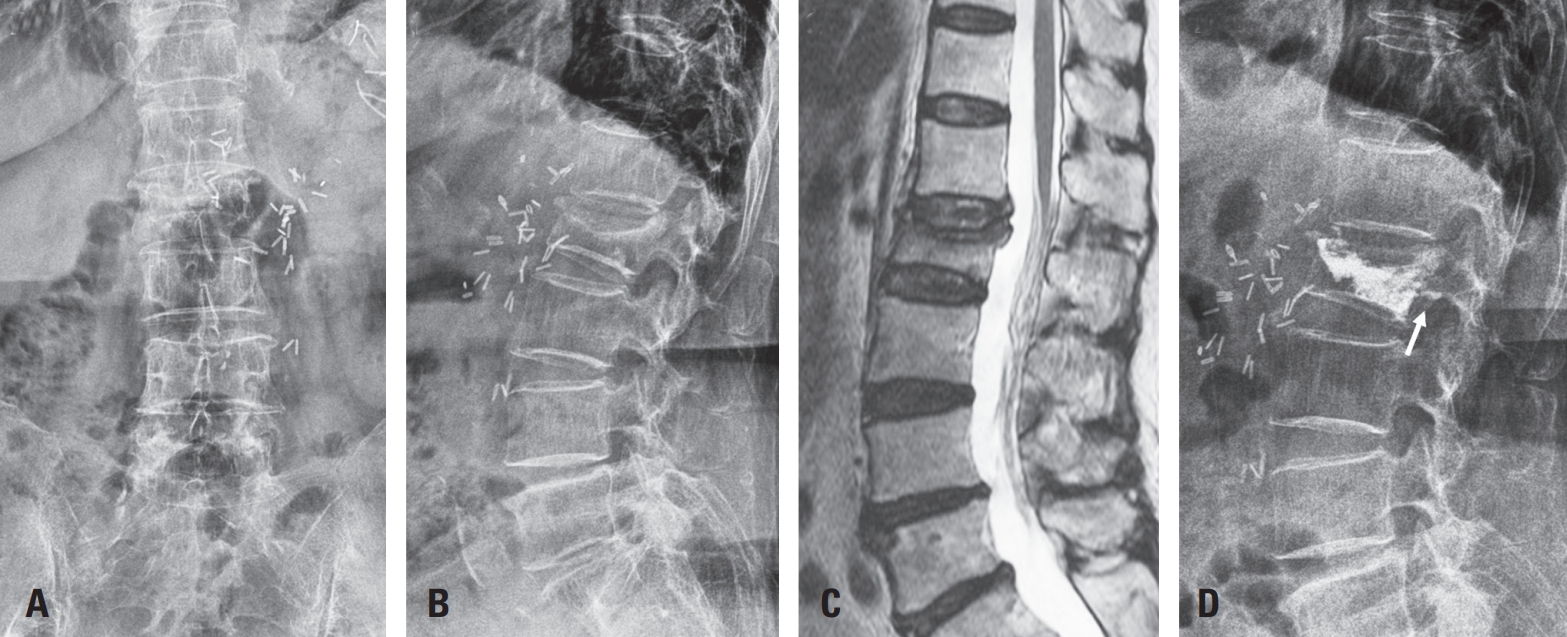
Vertebroplasty or kyphoplasty is a widely accepted minimally invasive procedure for treating painful vertebral compression fractures. Although considered safe, rare but serious complications such as spinal subdural hematoma (SDH) can occur, particularly in patients receiving long-term anticoagulation therapy. We present a rare case of spinal SDH following kyphoplasty in a 78-year-old woman with a mechanical aortic valve on chronic warfarin therapy. Anticoagulation was managed perioperatively with warfarin discontinuation and bridging enoxaparin. Postoperative X-ray showed subtle posterior cement leakage. MRI on postoperative day 1 revealed lumbar SDH, which progressed cranially by day 2. The patient remained neurologically intact and was treated conservatively with corticosteroids and temporary suspension of anticoagulation. Follow-up imaging showed gradual hematoma resolution, and she was discharged without deficits. This case suggests the importance of maintaining a high index of suspicion for spinal hematoma in anticoagulated patients, especially when new symptoms or even minor cement leakage are present. Careful perioperative planning, including early imaging and multidisciplinary management, is crucial in such high-risk patients.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
When conservative treatment fails in the treatment of osteoporotic vertebral compression fractures, a minimally invasive procedure, such as percutaneous balloon kyphoplasty or vertebroplasty is performed. Among these, balloon kyphoplasty is known as an advantageous method for lower risk of cement leakage and greater correction effect of kyphosis and better sagittal balance correction. However, there are reports of various complications during and after procedure, and sometimes result in serious consequences. This paper reviews with previous literatures about the complications related to balloon kyphoplasty.
Purpose To evaluate long term efficacy of percutaneous balloon kyphoplasty for osteoporotic compressive vertebral fracture.
Materials and Methods Percutaneous balloon kyphoplasty was performed to 52 vertebral bodies, for 42 patients with compression fracture from March 2003 to October 2007. During observation, 32 patients (39 vertebral bodies) were followed over 5 years except 8 patients (19.0%) who have expired. Pre operational, post operational and final observational radiologic evaluation (vertebral height, compression ratio, kyphotic angle) and clinic evaluation(VAS score) were checked. And correlation with bone cement leakage, fracture of adjacent vertebral body, gender, age, bone mineral density and medication was analyzed.
Result Average age was 71.3 years old and average observation period was 74.3 months. Average interval from injury to operation was 24.1 days. Vertebral compression ratio recovered 29.7% to 17.4% (12.3%), kyphotic angle improved 11.6 degree to 9.0 degree (2.6 degree) and there was no significant change until final observation. VAS score got better 7.60 to 3.57 (4.03) after operation. Bone cement leakage occurred in 5 cases (12.8%) and fracture of adjacent vertebral body occurred in 10 cases (25.6%), there was no correlation between two groups (p=1.000). Fracture of adjacent vertebral body showed meaningful correlation with bone mineral density only.
Conclusion Percutaneous balloon kyphoplasty relieve the pain after compression fracture of vertebral body and is safe and efficient procedure to correct sagittal deformity. After 5 year follow up, the effect of procedure was maintained clinically. Bone cement leakage did not increase risk of fracture of adjacent vertebral body which occurred frequently in low bone mineral density.
Purpose To find the factors that affecting surgical outcome after vertebroplasty and kyphoplasty in osteoporotic compression fracture.
Materials and Methods Pre-operative, post-operative, technical, radiological factors of patients who diagnosed osteoporotic compression fracture and treated with vertebroplasty or kypholasty during from January 2008 to December 2010, were compared by outcomes that acute and chronic back pain, refracture rate and maintenance of the reduction of body height.
Results The period of acute pain after the operation was less than 3 days in groups of trauma( p=0.0262) and hospital treatment(p=0.0113) before the operation as pre-operative factors. When it comes to technical factors, the cases of vertebroplasty(p<0.0001), injection of cement(p=0.0053), the case without leakage of cement(p=0.007) and the case being under anesthesia (p<0.005)achieved statistical significance. In the groups who got conservative treatment less than 1 week (p=0.0119) and local anesthetics(p=0.0246), refractures occurred many times. The groups of non-trauma(p=0.0105), having had more than 30% compression(p=0.0244) and the group that prescribed bisphosphonate(p=0.0286) statistical significantly maintained restoration.
Conclusion Conservative treatment in the hospital for more than 1 week before the operation, operation being under anesthesia and intake of bisphosphonate after the operation put positive effects on the outcome of vertebroplasty and kyphoplasty.

 First
First Prev
Prev

