Clinical and Radiological Outcomes of Biportal Endoscopic Revision Extraforaminal Lumbar Interbody Fusion Following Previous Central Decompression: A Case Series
1)Department of Orthopaedic Surgery, Spine Center, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
2)Department of Orthopaedic Surgery, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Corresponding author: Hyun-Jin Park, M.D., Ph.D. Department of Orthopedic Surgery, Spine Center, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, 1, Singil-ro, Yeongdeungpogu, Seoul, 07441 Korea TEL: +82-2-829-5445, FAX: +82-2-849-4469 E-mail: phjfrog@hanmail.net, phjfrog@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods
This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results
Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions
Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
후방 감압술 후 시행되는 요추 재수술은 경막외 유착과 해부학적 구조 변화로 인해 후방 재진입 시 합병증 위험이 증가하여 기술적으로 어렵다. 기존에 수술된 경로를 피하는 수술 접근법은 이러한 위험을 줄일 수 있다. 외측공 접근을 이용한 양방향 내시경 요추체간 유합술은 새로운 수술 경로를 통해 직접적인 신경 감압과 체간 유합을 가능하게 하여 재수술 상황에서 장점이 있을 수 있다. 그러나 재수술에서 이 술기에 대한 임상적 근거는 아직 제한적이다. 본 연구의 목적은 기존에 중심부 감압술을 시행받은 요추 분절에서 시행한 양방향 내시경 재수술 외측공 요추체간 유합술(BE-REFLIF)의 임상적 및 방사선학적 결과를 평가하는 것이다.
대상 및 방법
본 연구는 단일 기관 후향적 증례 연속 연구이다. 2017년 9월부터 2024년 6월까지 기존 중심부 감압술 이후 재수술로 단일 분절 BE-REFLIF를 시행받은 연속된 20명의 환자를 후향적으로 분석하였다. 임상적 결과는 요통 및 하지통에 대한 시각적 통증 척도(Visual Analogue Scale, VAS), Oswestry Disability Index (ODI), EuroQol-5D (EQ-5D)를 이용하여 평가하였다. 방사선학적 결과로는 추간판 높이, 분절 정렬, 요추 전만각, 유합 여부, 케이지 침강을 분석하였다. 또한 수술 전후 자료와 수술 후 합병증도 함께 분석하였다.
결과
추적 관찰 기간 동안 모든 임상적 지표에서 유의한 호전을 보였다. 요통 및 하지통에 대한 평균 VAS 점수와 ODI는 시간 경과에 따라 유의하게 감소하였다(p<0.001). 방사선학적 분석에서는 추간판 높이의 유의한 회복, 분절 정렬의 개선, 요추 전만각의 유지가 확인되었다. 최종 추적 관찰 시 85%의 환자에서 견고한 유합이 확인되었으며, 케이지 침강은 25%에서 발생하였으나 재수술이 필요한 경우는 없었다. 수술 전후 합병증으로는 경막 파열이 10%, 경막외 혈종이 5%, 수술 부위 감염이 5%에서 발생하였으며, 기구 관련 실패는 관찰되지 않았다.
결론
기존 중심부 감압술 이후 재수술로 시행한 양방향 내시경 재수술 외측공 요추체간 유합술은 만족스러운 임상적 및 방사선학적 결과를 보였다. 반흔이 형성된 후방 조직을 피하는 외측공 수술 경로를 활용함으로써, BE-REFLIF는 효과적인 직접 감압과 체간 유합을 허용하며 허용 가능한 합병증 발생률을 보였다. 이 술기는 요추 재유합술이 필요한 일부 선택된 환자에서 유용하고 덜 침습적인 대안이 될 수 있을 것으로 생각된다.
Lumbar spinal stenosis and lumbar disc herniation are common degenerative spinal disorders that often cause dis-abling back pain or radiculopathy. When symptoms persist despite adequate conservative treatment, posterior decompression surgery—such as laminectomy, hemilaminectomy, or discectomy—is considered an effective primary surgical option.1-3) However, postoperative restenosis or recurrent disc herniation may occur as part of the degenerative cascade, and these conditions frequently require reoperation at the previously decompressed segment. Several large cohort studies have reported that the reoperation rate continues to increase over time following initial decompression, reaching 9.5% at 4 years and up to 19% at 11 years postoperatively.4) Revision surgery at the same level poses significant technical challenges. Epidural adhesions and distortion of normal anatomical landmarks increase the risk of complications such as incidental durotomy, neural injury, and excessive bleeding, with revision cases showing substantially higher dural tear rates compared to primary surgeries.5,6) To overcome these challenges, alternative surgical approaches that avoid the previously operated posterior corridor have been explored. Anterior and oblique retroperitoneal approaches—including oblique lumbar interbody fusion (OLIF)—have been reported as safe and effective methods for indirect decompression while avoiding epidural adhesions associated with posterior revision surgery.7,8) However, these anterior-based fusion techniques may have limitations in cases requiring direct neural decompression or when vascular anomalies restrict access to the L5–S1 corridor.9) Biportal endoscopic lumbar interbody fusion using an extraforaminal approach (BE-EFLIF) provides a unique advantage in revision surgery because it enables direct decompression and fusion while entering through a completely new extraforaminal working corridor, thereby avoiding the scarred central canal and epidural adhesions.10-12) By accessing the disc space from a “virgin plane,” BE-EFLIF may reduce the risk of revision-related complications such as incidental durotomy and neural injury. These theoretical advantages are clinically meaningful, but evidence evaluating BE-EFLIF specifically as a revision technique remains limited. Therefore, this study aims to evaluate the clinical and radiologic outcomes of biportal endoscopic extraforaminal TLIF (BEEFLIF) performed at levels previously treated with posterior decompression. We hypothesize that this approach may offer safe and effective decompression and fusion while minimizing revision-related complications.
Methods
1. Study design and patient population
This retrospective case series was conducted at a single tertiary spine center. Consecutive patients who underwent biportal endoscopic extraforaminal transforaminal lumbar interbody fusion (BE-EFLIF) as revision surgery were reviewed. A total of 20 patients were included in the final analysis. All procedures were performed by a single surgeon. Institutional Review Board approval was obtained prior to data collection. This study was approved by the Institutional Review Board of Hallym University Kangnam Sacred Heart Hospital (IRB No. HKS 2025-10-027). The requirement for written informed consent was waived due to the retrospective nature of the study.
