Department of Orthopaedic Surgery, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Corresponding author: Hyung-Youl Park, M.D., Ph.D. Department of Orthopedic Surgery, Eunpyeong St. Mary's Hospital, College of Medicine, The Catholic University of Korea, 1021, Tongil-ro, Eunpyeong-Ku, Seoul, 03321, Korea TEL: +82-2-2030-4806, FAX: +82-2-2030-4629 E-mail: matrixbest@naver.com
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Vertebroplasty or kyphoplasty is a widely accepted minimally invasive procedure for treating painful vertebral compression fractures. Although considered safe, rare but serious complications such as spinal subdural hematoma (SDH) can occur, particularly in patients receiving long-term anticoagulation therapy. We present a rare case of spinal SDH following kyphoplasty in a 78-year-old woman with a mechanical aortic valve on chronic warfarin therapy. Anticoagulation was managed perioperatively with warfarin discontinuation and bridging enoxaparin. Postoperative X-ray showed subtle posterior cement leakage. MRI on postoperative day 1 revealed lumbar SDH, which progressed cranially by day 2. The patient remained neurologically intact and was treated conservatively with corticosteroids and temporary suspension of anticoagulation. Follow-up imaging showed gradual hematoma resolution, and she was discharged without deficits. This case suggests the importance of maintaining a high index of suspicion for spinal hematoma in anticoagulated patients, especially when new symptoms or even minor cement leakage are present. Careful perioperative planning, including early imaging and multidisciplinary management, is crucial in such high-risk patients.
척추 압박골절에 대한 치료로 척추성형술(vertebroplasty) 또는 척추후만성형술(kyphoplasty)은 널리 시행되는 최소침습적 시술이다. 일반적으로 안전한 시술로 간주되지만, 드물게 심각한 합병증이 발생할 수 있으며, 특히 장기간 항응고 치료를 받고 있는 환자에서 척추 경막하 혈종(spinal subdural hematoma, SDH)과 같은 중대한 합병증이 보고되고 있다. 본 증례는 기계식 대동맥 판막을 이식받고 만성적으로 와파린(warfarin)을 복용 중이던 78세 여성에서 척추후만성형술 시행 후 발생한 척추 경막하 혈종 사례이다. 수술 전후 항응고 관리는 와파린 중단 후 에녹사파린(enoxaparin)으로 교량 요법(bridging therapy)을 시행하였다. 수술 후 단순 방사선 검사에서 경미한 후방 시멘트 누출이 관찰되었으며, 수술 다음 날 시행한 MRI에서는 요추부 경막하 혈종이 확인되었고, 이 혈종은 이후 상부 흉추까지 진행되었다. 환자는 신경학적으로 안정된 상태를 유지하였으며, 스테로이드 치료 및 항응고제 일시 중단을 포함한 보존적 치료를 시행하였다. 이후 추적 영상에서 혈종의 점진적 흡수가 확인되었고, 환자는 신경학적 결손 없이 퇴원하였다. 본 증례는 장기간 항응고 치료를 받는 고위험 환자에서 새로운 증상이 발생하거나 사소한 시멘트 누출이 보이는 경우에도 척추 혈종의 가능성을 항상 염두에 두는 것이 중요함을 시사한다. 고위험 환자에서는 조기 영상 검사 및 다학제적 접근을 포함한 신중한 수술 전후 계획 수립이 중요하다.
Vertebroplasty (VP) or kyphoplasty (KP) is a widely accepted minimally invasive treatment for painful vertebral compression fractures, especially in elderly osteoporotic patients.1,2) Although generally considered safe, complications such as cement leakage, infection, or adjacent vertebral fractures may occur. Neurological complications, including epidural or subdural hematomas, are exceedingly rare but potentially serious.3,4)
Subdural spinal hematoma (SDH) after VP or KP is rare but can occur, and the risk may be further increased in patients requiring long-term anticoagulation.5,6) Management of such patients presents a clinical dilemma between preventing thromboembolic events and minimizing bleeding risk.7,8) We present a rare case of spinal subdural hematoma following KP in a patient on chronic warfarin therapy for a mechanical aortic valve, along with a brief review of the literature.
