Purpose This retrospective study investigated the distinct clinical and radiographic drivers of early- versus late-onset proximal junctional kyphosis (PJK) following multilevel thoracolumbar (TL) fusion.
Methods After applying the exclusion criteria (spinal infection, neuromuscular disease, age <50 years), the analysis included 136 patients who underwent ≥4-level TL fusion and were followed up for a minimum of 2 years. PJK was classified as early (≤6 months) or late (>6 months) onset. Patient-related factors, surgical variables, sagittal spinopelvic parameters, and preoperative magnetic resonance imaging findings were analyzed using multivariate logistic regression to identify independent predictors of early PJK.
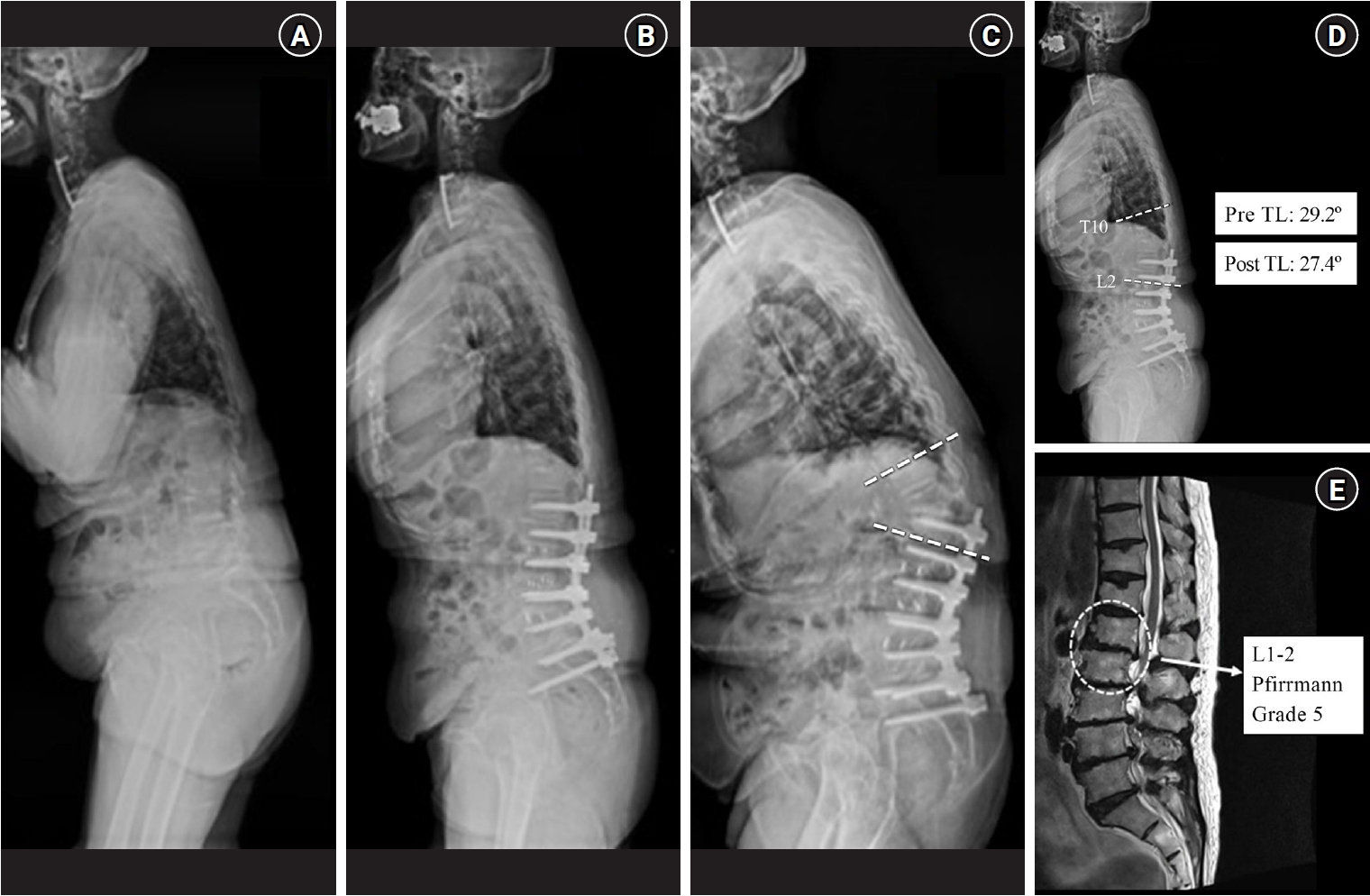
Results Among 24 patients (17.6%) who developed PJK, the early and late-onset groups included 13 and 11 patients, respectively. The early PJK group exhibited significantly greater preoperative and postoperative TL angles compared with the late group (preoperative: 23.03±13.83° vs. 9.67±9.67°, p=0.024; postoperative: 19.6±6.95° vs. 6.95±6.35°, p<0.001). The Pfirrmann grade of the L1–2 intervertebral disc was significantly higher in the early PJK group (3.92±0.95 vs. 2.81±0.60, p=0.006). No surgical variables differed significantly between the groups. Multivariate analysis confirmed greater postoperative TL angle and more advanced L1–2 disc degeneration as independent predictors of early PJK.
Conclusion Early-onset PJK following multilevel TL fusion is primarily driven by regional biomechanical vulnerabilities, specifically residual postoperative TL kyphosis and advanced adjacent L1–2 disc degeneration, rather than by surgical variables. Meticulous evaluation of regional TL alignment and adjacent disc health during surgical planning is critical for risk stratification and prevention of early junctional failure.
