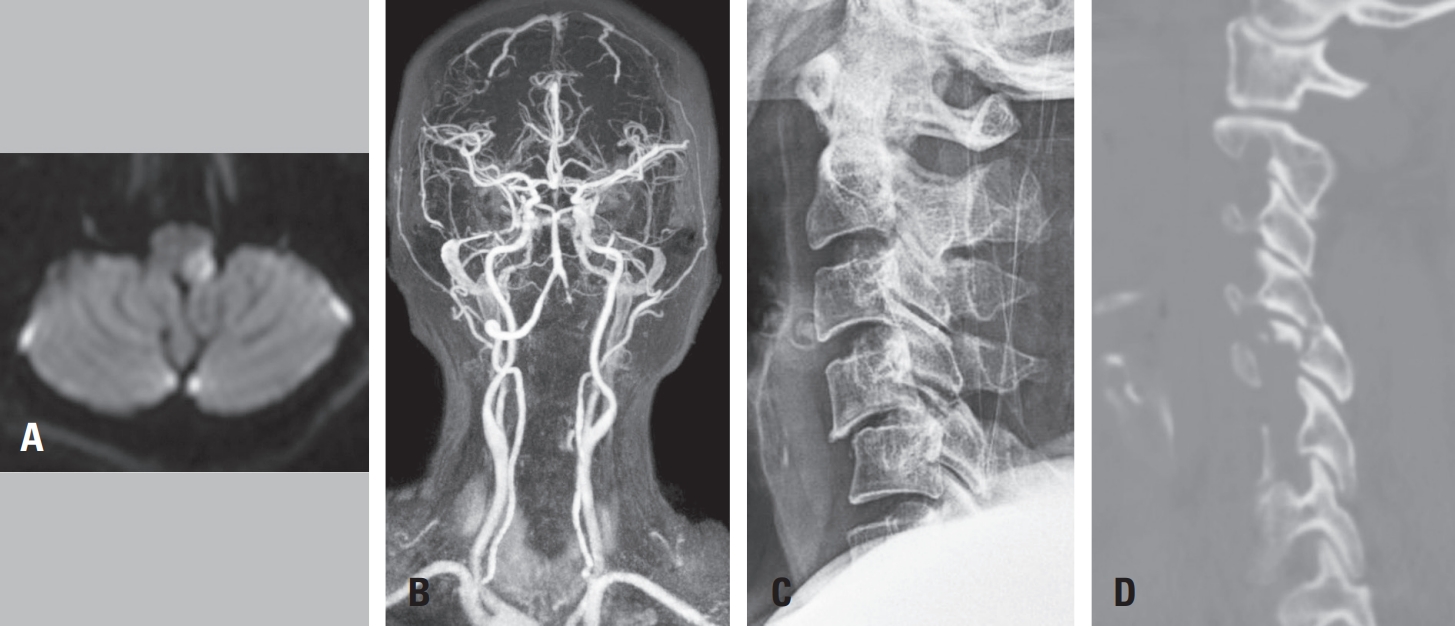
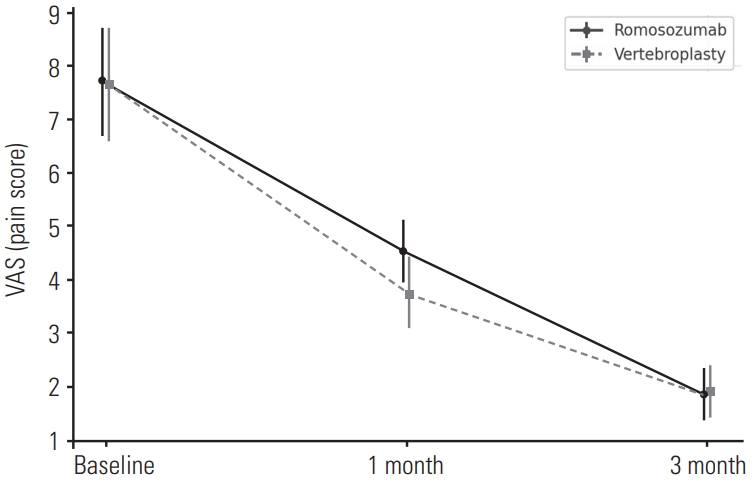
 First
First Prev
Prev