Case Report
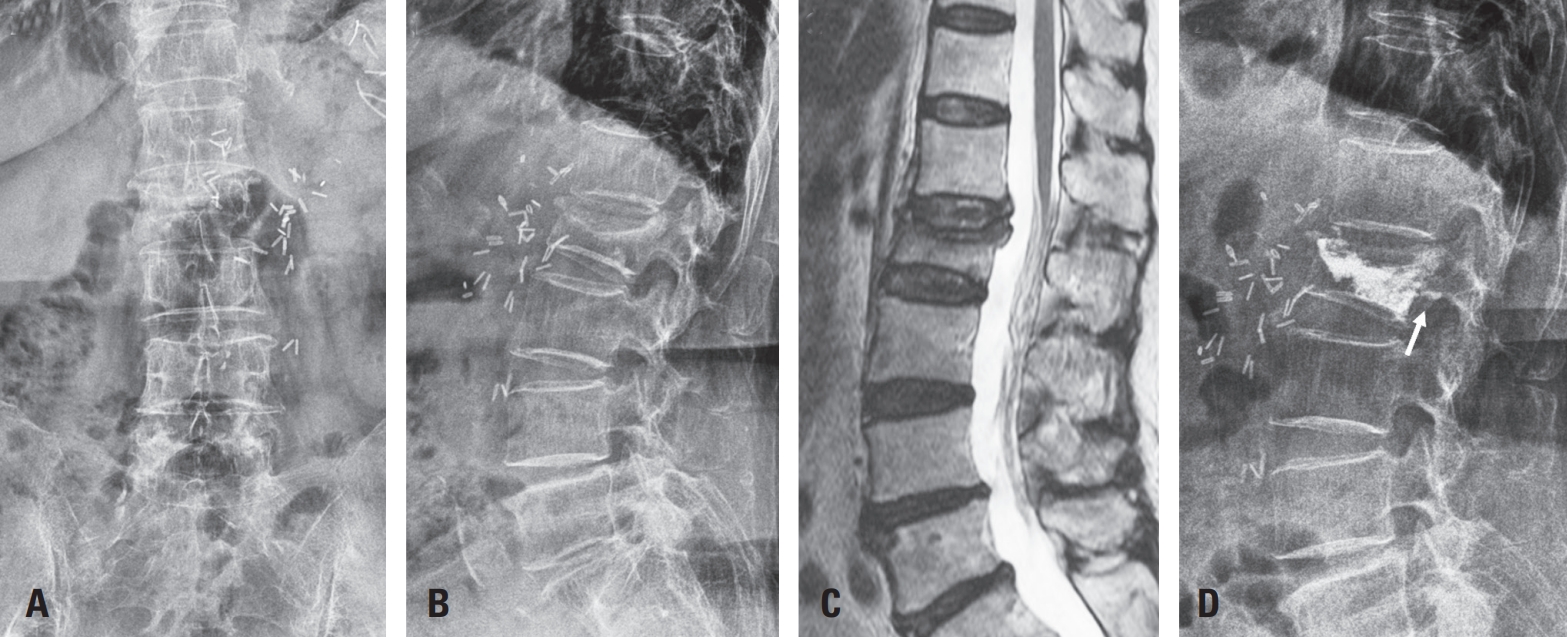
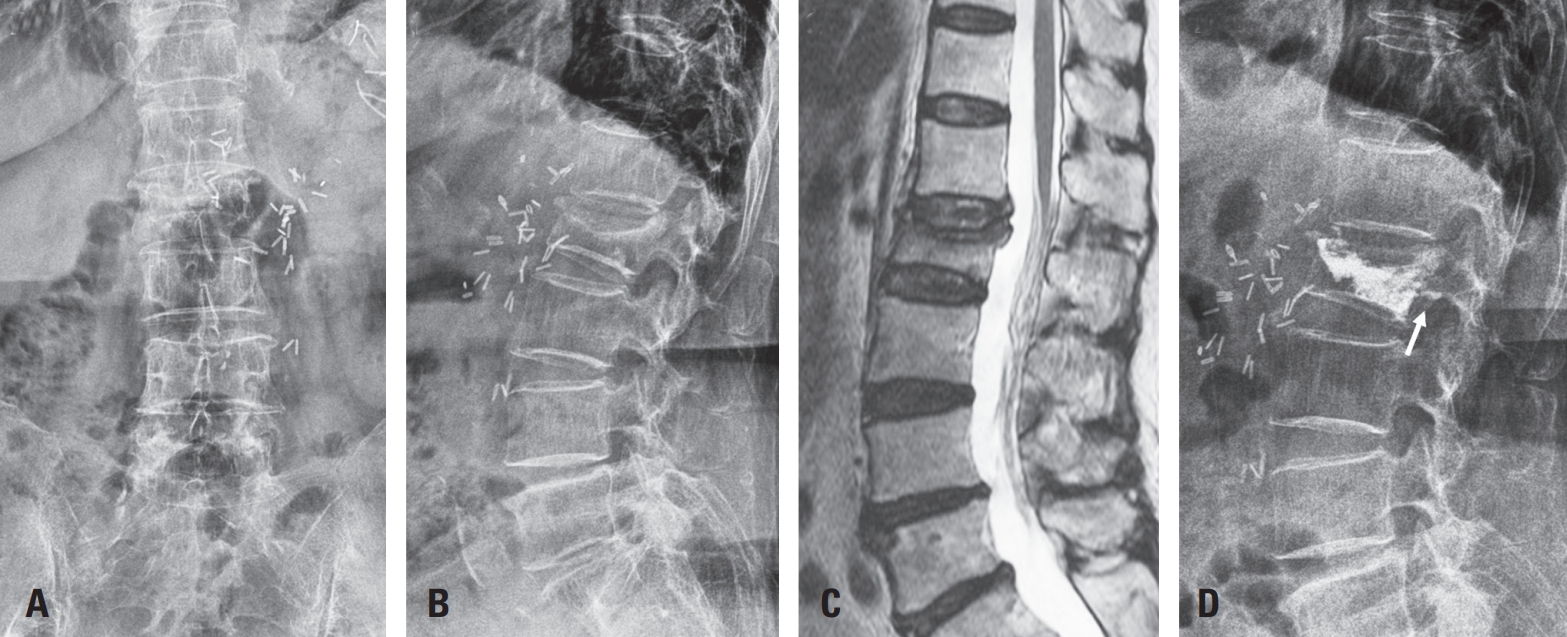
A 78-year-old woman with a history of hypertension, hyperlipidemia, and two prior aortic surgeries for aortic dissection had undergone mechanical aortic valve replacement and was on long-term warfarin therapy (2.5 mg daily). She presented with lower back pain and was diagnosed with an L2 compression fracture, initially managed conservatively (Fig. 1A–C).
Due to persistent symptoms, kyphoplasty was performed after discontinuation of warfarin and bridging with enoxaparin. The procedure was uneventful, though postoperative X-ray showed mild posterior cement leakage (Fig. 1D). Enoxaparin (50 mg twice daily) was resumed for anticoagulation.
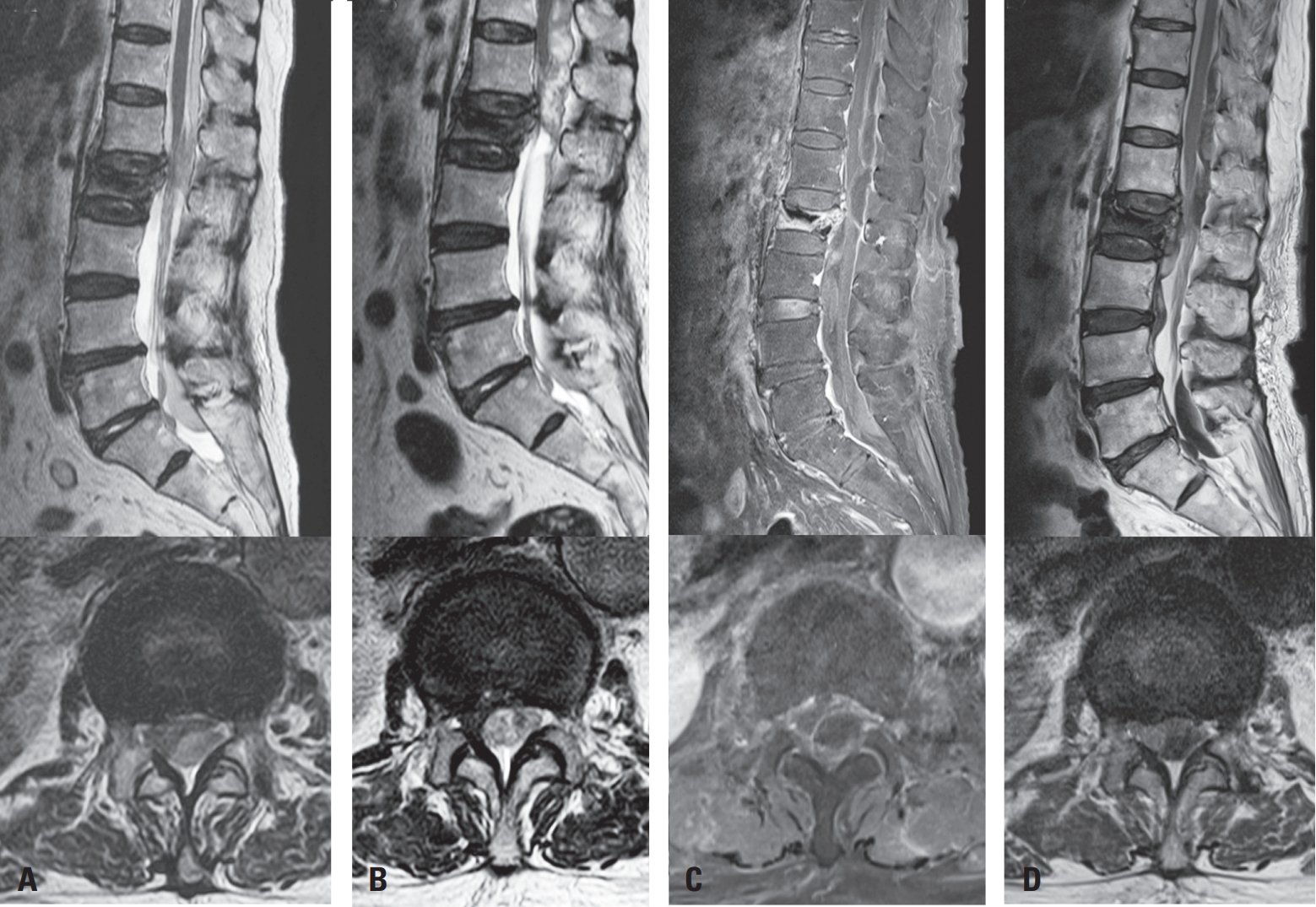
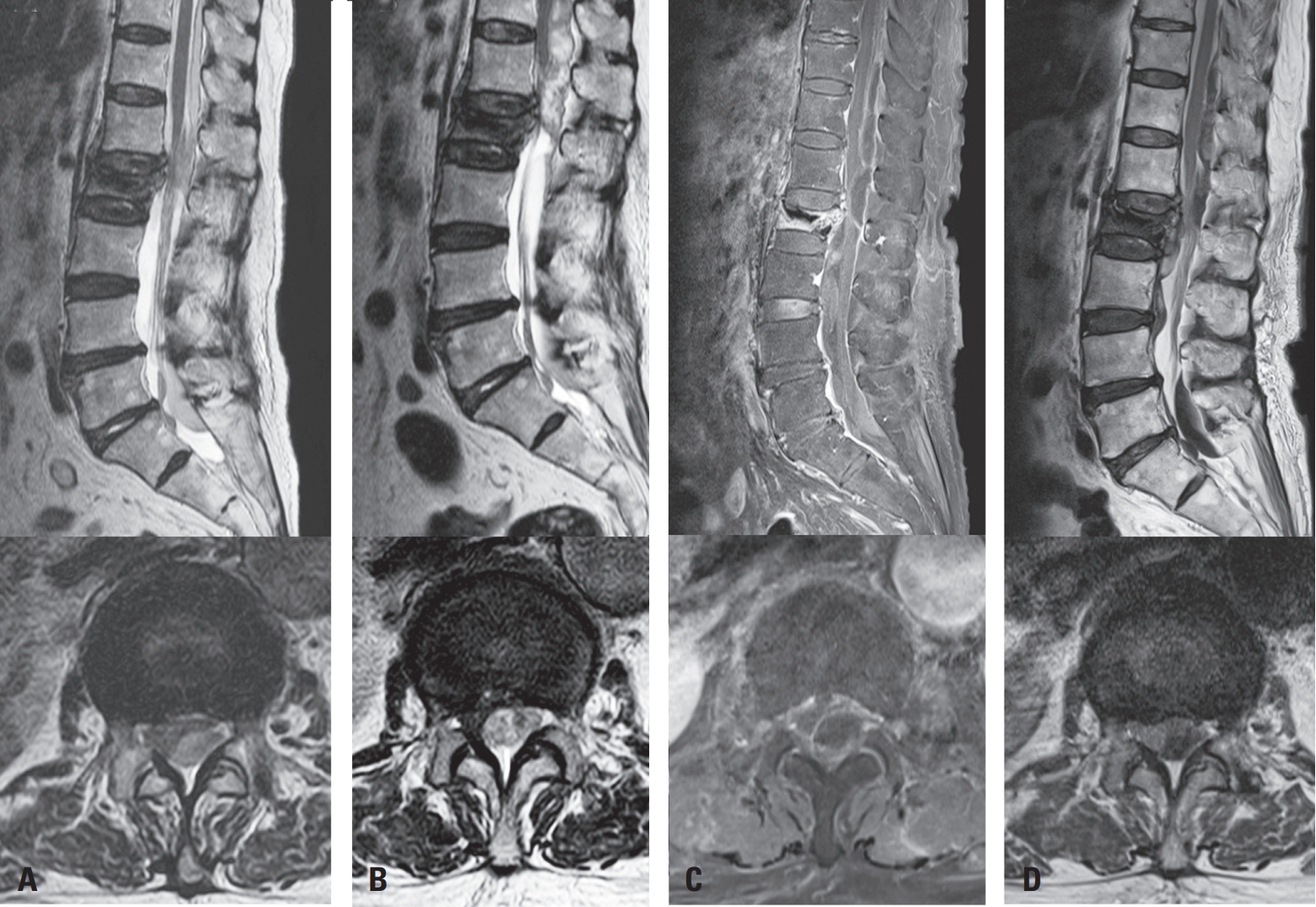
Routine MRI on POD 1 revealed a subdural hematoma at L1–2 and L5–S1 (Fig. 2A), which progressed cranially to the thoracic spine by POD 2 (Fig. 2B). The patient developed new back and buttock pain but remained neurologically intact. Intravenous dexamethasone (4 mg every 6 hours) was administered per spinal cord compression protocol.9)