2. Inclusion and exclusion criteria
Patients were included if they had (1) a history of prior posterior central decompression at the index level, (2) recurrent or persistent radiculopathy and/or mechanical low back pain refractory to conservative treatment, (3) radiologic evidence of recurrent stenosis, disc degeneration, or instability at the previously decompressed segment, and (4) underwent revision fusion using BE-EFLIF. Patients with high-grade spondylolisthesis, spinal infection, malignancy, trauma, or incomplete follow-up data were excluded. Revision fusion was indicated in patients with recurrent symptoms after previous decompression when re-entry into the prior posterior surgical corridor was considered high risk due to epidural adhesions and distorted anatomy. The extraforaminal biportal endoscopic approach was selected to allow direct neural decompression and interbody fusion through a relatively unviolated surgical corridor.
3. Surgical technique
1) Patient positioning and preparation
All procedures were performed under general anesthesia with the patient positioned prone on a radiolucent Jackson table. After confirming the target level using C-arm fluoroscopy, the operative field was prepared in a standard sterile manner. A 0° or 30°, 4-mm biportal endoscope certified forspinal use was utilized, and standard endoscopic and arthroscopic instruments were prepared.
2) Portal placement
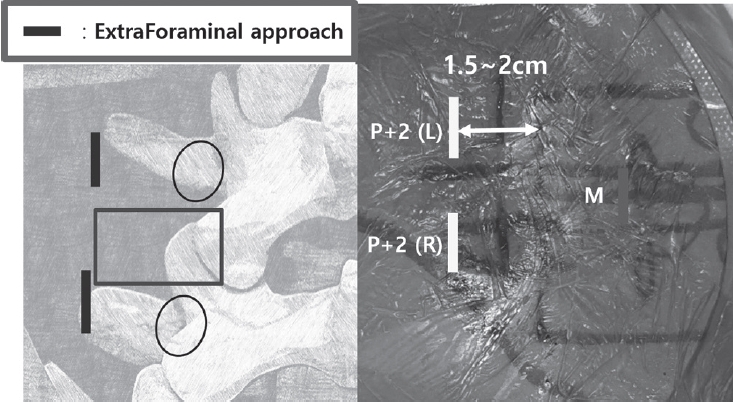
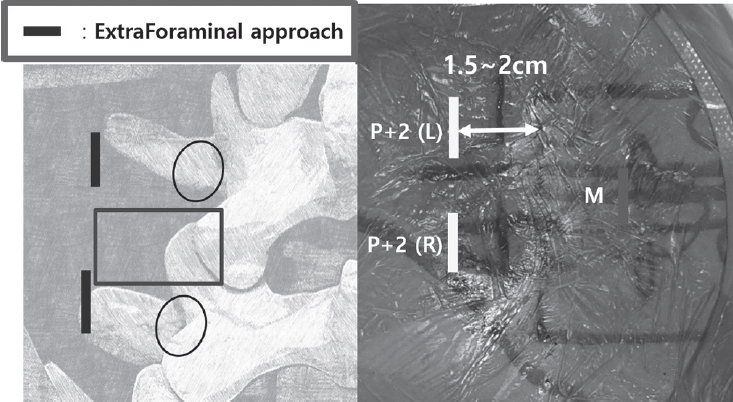
Under anteroposterior fluoroscopic guidance, the pedicles and transverse processes at the target level were marked. Two vertical skin incisions approximately 2 cm lateral to the pedicle line were created to establish the viewing and working portals. At the L5–S1 level, the portals were positioned more cranially to avoid iliac crest interference. When endplate visualization was anticipated, additional medial portals (M portal) were created to accommodate the endoscope or a root retractor during cage insertion (Fig. 1).
3) Facet resection and foraminal decompression
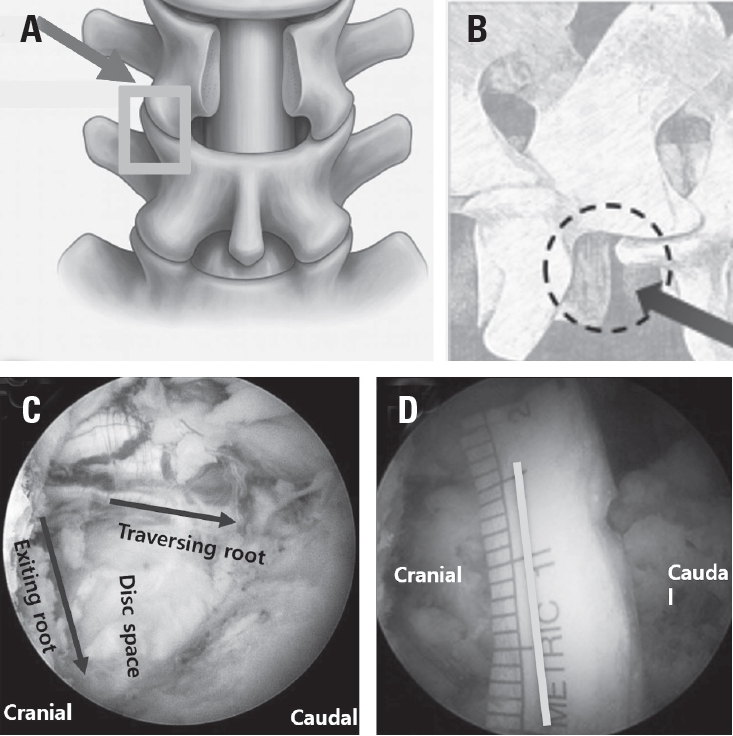
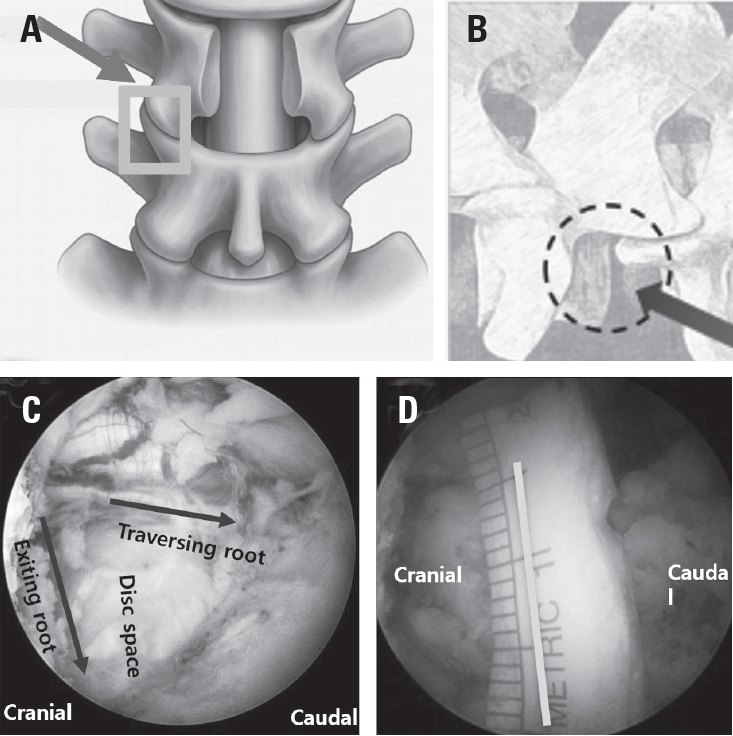
The extraforaminal surgical corridor was developed by exposing the transverse process and advancing medially to the facet joint. The facet capsule was released, and the superior articular process was removed using a high-speed burr and chisel to maximize the acquisition of autologous bone graft. Subsequent flavectomy allowed visualization of Kambin’s triangle. Foraminal decompression was completed by resecting the medial aspect of the transverse process and residual bony structures adjacent to the exiting nerve root, ensuring adequate decompression and a safe working corridor (Fig. 2).
4) Disc space preparation
