1)Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea
2)Department of Orthopaedic Surgery, Ewha Womans University College of Medicine, Seoul, Korea
Corresponding author: Ji-Won Kwon, M.D., Ph.D. Department of Orthopaedic Surgery, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul, 03722, Korea TEL: +82-2-2019-3411, FAX: +82-2-2019-3410 E-mail: kwonjjanng@yuhs.ac
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
Materials and Methods
This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results
Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions
Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
천장관절(SI) 퇴행은 요천추 유합 수술 후 발생할 수 있는 흔한 합병증 중 하나이다. 이 퇴행은 유합된 수준의 수, 골반이나 천골의 관여, 그리고 sagittal 정렬 변화 등 여러 가지 요인과 관련이 있을 수 있다. 본 연구는 SI 관절 퇴행의 진행에 영향을 미치는 위험 요인과 척추-골반 파라미터 변화들을 규명하는 것을 목표로 하며, 이러한 요인들이 SI 관절 퇴행에 미치는 영향을 분석하고자 했다.
대상 및 방법
본 연구는 2021년 3월부터 2024년 2월까지 세개의 병원에서 유합 수술을 받은 472명의 환자를 대상으로 한 다기관 후향적 연구이다. SI 관절 퇴행은 7가지 주요 지표(경화 변화, 침식, 골극 형성, 관절 내 뼈 형성, 관절 공간 협소, 관절 내 가스 형성, 하연 낭종)를 통해 평가했다. 수술 전과 6개월 후에 각각 CT 촬영을 진행하여, 각 측면에 대해 총 14점 만점을 기준으로 점수를 계산하였으며, 수술 전후 2점 이상의 차이를 보일 경우 이를 SI 관절 퇴행으로 정의했다. 환자들은 SI 관절 퇴행이 진행된 그룹과 그렇지 않은 그룹으로 나누어졌다. 또한, 수술 전과 수술 후 6개월에 서 있는 상태에서 촬영한 전체 척추 측면 X선 영상을 사용하여 10개의 척추-골반 파라미터(T1PA, GT, PT, SS, PI, LL, TK, TLK, SVA, PI-LL)를 측정했다. 통계 분석에는 두 샘플 t-검정과 다변량 로지스틱 회귀 분석을 사용했다.
결과
472명의 환자 중 135명(28.6%)이 SI 관절 퇴행이 진행된 것으로 나타났다. 두 그룹을 비교한 결과, 나이(p=0.022), 음주(p=0.001), 흡연(p<0.001), 그리고 S1 관여(p=.04)가 SI 관절 퇴행과 유의미한 연관이 있음을 확인했다. 척추-골반 파라미터 측면에서, SI 관절 퇴행이 진행된 환자들은 흉추 후만(p=.017)과 골반 기울기(p=.049)에서 유의미한 변화를 보였으며, 이는 골반의 전후 기울기에 따른 SI 관절의 뉴테이션 및 카운터뉴테이션 운동의 변화와 관련이 있을 수 있다.
결론
천골 고정, 흡연, 음주, 나이는 요천추 융합 수술 후 SI 관절 퇴행의 중요한 위험 요인이 될 수 있으며, 이러한 요인들을 미리 파악하고 관리하는 것이 수술 후 SI 관절 퇴행을 예방하는 데 중요한 역할을 할 수 있습니다. 또한, 척추-골반 파라미터에서 흉추 후만과 골반 기울기의 변화는 SI 관절 퇴행과 밀접한 관계가 있음을 시사합니다.
Degenerative changes in the lumbar spine, including recurrent disc herniation, facet joint degeneration, spinal stenosis, and spondylolisthesis, have become increasingly prevalent in the aging population. These degenerative conditions often lead to chronic pain and functional impairment, particularly in patients over 50 years of age. When conservative treatments such as physical therapy, medication, or injections fail to alleviate symptoms, surgical interventions such as posterior decompression and lumbar fusion become wellestablished treatment options. However, while lumbar fusion aims to restore stability and improve function by fusing the vertebrae, it also introduces new challenges and potential complications, including the development of degenerative changes in adjacent segments. These adjacent segment diseases (ASD) are of increasing clinical concern and have prompted considerable research to better understand their underlying mechanisms, risk factors, and potential treatment strategies.1-4) Lumbar fusion, by its very nature, alters the biomechanics of the lumbopelvic region. By immobiliz-ing the lumbar segments, fusion surgery inevitably increases mechanical stress on the adjacent levels, which can accelerate the degenerative process. These changes often manifest in the form of disc degeneration, facet joint osteoarthritis, or spinal stenosis in the segments adjacent to the fusion site. Studies have shown that fusion can alter the natural range of motion and load distribution across the spine, leading to increased stress at the adjacent segments, which in turn may contribute to further degeneration.2,5-7) At the base of the spine, the sacroiliac joint (SIJ) plays a critical role in force transmission between the upper body and the lower extremities. As the lowest component of the spinal axis, the SIJ is integral in absorbing and distributing the mechanical loads that are transferred through the spine. Although the SIJ has approximately six times greater resistance to lateral flexion than the lumbar spine, it is significantly weaker when subjected to axial forces and rotational stress, with resistance