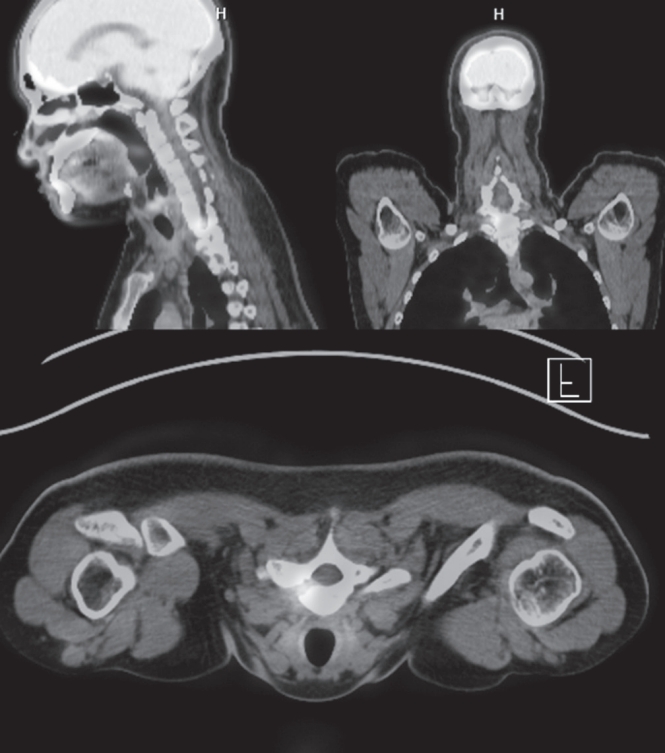
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
The standard method for treating posterior pelvic ring injuries involves sacroiliac joint cannulated lag screw fixation, necessitating repeated fluoroscopy and leading to radiation exposure. The O-arm navigation system, designed for spine screw fixation, is applied in pelvic injuries to enhance precision. A successful case involved a 39-year-old male with a complex pelvic injury, where sacroiliac screw fixation was performed in the prone position using the O-arm guide. The patient, injured at a construction site, showed fractures and widening of the symphysis pubis and right sacroiliac joint. Surgery was planned for both lumbar and pelvic regions due to an L3 burst fracture. The O-arm system demonstrated efficacy in precise screw placement, reducing surgical duration, and minimizing complications. The discussion emphasizes early pelvic fixation benefits, with percutaneous iliosacral screws standing out. Conventional fluoroscopy-guided methods pose challenges, and the O-arm system proves advantageous, especially for less experienced surgeons. Future advancements may enable pelvic surgery using the O-arm without C-arm guidance if instrumentation for pelvis fixation is developed.

 First
First Prev
Prev