On POD 3, the patient was transferred to our institution for further evaluation. Neurologic examination revealed intact motor and sensory function without signs of myelopathy, and her back pain had partially improved with corticosteroids. A multidisciplinary discussion with cardiology and cardiothoracic surgery teams was held, and anticoagulation was temporarily withheld due to the relatively lower thromboembolic risk associated with mechanical aortic valves.8)
On POD 4, follow-up MRI showed no further cranial extension of the thoracic subdural hematoma but revealed a new subdural hematoma at the L3–4 level (Fig. 2C). As the patient remained neurologically stable without new symptoms, enoxaparin (50 mg twice daily) was resumed on POD 6, and corticosteroids were gradually tapered.
By POD 11, MRI demonstrated partial resolution of the hematoma with a mixed subdural and epidural appearance (Fig. 2D). Warfarin was reintroduced and gradually resumed at the original dose. The patient was discharged without neurological complications and remained symptom-free at one-month follow-up. This case was conducted in accordance with institutional ethical guidelines and approved by the Institutional Review Board of Eunpyeong St. Mary’s Hospital (IRB No. PC25ZISI0119).
Discussion
SDH following VP or KP is exceedingly rare, with only a limited number of cases reported in the literature (Table 1). Based on our review of 11 published cases identified in the literature through database search, most patients developed symptoms within hours to a few days postoperatively, although delayed presentations—up to two weeks—were also observed.5,6,10-16)
Two of the most recent and severe cases involved kyphoplasty in patients receiving anticoagulation. Mrad et al.6) described a case of paraplegia progressing to tetraplegia due to extensive hematoma in a patient on therapeutic anticoagulation. Despite decompressive laminectomy and hematoma evacuation, neurological recovery was only gradual. Similarly, Kaplan et al.5) reported SDH and subsequent epidural hematoma (SEH) within three days post-kyphoplasty in an anticoagulated patient; surgical decompression led to partial improvement.
By contrast, Lee et al.11) presented a unique case of delayed SDH following vertebroplasty that was successfully managed with corticosteroids alone, suggesting that conservative treatment may be feasible in select cases with mild or non-progressive symptoms.
Our case represents the first reported instance of SDH following kyphoplasty in a patient with a mechanical aortic valve on long-term warfarin therapy. Despite the high thrombotic risk associated with valve replacement, anticoagulation was carefully suspended, and the patient was treated conservatively with intravenous dexamethasone and close monitoring.9) Neurological function remained stable throughout the clinical course, and the hematoma showed gradual resolution.
However, this case illustrates the clinical dilemma of anticoagulation management in patients with mechanical heart valves. While these patients carry an inherent thrombotic risk, perioperative anticoagulation can increase the risk of bleeding complications.8) Balancing the competing risks of thrombosis and hematoma progression was especially challenging.7) With multidisciplinary input, anticoagulation was temporarily withheld under close monitoring and later resumed without neurological deterioration. This outcome supports the feasibility of individualized, risk-adapted anticoagulation protocols in select high-risk patients.