Purpose This study was conducted to identify risk factors predicting the loss of cervical lordosis (LCL) in patients with multilevel ossification of the posterior longitudinal ligament (OPLL) following laminoplasty.
Material and Methods: We conducted a retrospective analysis of data from patients who underwent laminoplasty at Chonnam National University Hospital between January 2013 and December 2022. Various radiological parameters and clinical outcome measures were collected perioperatively. Patients were divided into 2 groups according to the severity of LCL. We examined preoperative radiological parameters associated with LCL.
Results We analyzed data from 109 patients (92 men and 17 women; mean age, 60.31±10.80 years). A higher T1 slope (odds ratio [OR], 1.420; p<0.001) and a lower extension ratio (OR, 0.883; p=0.019) were associated with a higher risk of LCL. T1 slope was shown to be an excellent predictor of LCL, with a cut-off value of 28° (p<0.001, area under the curve=0.918). Also, The T1 slope and extension ratio were statistically significant correlated with clinical outcomes.
Conclusions T1 slope and extension ratio were significantly associated with LCL in patients with multilevel OPLL following laminoplasty. The cut-off value for the T1 slope was 28°, and the cut-off value for the extension ratio was 33. Therefore, in multilevel OPLL patients with a T1 slope exceeding 28° or an extension ratio below 33, a warning regarding the potential LCL should be given before performing cervical laminoplasty.
After posterior cervical arthrodesis, many problems can arise, including adjacent segment degeneration and the related adjacent segment disease (ASD). As indicated by studies on the causes of ASD, posterior cervical arthrodesis can produce biomechanical and kinematic changes in adjacent unfused segments due to inappropriate forces.
Several studies have been conducted to determine the appropriate lowest instrumented vertebra, specifically regarding whether to cross the cervicothoracic junction via extension of long-segment posterior cervical fusion. We searched for relevant articles in electronic databases including PubMed, the Cochrane Registry, Embase, and Ovid.
Five meta-analyses were reviewed on this topic. Among these, Goyal et al. (2019), Rajjoub et al. (2022), and Chang et al. (2022) argued that ending instrumentation at the cervical level was associated with higher rates of ASD and reoperation. However, Truumees et al. (2022) and Coban et al. (2022) found no statistically significant differences between cases of instrumentation ending at the cervical and thoracic levels in the rates of ASD and requirement of revision surgery. Cervicothoracic junction breakage is a known possibility after cervical spine surgery because of the anatomical fragility of the junction. Terminating at the thoracic level reduces the stress on the cervicothoracic junction, thereby decreasing complications such as cervicothoracic junction breakage and lowering the frequency of reoperation. Based on the findings published to date, instrumentation across the cervicothoracic junction can be reasonably recommended in cases of multilevel posterior cervical fusion based on the lower reoperation and higher fusion rate.
Background Proximal junctional kyphosis (PJK) following long instrumented fusion is a well-recognized complication that does not negatively affect the clinical outcomes. However, there were few studies with regard to the long-term consequences of PJK.
Objective: To investigate the long-term clinical and radiographic consequences of proximal junctional kyphosis (PJK) following the long instrumented fusion for elderly patients with sagittal imbalance.
Methods Patients older than 60 years who underwent ≥4 fusion including the sacrum for sagittal imbalance were followed up longer than five years. PJK was defined as proximal junctional angle (PJA) >10° without any bony compromise or myelopathy. The radiographic and clinical outcomes were compared between PJK and non-PJK groups. Clinical outcome measures included visual analog scale (VAS) for back and leg, Oswestry disability index (ODI), and Scoliosis Research Society (SRS)-22 scores.
Results A mean age was 69.2 years. An average follow-up duration was 92.4 months. There were 30 patients in PJK group and 43 in non-PJK group. At the final follow-up, pelvic incidence-lumbar lordosis mismatch, pelvic tilt, and sacral vertical axis were not different between the two groups. In PJK group, PJA significantly increased from 6.5° postoperatively to 21.2° at the final follow-up. At the final follow-up, clinical outcomes were worse in PJK group than in non-PJK group with regard to VAS for back, ODI, and SRS-22 scores except satisfaction domain. Three (10%) of 30 patients underwent a revision surgery for PJK progression.
Conclusions PJK progressed with time and negatively affect the clinical outcomes in a long-term follow-up after ASD surgery.
Purpose The purpose of this review is the current understanding of proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) following adult spinal deformity (ASD) surgery.
Materials and Methods We carried out a systematic search of PubMed for literatures published up to September 2016 with “proximal junctional kyphosis” and “proximal junctional failure” as search terms. A total of 57 literatures were searched.
Finally, the 33 articles were included in this review.
Result PJK and PJF are recognized complications after long instrumented posterior fusion in ASD surgery. PJK is multifactorial in origin and likely results from surgical, radiographic, and patient related risk factors. PJF is a progressive form of the PJK spectrum including bony fracture of uppermost instrumented vertebra (UIV) or UIV+1, subluxation between UIV and UIV+1, failure of fixation, neurological deficit, which may require revision surgery for proximal extension of fusion.
Variable risk factors for PJK and PJF have been investigated, and they can be categorized into surgical, radiographic, and patient-related factors. There are several strategies to minimize PJK and PJF. Soft tissue protections, adequate selection of the UIV, prophylactic rib fixation, hybrid instrumentation such as hooks, vertebral cement augmentation at UIV and UIV+1, and age-appropriate spinopelvic alignment goals are worth consideration.
Conclusion The ability to perform aggressive global realignment of spinal deformities has also led to the discovery of new complications such as PJK and PJF. Continuous research on PJK and PJF should be proceeded in order to comprehend the pathophysiology of these complications.

 First
First Prev
Prev