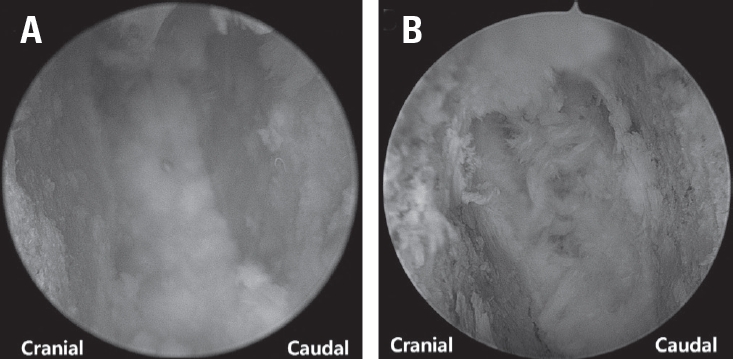
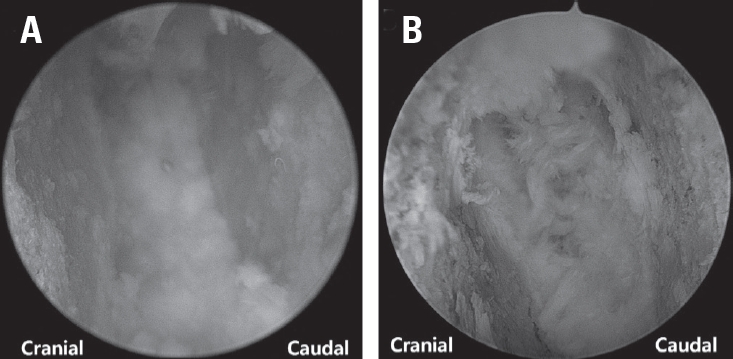
Through the extraforaminal portal and medial portal, annulotomy was performed, followed by disc removal using reamers and pituitary forceps. About 20 mm safety margin lateral to the traversing nerve root was maintained to accommodate a large-footprint cage. Endplate preparation was performed with angled curettes under direct endoscopic visualization, using the medial portals when necessary to inspect the endplate corners (Fig. 3). Sequential trials were used to restore disc height with minimal endplate violation. Bone graft material was introduced into the disc space via a funnel-type delivery device.
5) Cage insertion
A large 3D-printed porous titanium cage was packed with bone graft and inserted through the extraforaminal working portal. Initial advancement occurred along the far lateral entry corridor, followed by medial adjustment using an impactor inserted through the M portal. Final cage positioning was confirmed fluoroscopically, ensuring placement within the anterior one-third of the disc space and symmetric coverage of the apophyseal rings. Hemostasis was achieved endoscopically, and a drain was placed via the M portal.
6) Percutaneous pedicle screw fixation
Percutaneous pedicle screws were inserted bilaterally under fluoroscopic guidance through the previously established lateral portals, with additional incisions made on the contralateral side. Rods were applied and compressed to optimize segmental lordosis before final tightening (Fig. 4).
7) Clinical outcome assessment
Clinical outcomes were evaluated using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Assessments were performed preoperatively and at 1, 6, and 12 months postoperatively.
8) Radiologic assessment
Standing anteroposterior and lateral radiographs were obtained preoperatively and postoperatively. Disc height, segmental sagittal angle, segmental coronal angle, and lumbar lordosis were measured. Fusion status was assessed based on radiographic fusion grading and classified as fused or non-fused at the final follow-up. Cage subsidence was defined as a decrease in disc height identified on follow-up imaging.
9) Perioperative and laboratory data
Perioperative variables included operative time, estimated blood loss, transfusion requirement, and length of hospital stay. Laboratory parameters—including hemoglobin, creatine phosphokinase (CPK), and C-reactive protein (CRP)—were measured preoperatively and postoperatively to assess surgical invasiveness and inflammatory response.
10) Complications
Surgical complications such as dural tear, epidural hematoma, surgical site infection, incomplete decompression, and transient nerve root injury were recorded throughout the follow-up period.