While the precise pathogenesis of spinal subdural hematoma remains unclear, multiple risk factors have been proposed. These include anticoagulation, mechanical trauma during needle insertion (particularly pedicle breach), and abrupt increases in venous pressure during cement injection. 12,13) In anticoagulated patients, even minor venous injury or pressure fluctuations may lead to clinically significant hematoma.5,6,15)
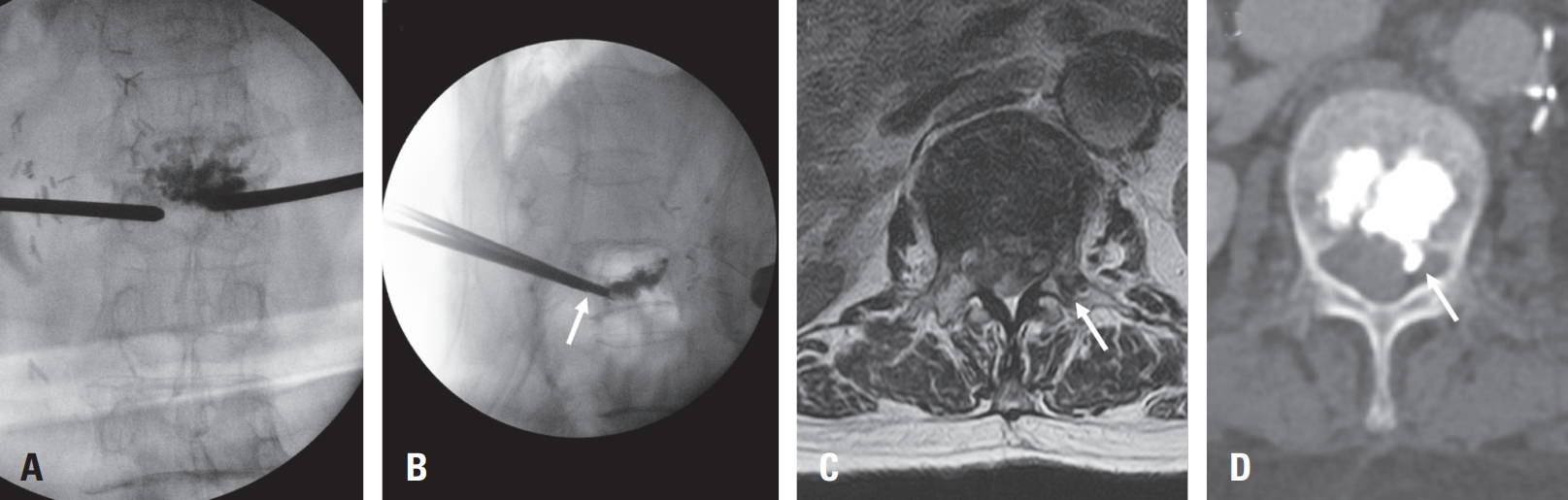
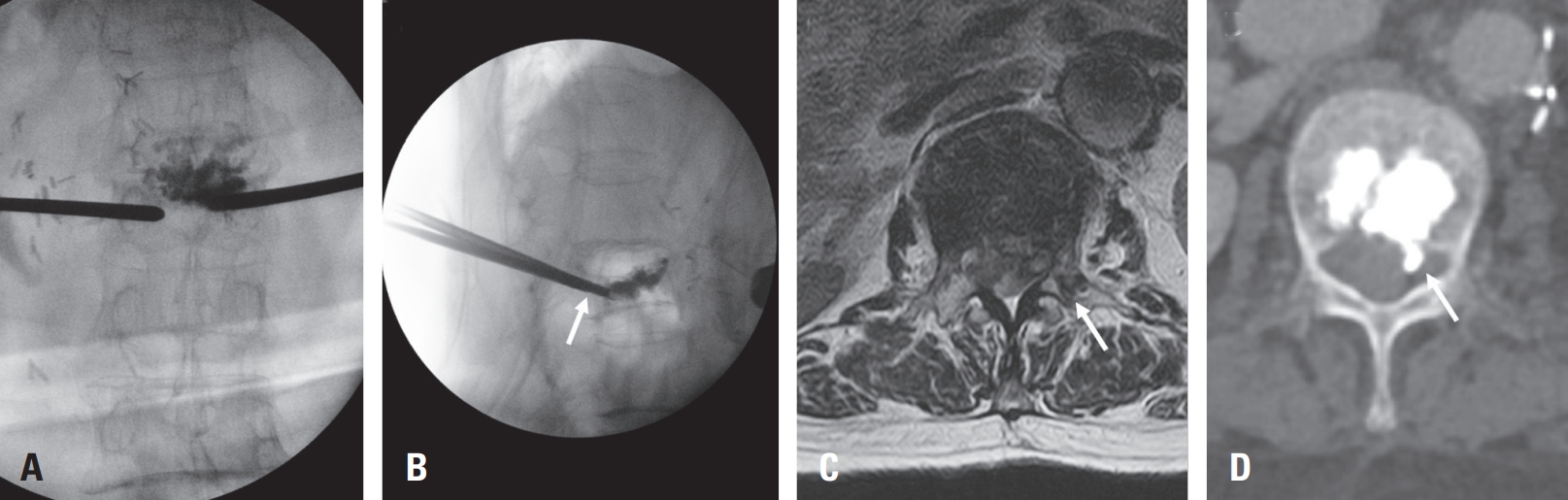
In our case, review of intraoperative fluoroscopic imaging revealed that during the left-sided needle insertion, the needle did not fully traverse the vertebral body in the lateral view, suggesting possible medial wall violation (Fig. 3A, B). Postoperative X-ray also demonstrated a very mild posterior cement leakage, which was initially overlooked due to its subtle appearance. On postoperative day 1 MRI, medial pedicle violation was suspected (Fig. 3C), and subsequent computed tomography performed after transfer to our institution demonstrated cement leakage into the spinal canal (Fig. 3D). These findings indicate that medial deviation of the needle, in combination with anticoagulation therapy (warfarin and enoxaparin), likely contributed to the development of the subdural hematoma.6,15)
Therefore, surgeons should take extra caution to avoid pedicle wall violations and should inject cement slowly and in a controlled manner, especially in osteoporotic spines where venous structures are more fragile.12) Preoperative imaging guidance and intraoperative fluoroscopy are crucial to maintaining procedural safety.
As far as we are aware, this may represent the first reported case of spinal subdural hematoma following kyphoplasty in a patient requiring chronic warfarin therapy due to a mechanical aortic valve. This case emphasizes the importance of maintaining a high index of suspicion for spinal hematoma in high-risk patients. Even subtle findings—such as minimal cement leakage on imaging or new-onset weakness and worsening back pain—should prompt consideration of spinal hematoma.17) In such cases, early MRI can facilitate timely diagnosis and guide appropriate management. While conservative treatment with corticosteroids and close observation may be sufficient in neurologically stable patients, surgical decompression remains the standard of care for those with progressive or severe deficits.
