Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Background Endoscopic spinal surgery for lumbar foraminal lesions comes to be more popular recently. Bleedings around the foramen during extraforaminal endoscopic approach could make surgical filed turbid and more difficult to perform procedures safely. There were, however, few reports and insufficient information about vascular geometry around the foramen.
Purpose To report lumbar foraminal vascular geometry to help endoscopic spinal surgery underwent well and decrease technical complications by control of bleeding.
Materials and Methods We reviewed operating record movie clips of extraforaminal approach using biportal endoscopic spine surgery (BESS). Several bleeding foci were matched with previously reported vascular anatomy and vascular geometry was modified to adapt to endoscopic view.
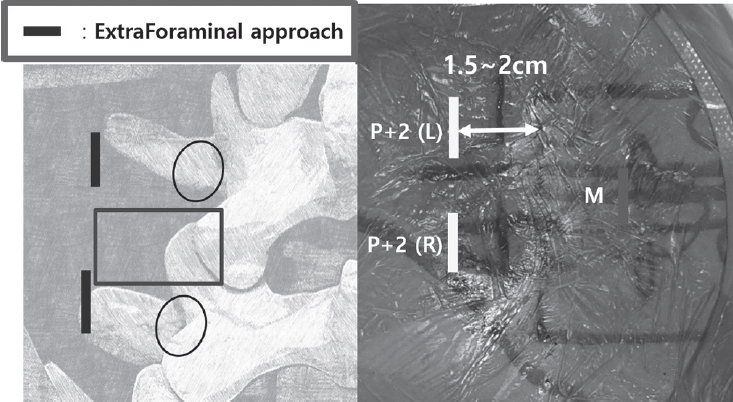
Results There were four main arterial branches coming out from the lumbar segmental artery. Inferior articular artery, superior articular artery, inter-articular artery and radicular artery could be faced in order during extraforaminal approach using BESS. To escape heavy bleeding from the inferior articular artery and superior articular artery, the dorso-distal surface of transverse process (TP) should be exposed to make a working space without scratching the proximal area of the TP and dorsal surface of the facet. Inter-articular artery was hidden and covered under the capsule overlying superior articular process. Radicular artery was running along the midline of the root under the foraminal ligamentum flavum.
Conclusion The information of the geometric location of the four arterial branches could help to escape heavy bleeding on extra-foraminal approach and control the bleeding foci to prevent postoperative hematoma.

 First
First Prev
Prev