11) Statistical analysis
Continuous variables were presented as mean±standard deviation, and categorical variables as counts and percentages. Changes in clinical outcomes over time were analyzed using repeated-measures models, and pre- and postoperative radiologic parameters were compared using paired statistical tests. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Results
1. Patient demographics
A total of 20 patients were included in this case series. The mean age was 67.2±11.2 years, with 11 male and 9 female patients. The mean body mass index was 26.1±3.1 kg/m², and the mean bone mineral density T-score was −1.2±1.2. According to the American Society of Anesthesiologists (ASA) classification, 8 patients (40%) were classified as ASA I and 12 patients (60%) as ASA II. The most commonly treated level was L4–5 (60%), followed by L5–S1 (20%), L3–4 (15%), and L2–3 (5%). The mean operative time was 200.8±42.5 minutes, and the mean length of hospital stay was 19.1±4.8 days (Table 1).
2. Clinical Outcomes
Significant improvements were observed in all clinical outcome measures over time.
The mean VAS score for back pain improved from 6.15±2.01 preoperatively to 3.75±1.86 at 1 month, 2.95±1.28 at 6 months, and 2.95±1.32 at 12 months postoperatively. Repeated-measures analysis demonstrated a significant interaction effect (p<0.001). Similarly, the mean VAS score for leg pain decreased from 6.50±2.40 preoperatively to 2.45±1.47 at 1 month, 1.80±1.40 at 6 months, and 1.65±1.53 at 12 months, with a significant interaction effect (p<0.001). Functional outcomes showed marked improvement following surgery. The mean ODI score improved significantly from 31.4±7.6 preoperatively to 21.3±8.63 at 1 month, 13.65±5.58 at 6 months, and 9.8±6.14 at 12 months postoperatively (p<0.001). Healthrelated quality of life, as assessed by the EuroQol-5D (EQ-5D), also demonstrated significant improvement. The mean EQ-5D index increased from −0.18±0.03 preoperatively to 0.18±0.49 at 1 month, 0.73±0.22 at 6 months, and 0.81±0.06 at 12 months postoperatively, with a significant interaction effect over time (p<0.001) (Table2).
Mean disc height increased from 8.4±2.4 mm preoperatively to 12.8±1.5 mm postoperatively, with a mean increase of 4.4±1.9 mm (p<0.001). Segmental sagittal angle improved from 5.7±4.6° to 9.7±4.8°, representing a mean increase of 4.1±4.5° (p<0.001). Segmental coronal angle decreased from 2.5±2.6° to 0.9±0.6°, indicating improved coronal alignment (p=0.014). Overall lumbar lordosis increased significantly from 35.1±12.4° to 40.8±10.7° (p<0.001). Radiographic fusion was achieved in 17 patients (85%) at the final followup. Cage subsidence was observed in 5 patients (25%), none of whom required revision surgery (Table 3).
4. Perioperative and laboratory outcomes
The mean estimated blood loss was 273.9±240.9 mL. Blood transfusion was not required in 87.5% of patients, while 12.5% required a single-unit transfusion. The mean hemoglobin level decreased from 13.0±1.3 g/dL preoperatively to 12.1±1.2 g/dL postoperatively, corresponding to a mean reduction of 6.9±4.1%. Serum creatine phosphokinase (CPK) levels increased from 104.0±50.5 IU/L preoperatively to 573.4±365.4 IU/L on postoperative day 1, and subsequently decreased to near baseline levels at 1 and 2 weeks postoperatively. C-reactive protein (CRP) levels showed a similar transient postoperative elevation, peaking at 79.1±42.8 mg/L on postoperative day 1, followed by gradual normalization (Table 4).
5. Complications
Surgical complications included dural tears in 2 patients (10%), epidural hematoma in 1 patient (5%), and surgical site infection in 1 patient (5%). No cases of incomplete decompression or transient nerve root injury were observed. No patients required reoperation related to instrumentation failure or nonunion during the follow-up period (Table 5).
Discussion