Conclusions
Spinal subdural hematoma is a rare but serious complication following kyphoplasty, especially in patients on anticoagulation therapy. Our case demonstrates that conservative management with corticosteroids and close monitoring can be a viable option in patients with mild and stable neurological symptoms.
This case also suggests the importance of individualized anticoagulation planning and technical precautions, including avoiding pedicle breach and injecting cement slowly to minimize venous pressure. Early detection through postoperative imaging may aid timely intervention. A multidisciplinary, risk-adapted strategy is essential to optimize outcomes in high-risk patients undergoing spinal augmentation.
Fig. 1.
(A–C) Sagittal and axial T2-weighted MR images and lateral radiograph demonstrating acute L2 compression fracture. (D) Postoperative lateral radiograph showing mild posterior cement leakage (white arrow) following kyphoplasty.
Fig. 2.
Serial postoperative MRI showing the evolution of spinal subdural hematoma. (A) POD 1: Subdural hematomas at L1–2 and L5–S1 levels with thecal sac compression. (B) POD 2: Cranial extension into the thoracic spine with increased spinal cord compression. (C) POD 4: No further thoracic progression, but a new subdural hematoma developed at L3–4. (D) POD 11: Partial resolution of the hematoma with mixed subdural and epidural components.
Fig. 3.
Imaging suggesting medial pedicle breach and cement leakage. (A, B) Intraoperative fluoroscopic images (AP and lateral views); the needle does not fully traverse the vertebral body in the lateral view (white arrow), suggesting possible medial wall violation. (C) Postoperative day 1 MRI showing suspected medial pedicle breach (white arrow). (D) Post-transfer CT confirming cement leakage into the spinal canal (white arrow).
Table 1.
Reported cases of spinal subdural hematoma following vertebroplasty or kyphoplasty
1. Jang HD, Kim EH, Lee JC, Choi SW, Kim HS, Cha JS, et al. Management of Osteoporotic Vertebral Fracture: Review Update 2022. Asian Spine J 2022;16:934-46.
