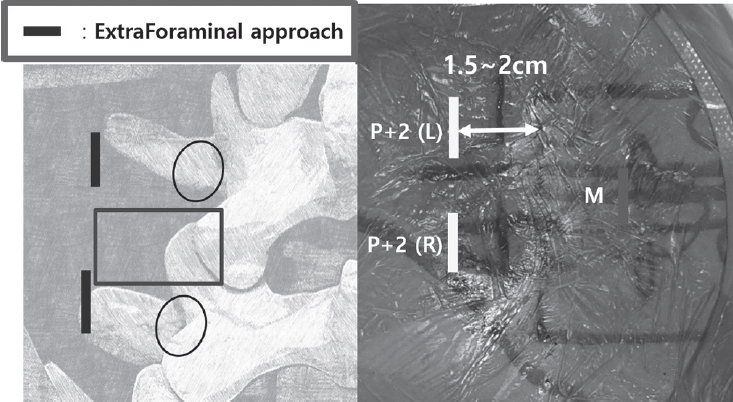
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Background This study aims to assess the clinical and radiographic outcomes of biportal endoscopic lumbar discectomy compared to microscopic lumbar discectomy in obese patients with lumbar herniated discs. Previous research has established a positive correlation between operation time and estimated blood loss in obese patients undergoing microscopic lumbar discectomy, based on an increase in body mass index. However, no studies have specifically examined the outcomes of biportal endoscopic lumbar discectomy in this patient population. Therefore, this study seeks to fill this research gap and provide valuable insights into the effectiveness of these two surgical approaches for obese patients with lumbar herniated discs.
Methods This retrospective multicenter study analyzed and compared clinical and radiological data from 48 obese patients with a body mass index (BMI) greater than 30 kg/m2 who underwent either microscopic or biportal endoscopic lumbar discectomy. The study assessed clinical outcomes using the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores. Radiological data were obtained through magnetic resonance imaging (MRI) scans.
Results The study included a total of 48 patients, with 31 patients undergoing microscopic discectomy and 17 patients undergoing biportal endoscopic discectomy. Both groups showed improvements in VAS, ODI, and EQ-5D scores following surgery compared to preoperative scores. However, there was no significant difference in these outcome measures between the two surgical techniques. Although there was a no significant difference in the occurrence of recurrent disc herniation confirmed by postoperative MRI, there was significant difference in the number of patients requiring additional surgery between the two groups.
Conclusions For obese patients with lumbar disc herniation that did not respond to conservative treatment, this study found no significant differences in clinical or radiological outcomes between microscopic and biportal endoscopic surgery methods. However, it is worth noting that the biportal group had a lower incidence of reoperation compared to the microscopic group.
Background When obese patients underwent lumbar discectomy using a microscope, a correlation was found between the operation time and an increase in estimated blood loss according to the increase in body mass index.
However, except for minor complications, there was no difference in postoperative outcomes between obese and normal-weight patients. These are the results of microscopic lumbar discectomy in obese patients, but there are no studies on biportal endoscopic lumbar discectomy. The aim of this study was to compare the clinical and radiographic outcomes of microscopic and endoscopic discectomy in obese patients.
Methods Clinical and radiological data were compared and analyzed in 23 obese patients with a body mass index of >30 kg/m2 who underwent microscopic and biportal endoscopic lumbar discectomy. Clinical data on the visual analog scale (VAS), Oswestry Disability Index (ODI), and EuroQol-5D (EQ-5D) scores were measured, and radiological data were measured using magnetic resonance imaging (MRI).
Results In total, 13 patients who underwent microscopic discectomy and 10 who underwent biportal endoscopic discectomy were enrolled in this study. The VAS, ODI, and EQ-5D scores in both groups improved after surgery compared with those before surgery, although there was no difference between the two groups. Although there was a difference in the incidence of recurrent disc herniation confirmed by MRI after surgery, there was no difference in the number of patients requiring surgery between the two groups.
Conclusions There were no significant clinical or radiological differences in outcomes between microscopic and biportal endoscopic surgery methods.

 First
First Prev
Prev