Revision lumbar surgery remains technically demanding because previous decompression alters normal anatomical planes and results in dense epidural adhesions. These changes substantially increase the risk of perioperative complications, particularly incidental durotomy and neural injury. Large cohort studies have consistently demonstrated that reoperation rates after lumbar decompression continue to rise over time, reaching approximately 9.5% at 4 years and up to 19% at more than 10 years postoperatively.4,5) Moreover, revision procedures have been reported to carry a significantly higher risk of dural tears compared with primary surgery, largely due to scarring and loss of natural tissue planes.6,7) To mitigate these risks, alternative surgical strategies that avoid re-entry into the scarred posterior corridor have been increasingly adopted. Anterior and oblique lumbar interbody fusion techniques, such as OLIF, allow access to the disc space through a relatively unviolated retroperitoneal corridor and achieve indirect neural decompression via disc height restoration and ligamentotaxis.8,9,11) Several studies have reported favorable outcomes of OLIF in revision settings, with lower rates of dural injury compared to posterior revision fusion.9,11) However, these approaches have inherent limitations, including restricted applicability in patients requiring direct neural decompression and those with unfavorable vascular anatomy, particularly at the L5–S1 level.9) Biportal endoscopic extraforaminal TLIF (BE-EFLIF) represents a hybrid solution that combines the advantages of a virgin surgical corridor with the ability to perform direct decompression. By accessing the disc space through an extraforaminal route, BE-EFLIF avoids the previously operated central canal and lateral recess, thereby minimizing dissection through scarred epidural tissue. In the present series, this approach resulted in significant improvements in pain, disability, and radiologic parameters, with acceptable fusion rates and a low incidence of major complications. These findings are consistent with prior studies demonstrating the safety and effectiveness of biportal endoscopic spine surgery in both decompression and fusion procedures.10,14-16) The clinical outcomes observed in this study showed marked and sustained improvement in VAS and ODI scores over the 12-month follow-up period. The magnitude of ODI improvement exceeded the minimum clinically important difference (MCID) reported for lumbar fusion surgery, suggesting that the observed functional gains were not only statistically significant but also clinically meaningful.13) Radiologic analysis demonstrated restoration of disc height, improvement in segmental alignment, and maintenance of global lumbar lordosis, supporting the biomechanical adequacy of the extraforaminal interbody construct. From a surgical perspective, the extraforaminal biportal endoscopic approach offers several technical advantages in revision settings. Continuous irrigation, magnified endoscopic visualization, and the use of standardarthroscopic instruments allow precise decompression and meticulous endplate preparation while preserving paraspinal musculature. The use of a large-footprint interbody cage further facilitates load sharing across the apophyseal ring, potentially reducing the risk of subsidence and promoting fusion, as suggested in recent biportal endoscopic fusion studies.10,17) One of the theoretical advantages of the BE-REFLIF technique is the ability to access the disc space through an extraforaminal corridor while avoiding dense epidural scar tissue created by prior posterior decompression. By minimizing dissection within the scarred central canal, this approach is expected to reduce the risk of incidental dural tears during revision surgery. In the present series, dural tears occurred in 2 patients (10%). Although dural injury was not completely avoided, this incidence falls within the range of dural tear rates reported in previous studies of revision lumbar surgery, which have been reported to range from approximately 8% to over 20%.6,7) Importantly, both dural tears in this study were successfully managed using fibrin sealant patches without the need for direct dural suturing or conversion to open surgery. No cerebrospinal fluid– related complications were observed during follow-up. We speculate that preservation of relatively fresh, non-scarred tissue planes in the extraforaminal corridor may facilitate effective sealing of small dural defects, thereby reducing the necessity for formal dural repair.Despite these encouraging results, this study has several limitations. First, its retrospective case series design without a control group limits the ability to draw direct comparisons with other revision strategies such as OLIF or conventional open