2. Liu Y, Liu J, Suvithayasiri S, Han I, Kim JS. Comparative Efficacy of Surgical Interventions for Osteoporotic Vertebral Compression Fractures: A Systematic Review and Network Meta-analysis. Neurospine 2023;20:1142-58.
3. Nussbaum DA, Gailloud P, Murphy K. A review of complications associated with vertebroplasty and kyphoplasty as reported to the Food and Drug Administration medical device related web site. J Vasc Interv Radiol 2004;15:1185-92.
4. Cavka M, Delimar D, Rezan R, Zigman T, Duric KS, Cimic M, et al. Complications of Percutaneous Vertebroplasty: A Pictorial Review. Medicina (Kaunas) 2023;59.
5. Kaplan N, Akyuva Y, Guven G. A Rare and Unusual Complication of Kyphoplasty: A Case Report of Spinal Subdural Hemotoma. Journal of Academic Research in Medicine 2019;9:107-10.
6. Mrad I, El Houshiemy M, Kawtharani S, Shouman WA, Lakkis S, Darwish H. Delayed-onset spinal subdural hematoma after kyphoplasty. Surg Neurol Int 2025;16:197.
8. Panduranga P, Al-Mukhaini M, Al-Muslahi M, Haque MA, Shehab A. Management dilemmas in patients with mechanical heart valves and warfarin-induced major bleeding. World J Cardiol 2012;4:54-9.
10. Cosar M, Sasani M, Oktenoglu T, Kaner T, Ercelen O, Kose KC, et al. The major complications of transpedicular vertebroplasty. J Neurosurg Spine 2009;11:607-13.
11. Lee KD, Sim HB, Lyo IU, Kwon SC, Park JB. Delayed onset of spinal subdural hematoma after vertebroplasty for compression fracture: a case report. Korean J Spine 2012;9:285-8.
12. Mattei TA, Rehman AA, Dinh DH. Acute Spinal Subdural Hematoma after Vertebroplasty: A Case Report Emphasizing the Possible Etiologic Role of Venous Congestion. Global Spine J 2015;5:e52-8.
13. Tropeano MP, La Pira B, Pescatori L, Piccirilli M. Vertebroplasty and delayed subdural cauda equina hematoma: Review of literature and case report. World J Clin Cases 2017;5:333-9.
14. Wang X, Peng Y, Qiu J, Huang D. Spinal subdural and epidural hematomas after vertebroplasty for compression fracture: a case report. Spinal Cord Ser Cases 2018;4:87.
15. von der Brelie C, Fiss I, Rohde V. Multilevel Spinal Combined Subdural/Subarachnoid Hemorrhage Resulting in Paraplegia: An Unusual Complication of Kyphoplasty. J Neurol Surg A Cent Eur Neurosurg 2019;80:220-2.
16. Yang HC, Liu HW, Lin CM. Spinal subdural hematoma from a ventral dural puncture after percutaneous vertebroplasty: illustrative case. J Neurosurg Case Lessons 2022;3.
Spinal Subdural Hematoma After Kyphoplasty in a Patient on Warfarin: A Case Report and Literature Review
Fig. 1. (A–C) Sagittal and axial T2-weighted MR images and lateral radiograph demonstrating acute L2 compression fracture. (D) Postoperative lateral radiograph showing mild posterior cement leakage (white arrow) following kyphoplasty.
Fig. 2. Serial postoperative MRI showing the evolution of spinal subdural hematoma. (A) POD 1: Subdural hematomas at L1–2 and L5–S1 levels with thecal sac compression. (B) POD 2: Cranial extension into the thoracic spine with increased spinal cord compression. (C) POD 4: No further thoracic progression, but a new subdural hematoma developed at L3–4. (D) POD 11: Partial resolution of the hematoma with mixed subdural and epidural components.
Fig. 3. Imaging suggesting medial pedicle breach and cement leakage. (A, B) Intraoperative fluoroscopic images (AP and lateral views); the needle does not fully traverse the vertebral body in the lateral view (white arrow), suggesting possible medial wall violation. (C) Postoperative day 1 MRI showing suspected medial pedicle breach (white arrow). (D) Post-transfer CT confirming cement leakage into the spinal canal (white arrow).
Fig. 1.
Fig. 2.
Fig. 3.
Spinal Subdural Hematoma After Kyphoplasty in a Patient on Warfarin: A Case Report and Literature Review