Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
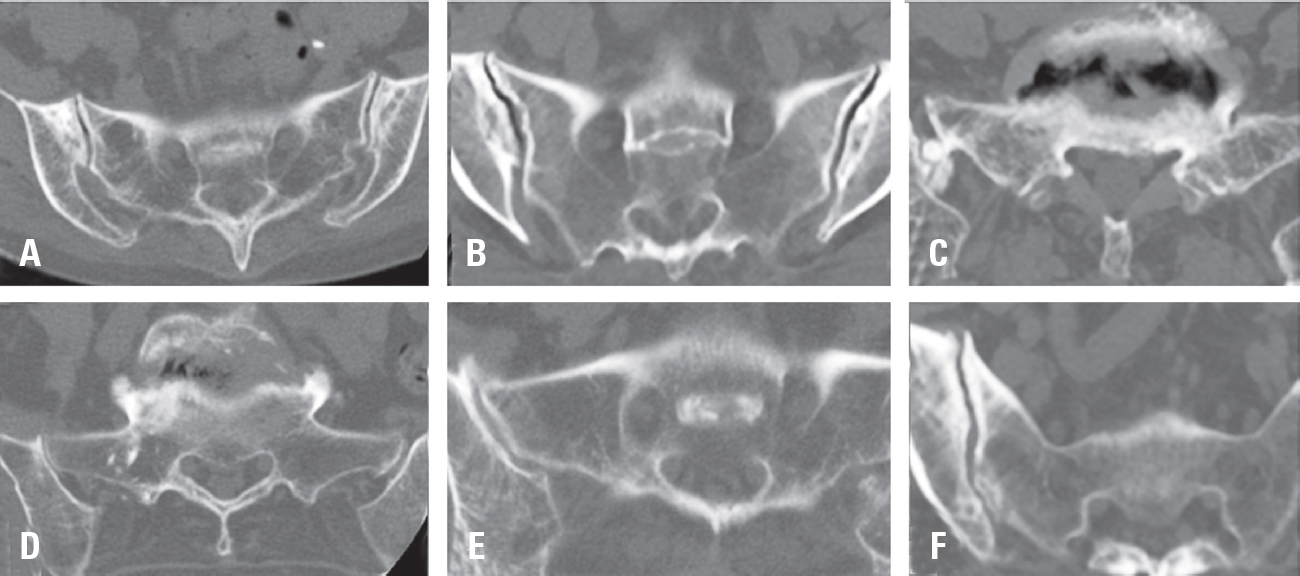
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Objective Proximal junctional fracture (PJFx) at the uppermost instrumented vertebra (UIV) or UIV+1 is the most common mechanism of PJF. There are few studies assessing the radiographic progression after PJFx development.
Therefore, this study sought to identify the risk factors for radiographic progression of PJFx in surgical treatment for ASD.
Methods In this retrospective study, among 317 patients aged > 60 years who underwent ≥5-level fusion from the sacrum, 76 with PJFx development were included. According to the change in proximal junctional angle (PJA), two groups were created: Group P (change ≥10°) and Group NP (change <10°). Patient, surgical, and radiographic variables were compared between the groups to demonstrate risk factors for PJFx progression using uni- and multivariate analysis. The receiver operating characteristic (ROC) curve was used to calculate cutoff values. Clinical outcomes, such as visual analog scale (VAS) scores for back and leg pain, the Oswestry Disability Index (ODI) score, and the Scoliosis Research Society (SRS)-22 score, and revision rate were compared between the two groups.
Results The mean age at the index surgery was 71.1 years, and there were 67 women enrolled in the study (88.2%).
There were 45 patients in Group P and 31 in Group NP. A mean increase of PJA was 15.6° (from 23.2° to 38.8°) in Group P and 3.7° (from 17.2° to 20.9°) in Group NP. The clinical outcomes were significantly better in Group NP than Group P, including back VAS score, ODI value, and the SRS-22 scores for all items. Revision rate was significantly greater in group P than in group NP (17.8% vs. 51.6%, p=0.001). Multivariate analysis revealed that overcorrection relative to the age-adjusted ideal pelvic incidence (PI)–lumbar lordosis (LL) target at the index surgery (odds ratio [OR]=4.484, p=0.030], PJA at the time of PJFx identification (OR=1.097, p=0.009), fracture at UIV versus UIV+1 (OR =3.410, p=0.027) were significant risk factors for PJFx progression. The cutoff value of PJA for PJFx progression was calculated as 21° using the ROC curve.
Conclusions The risk factors for further progression of PJFx were overcorrection relative to age-adjusted PI–LL target at the index surgery, PJA > 21° at initial presentation, and fracture at the UIV level. Close monitoring is warranted for such patients not to miss the timely revision surgery.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Cervical ossification of posterior longitudinal ligament (OPLL) can cause cord compression which can lead to myelopathy. Operative management including anterior fusion or laminoplasty is needed in these cases.
Understanding the progression course of OPLL, risk factors of progression, and risk factors of myelopathy caused by OPLL is essential to determine the necessity, timing and method of operation. Therefore, we will review the previous study results regarding characteristics and progression course of OPLL. Furthermore, the results of study about risk factors and progression course of OPLL undergoing conservative management will be discussed.

 First
First Prev
Prev