TLIF. Second, the sample size was relatively small, which may have limited the statistical power to detect less frequent complications. Third, all procedures were performed by a single experienced surgeon at a single institution, which may limit the generalizability of the results. Finally, although early fusion rates were acceptable, longer follow-up is necessary to evaluate long-term fusion durability and adjacent segment degeneration. Nevertheless, this study provides clinically relevant evidence supporting the use of BE-EFLIF as a viable revision option after failed posterior decompression. In patients for whom re-entry into the posterior canal poses substantial risk and anterior approaches are not ideal, biportal endoscopic extraforaminal fusion may represent a reasonable and safe alternative.
Conclusions
Biportal endoscopic extraforaminal transforaminal lumbar interbody fusion (BE-EFLIF) demonstrated favorable clinical and radiologic outcomes in patients requiring revision surgery after prior posterior decompression. By utilizing a relatively unviolated extraforaminal corridor, this technique allowed effective direct neural decompression and interbody fusion while potentially reducing the risks associated with re-entry into scarred posterior tissues. BEEFLIF may represent a reasonable and safe alternative revision strategy for selective indication. Further comparative studies with larger cohorts and longer follow-up are warranted to confirm these findings.
Fig. 1.
Portal placement and fluoroscopic landmarks for biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF).
Surgical incisions for BE-EFLIF using multiportal approach. P+2 ports mean that it is made 2 cm lateral to the pedicle lateral margin, and are used for facetectomy and foraminotomy. Based on when a right-handed surgeon performs a left side approach, the port on the left used as a viewing port is called P+2 (L) port, and the port on the right used as a working port is called P+2 (R) port. Additional M ports are made to perform Root retraction during cage insertion or accomodate the endoscope. BE-EFLIF, biportal endoscopic extraforaminal lumbar interbody fusion
Fig. 2.
Schematic illustration of the extraforaminal working corridor for biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) in a previously decompressed segment. (A) Targeting of the remnant inferior articular process (IAP) and the superior articular process (SAP) to define the bony boundaries of the working corridor. (B) Illustration of the established extraforaminal corridor used for interbody cage insertion. (C) Visualization of the opened disc space between the exiting nerve root and the traversing nerve root after adequate decompression. (D) Measurement of the distance between the traversing and exiting nerve roots, demonstrating a minimum required safety margin of 15 mm to allow safe insertion of the interbody cage.
Fig. 3.
Visualization of endplate preparation during biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF). (A) Endoscopic view obtained through the medial portal demonstrating inspection of adequate endplate preparation prior to cage insertion. (B) Endoscopic view using a 30° scope to evaluate the medial aspect of the endplate, allowing confirmation of complete disc removal and appropriate endplate preparation
Fig. 4.
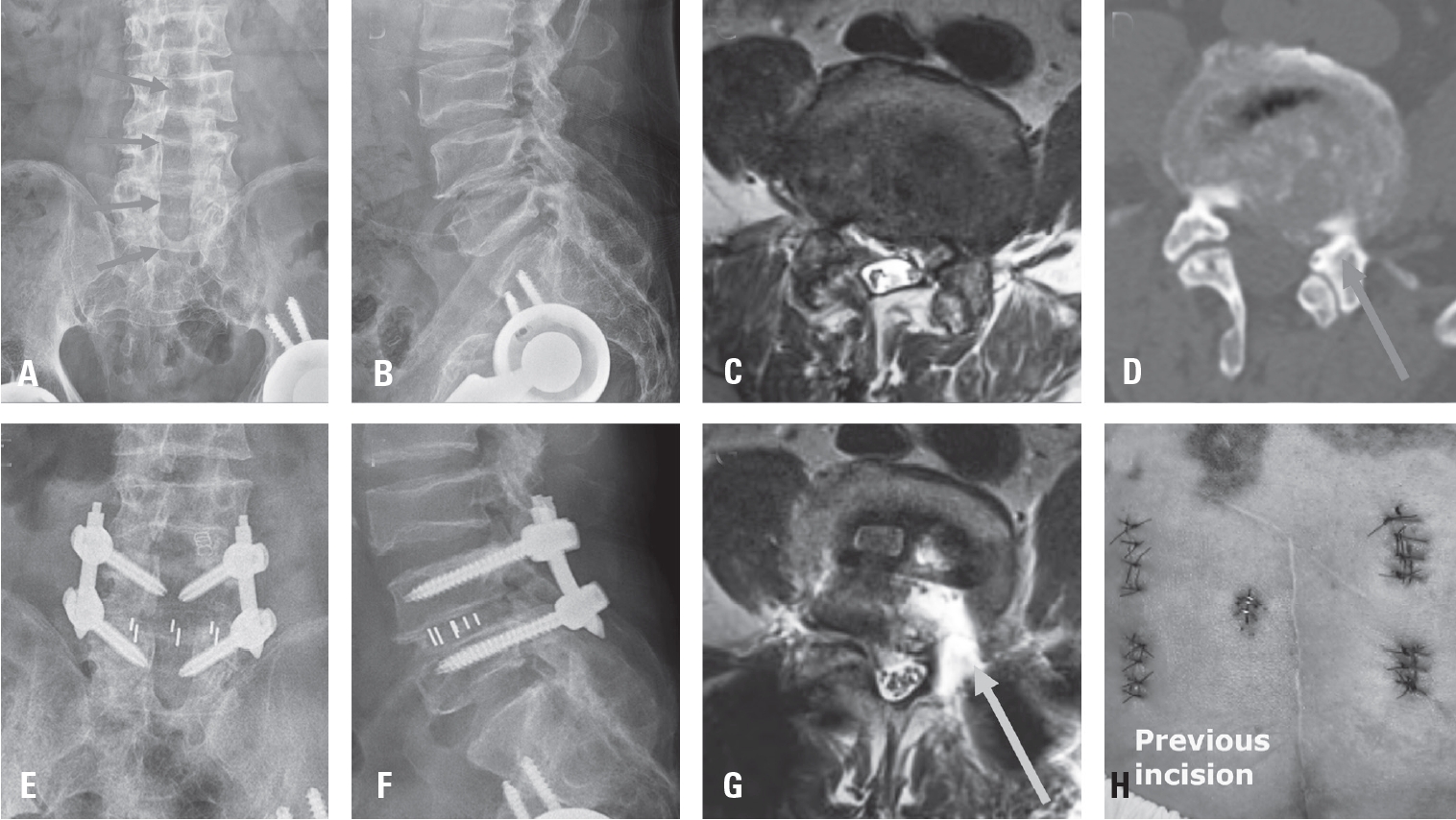
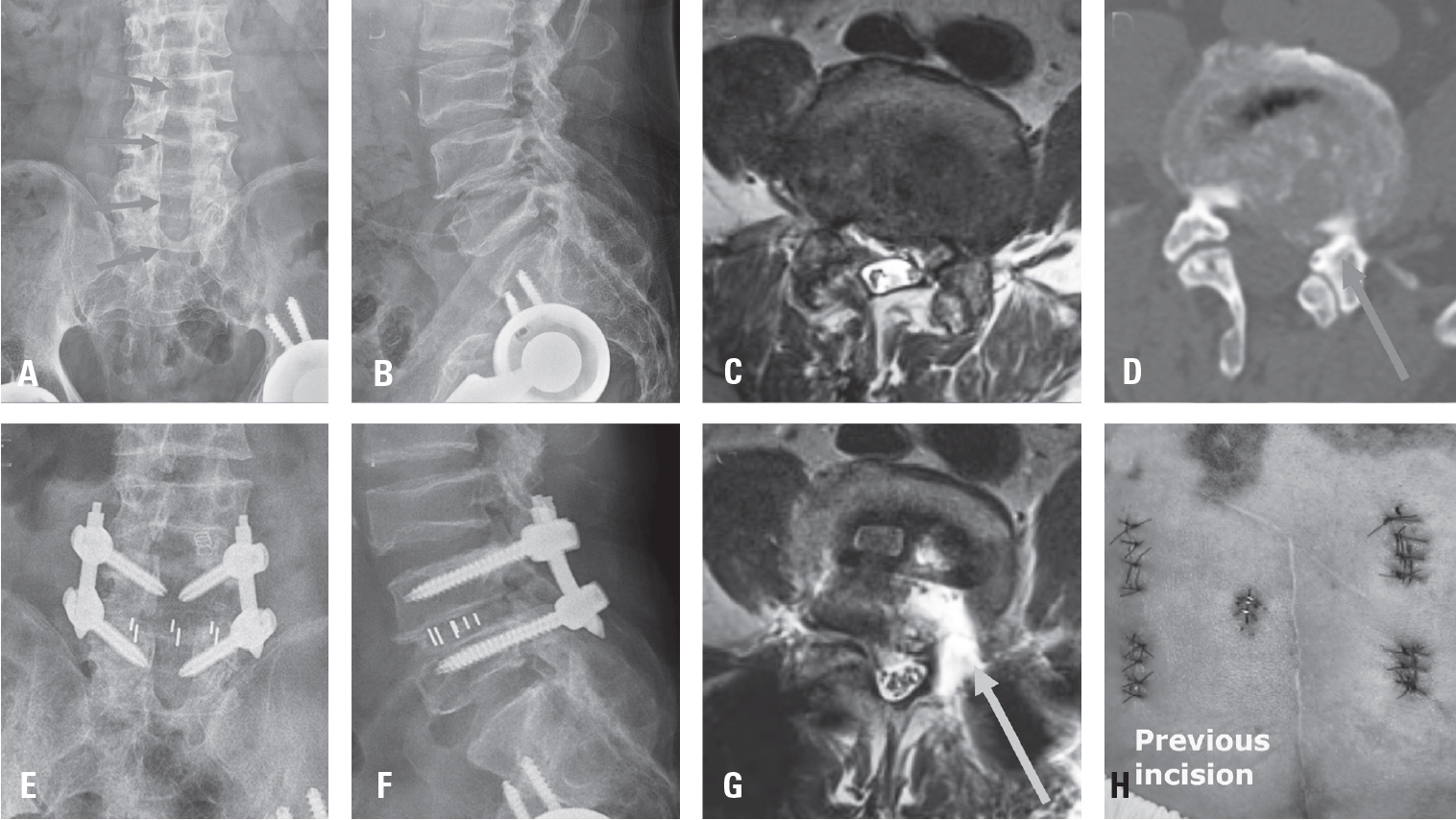
Representative case of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF). A 66-year-old man with recurrent left-sided radicular pain 10 years after extensive posterior decompression. (A, B) Preoperative radiographic images demonstrating extensive laminectomy on the left side at the L3–4, L4–5, and L5–S1 levels. (C) Preoperative axial MRI showing adhesive epidural fibrosis and a recurrent disc fragment compressing the left exiting nerve root. (D) Axial CT image demonstrating the previous hemilaminectomy site at the L4–5 level. (E, F) Postoperative radiographs showing proper interbody cage placement and restoration of disc height. (G) Postoperative axial MRI demonstrating adequate neural decompression and appropriate cage positioning. (H) Revision incision placed to avoid the previous surgical incision.BE-REFLIF, biportal endoscopic revision extraforaminal lumbar interbody fusion; CT, computed tomography; MRI, magnetic resonance imaging.
Table 1.
Demographic data
Variable
Value
Age (years)
67.2±11.2
Male / Female (N)
11:9
Height (cm)
158.0±8.2
Weight (Kg)
65.3±11.5
Asa
I
8 (40)
II
12 (60)
Body mass index (kg/m2)
26.1±3.1
Bone mineral density (T-score)
-1.2±1.2
Operation level (%)
L2-3
1 (5)
L3-4
3 (15)
L4-5
12 (60)
L5-S1
4 (20)
Operation time (min)
200.8±42.5
Hospital stay
19.1±4.8
Values are presented as mean±standard deviation.
Table 2.
Clinical outcome measures : VAS score for Back and Leg pain and ODI score, EQ-5D
Variable
Value
Differene (95%CI)
p-value
VAS-Back
Preop
6.15±2.01
Postop 1M
3.75±1.86
Postop 6M
2.95±1.28
Postop 12M
2.95±1.32
Interaction
-0.20 (-0.27 to -0.13)
<0.001
VAS-Leg
Preop
6.5±2.4
Postop 1M
2.45±1.47
Postop 6M
1.8±1.4
Postop 12M
1.65±1.53
Interaction
-0.28 (-0.39 to -0.18)
<0.001
ODI
Preop
31.4±7.6
Postop 1M
21.3±8.63
Postop 6M
13.65±5.58
Postop 12M
9.8±6.14
Interaction
-1.6 (-1.9 to -1.2)
<0.001
EQ-5D
Preop
-0.18±0.03
Postop 1M
0.18±0.49
Postop 6M
0.73±0.22
Postop 12M
0.81±0.06
Interaction
0.08 (0.06 to 0.09)
<0.001
Values are presented as mean±standard deviation. VAS: visual analogue scale, ODI: Oswestry disability Index.
Table 3.
Radiologic outcomes.
Variable
Preoperative
Postoperative
Difference
p-value
Disc Height (mm)
8.4±2.4
12.8±1.5
4.4±1.9
<0.001
Segmental Sagittal angle (˚)
5.7±4.6
9.7±4.8
4.1±4.5
<0.001
Segmental Coronal angle (˚)
2.5±2.6
0.9±0.6
-1.6±2.6
0.014
Lumbar lordosis (˚)
35.1±12.4
40.8±10.7
5.7±5.4
<0.001
Fusion grade (%)
6 (30)
11 (55)
3 (15)
0 (0)
Fusion (%)
17 (85)
3 (15)
Cage Subsidence
5 (25)
Values are presented as mean±standard deviation.
Table 4.
Laboratory outcomes measures
Variable
Value
Estimated blood loss (ml)
273.9±240.9
Mean transfusion (%)
0
21 (87.5)
1
3 (12.5)
Preop hemoglobin (g/dL)
13.0±1.3
Postop hemoglobin (g/dL)
12.1±1.2
ΔHb (%)
6.9±4.1
Preoperative CPK (IU/L)
104.0±50.5
Postop 1 day CPK
573.4±365.4
Postop 1 week CPK
110.3±75.2
Postop 2 weeks CPK
117.6±218.3
Preoperative CRP (mg/L)
2.2±2.5
Postop 1 day CRP
79.1±42.8
Postop 1 week CRP
20.3±13.4
Postop 2 weeks CRP
17.6±55.5
Values are presented as mean±standard deviation.
Table 5.
Surgical complications
Variable
Value
Dural tear
2 (10)
Epidural hematoma
1 (5)
Incomplete decompression
0 (0)
Surgical site infection
1 (5)
Transient nerve root injury
0 (0)
References
1. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 2008;358:794-810.
2. Malmivaara A, Slätis P, Heliövaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine (Phila Pa 1976) 2007;32:1-8.
4. Radcliff K, Curry P, Hilibrand A, et al. Risk for adjacent segment and same segment reoperation after surgery for lumbar stenosis: a subgroup analysis of the SPORT trial. Spine (Phila Pa 1976) 2013;38:531-9.
5. Martin BI, Mirza SK, Comstock BA, et al. Reoperation rates following lumbar spine surgery and the influence of spinal fusion procedures. Spine (Phila Pa 1976) 2007;32:382-7.
7. Khan IS, Sonig A, Thakur JD, et al. Perioperative complications in patients undergoing open TLIF as a revision surgery. J Neurosurg Spine 2013;18:260-4.
9. Jin C, Xie M, He L, et al. Oblique lumbar interbody fusion for adjacent segment disease after posterior lumbar fusion: a case-controlled study. J Orthop Surg Res 2019;14:216.
11. Park SJ, Hwang JM, Cho DC, et al. Indirect decompression using OLIF revision surgery following previous posterior decompression. Neurospine 2022;19(3):544-54.
12. Heo DH, Kim HS, Whang YH, et al. History of endoscopic spine surgery: development of indications and techniques. Spine J 2025 (in press).
13. Yang HS, Heo DH, Park JY. Biportal endoscopic approach for lumbar central stenosis. In: Kim HS, , editor. Advanced Techniques of Endoscopic Lumbar Spine Surgery. Singapore: Springer; 2020. p. 45-54.
14. Park DY, Upfill-Brown A, Curtin N, et al. Clinical outcomes and complications after biportal endoscopic spine surgery: a systematic review and meta-analysis of 3673 cases. Eur Spine J 2023;32:2637-46.
15. Hwang YH, Kim JS, Chough CK, et al. Prospective comparative analysis of three types of decompressive surgery for lumbar central stenosis. Sci Rep 2024;14:19853.
16. Park SM, Song KS, Ham DW, et al. Safety profile of biportal endoscopic spine surgery compared with conventional microscopic approach: pooled analysis of two RCTs. Neurospine 2024;21(4):1190-8.
18. Song KS, Lee CW, Moon JG. Biportal endoscopic spinal surgery for bilateral lumbar foraminal decompression: report of 2 cases with technical note. Neurospine 2019;16(1):138-47.
Clinical and Radiological Outcomes of Biportal Endoscopic Revision Extraforaminal Lumbar Interbody Fusion Following Previous Central Decompression: A Case Series
Fig. 1. Portal placement and fluoroscopic landmarks for biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF).
Surgical incisions for BE-EFLIF using multiportal approach. P+2 ports mean that it is made 2 cm lateral to the pedicle lateral margin, and are used for facetectomy and foraminotomy. Based on when a right-handed surgeon performs a left side approach, the port on the left used as a viewing port is called P+2 (L) port, and the port on the right used as a working port is called P+2 (R) port. Additional M ports are made to perform Root retraction during cage insertion or accomodate the endoscope. BE-EFLIF, biportal endoscopic extraforaminal lumbar interbody fusion
Fig. 2. Schematic illustration of the extraforaminal working corridor for biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) in a previously decompressed segment. (A) Targeting of the remnant inferior articular process (IAP) and the superior articular process (SAP) to define the bony boundaries of the working corridor. (B) Illustration of the established extraforaminal corridor used for interbody cage insertion. (C) Visualization of the opened disc space between the exiting nerve root and the traversing nerve root after adequate decompression. (D) Measurement of the distance between the traversing and exiting nerve roots, demonstrating a minimum required safety margin of 15 mm to allow safe insertion of the interbody cage.
Fig. 3. Visualization of endplate preparation during biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF). (A) Endoscopic view obtained through the medial portal demonstrating inspection of adequate endplate preparation prior to cage insertion. (B) Endoscopic view using a 30° scope to evaluate the medial aspect of the endplate, allowing confirmation of complete disc removal and appropriate endplate preparation
Fig. 4. Representative case of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF). A 66-year-old man with recurrent left-sided radicular pain 10 years after extensive posterior decompression. (A, B) Preoperative radiographic images demonstrating extensive laminectomy on the left side at the L3–4, L4–5, and L5–S1 levels. (C) Preoperative axial MRI showing adhesive epidural fibrosis and a recurrent disc fragment compressing the left exiting nerve root. (D) Axial CT image demonstrating the previous hemilaminectomy site at the L4–5 level. (E, F) Postoperative radiographs showing proper interbody cage placement and restoration of disc height. (G) Postoperative axial MRI demonstrating adequate neural decompression and appropriate cage positioning. (H) Revision incision placed to avoid the previous surgical incision.BE-REFLIF, biportal endoscopic revision extraforaminal lumbar interbody fusion; CT, computed tomography; MRI, magnetic resonance imaging.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Clinical and Radiological Outcomes of Biportal Endoscopic Revision Extraforaminal Lumbar Interbody Fusion Following Previous Central Decompression: A Case Series
Variable
Value
Age (years)
67.2±11.2
Male / Female (N)
11:9
Height (cm)
158.0±8.2
Weight (Kg)
65.3±11.5
Asa
I
8 (40)
II
12 (60)
Body mass index (kg/m2)
26.1±3.1
Bone mineral density (T-score)
-1.2±1.2
Operation level (%)
L2-3
1 (5)
L3-4
3 (15)
L4-5
12 (60)
L5-S1
4 (20)
Operation time (min)
200.8±42.5
Hospital stay
19.1±4.8
Variable
Value
Differene (95%CI)
p-value
VAS-Back
Preop
6.15±2.01
Postop 1M
3.75±1.86
Postop 6M
2.95±1.28
Postop 12M
2.95±1.32
Interaction
-0.20 (-0.27 to -0.13)
<0.001
VAS-Leg
Preop
6.5±2.4
Postop 1M
2.45±1.47
Postop 6M
1.8±1.4
Postop 12M
1.65±1.53
Interaction
-0.28 (-0.39 to -0.18)
<0.001
ODI
Preop
31.4±7.6
Postop 1M
21.3±8.63
Postop 6M
13.65±5.58
Postop 12M
9.8±6.14
Interaction
-1.6 (-1.9 to -1.2)
<0.001
EQ-5D
Preop
-0.18±0.03
Postop 1M
0.18±0.49
Postop 6M
0.73±0.22
Postop 12M
0.81±0.06
Interaction
0.08 (0.06 to 0.09)
<0.001
Variable
Preoperative
Postoperative
Difference
p-value
Disc Height (mm)
8.4±2.4
12.8±1.5
4.4±1.9
<0.001
Segmental Sagittal angle (˚)
5.7±4.6
9.7±4.8
4.1±4.5
<0.001
Segmental Coronal angle (˚)
2.5±2.6
0.9±0.6
-1.6±2.6
0.014
Lumbar lordosis (˚)
35.1±12.4
40.8±10.7
5.7±5.4
<0.001
Fusion grade (%)
6 (30)
11 (55)
3 (15)
0 (0)
Fusion (%)
17 (85)
3 (15)
Cage Subsidence
5 (25)
Variable
Value
Estimated blood loss (ml)
273.9±240.9
Mean transfusion (%)
0
21 (87.5)
1
3 (12.5)
Preop hemoglobin (g/dL)
13.0±1.3
Postop hemoglobin (g/dL)
12.1±1.2
ΔHb (%)
6.9±4.1
Preoperative CPK (IU/L)
104.0±50.5
Postop 1 day CPK
573.4±365.4
Postop 1 week CPK
110.3±75.2
Postop 2 weeks CPK
117.6±218.3
Preoperative CRP (mg/L)
2.2±2.5
Postop 1 day CRP
79.1±42.8
Postop 1 week CRP
20.3±13.4
Postop 2 weeks CRP
17.6±55.5
Variable
Value
Dural tear
2 (10)
Epidural hematoma
1 (5)
Incomplete decompression
0 (0)
Surgical site infection
1 (5)
Transient nerve root injury
0 (0)
Table 1. Demographic data
Values are presented as mean±standard deviation.
Table 2. Clinical outcome measures : VAS score for Back and Leg pain and ODI score, EQ-5D
Values are presented as mean±standard deviation. VAS: visual analogue scale, ODI: Oswestry disability Index.