levels of only 1/12 and 1/2, respectively, compared to the lumbar spine. Despite its primary function of contributing to stability rather than mobility, the SIJ still permits small but essential movements, including approximately 4° of rotational motion and 1.6 mm of translational motion. These movements are crucial for shock absorption and the distribution of forces during activities such as walking and lifting.3,6,8) The small but critical movements of nutation and counternutation of the sacrum are essential for maintaining the proper function of the SIJ. Nutation refers to the forward tilting of the sacrum in relation to the ilium, while counternutation is the opposite motion, where the sacrum tilts backward. These movements allow for the accommodation of changes in load distribution across the pelvis and spine. However, when lumbar fusion is performed, particularly when sacral fixation is involved, the natural motion of the SIJ may be disrupted. The abnormal concentration of mechanical stress in the SIJ due to altered lumbopelvic kinematics can contribute to degeneration of the joint over time.4,9,10)
Although SIJ degeneration was once considered less significant than degeneration in the proximal adjacent segments of the lumbar spine, its clinical impact has become increasingly recognized in recent years. Studies now indicate that approximately 15% of patients with chronic low back pain also report concomitant hip pain, which is often attributed to dysfunction in the SIJ. This highlights the relevance of SIJ health in post-fusion outcomes. The increasing recognition of SIJ degeneration emphasizes the need for a comprehensive understanding of its risk factors and its potential to affect long-term outcomes following lumbar fusion surgery. Recent research suggests that several factors contribute to the development of SIJ degeneration, particularly after lumbar or lumbosacral fusion. These factors include the type of fusion procedure (such as posterior or anterior fusion), the number of vertebral levels fused, the preoperative condition of adjacent spinal segments, and the overall sagittal alignment of the lumbar spine. These elements can influence the mechanical stress placed on the SIJ and contribute to its degenerative process. Additionally, preoperative assessment of SIJ integrity and alignment may provide valuable insight into which patients are at greater risk for developing SIJ degeneration post-surgery.6,11)
1. Objective
This study aims to compare the spino-pelvic radiographic parameters between patients who underwent lumbar and lumbosacral fusion and developed postoperative degenerative changes in the sacroiliac joint (SIJ) and those who did not. Additionally, the study seeks to identify the risk factors associated with SIJ degeneration following lumbosacral fusion surgery.
Materials and Methods
1. Study data
This study included patients diagnosed with lumbar degenerative spinal diseases, such as recurrent disc herniation, spinal stenosis, disc degeneration, and spondylolisthesis, between January 1, 2019, and February 28, 2024. These patients underwent posterior decompression and lumbar or lumbosacral fusion due to persistent symptoms despite conservative treatments.
Patients who lacked preoperative MRI or CT scans of the lumbar spine, those with poor imaging quality that rendered analysis impossible, patients who underwent reoperation, and those who received surgical treatment due to infection or trauma were excluded from the study.
As a result, a retrospective analysis was conducted based on the medical records of 548 patients. Of these, 52 patients were excluded due to failure to attend outpatient followup visits, and 24 patients were excluded due to reoperation or follow-up failure related to trauma, metastatic cancer, or infection. Therefore, the final analysis included 472 patients.
2. Radiological criteria and diagnosis of sacroiliac joint degeneration
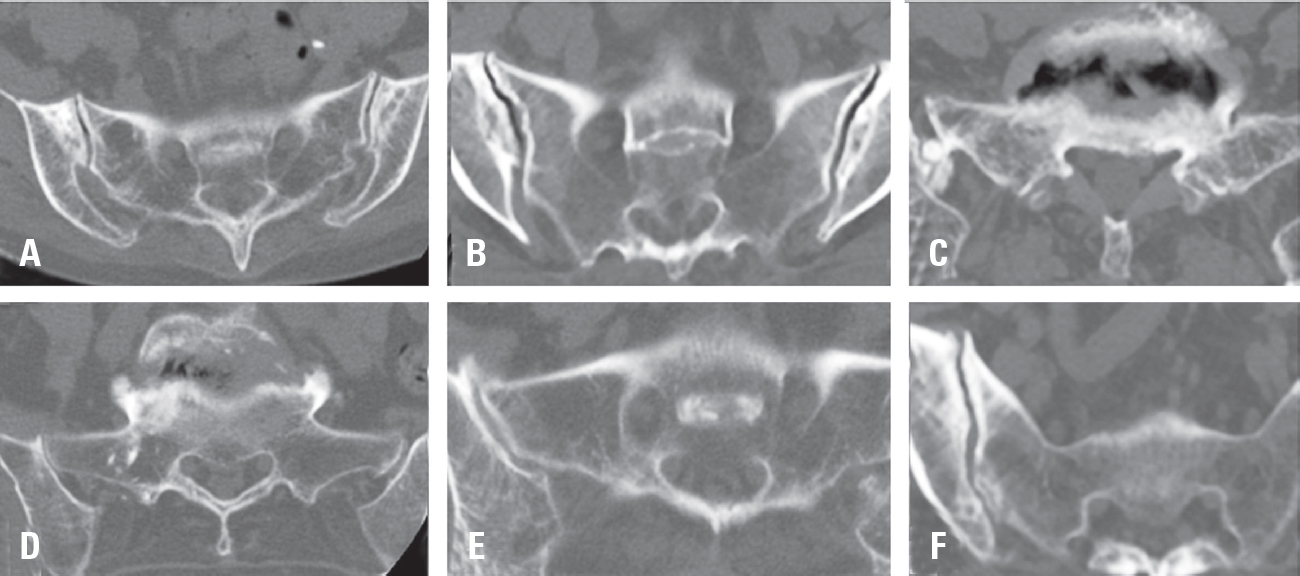
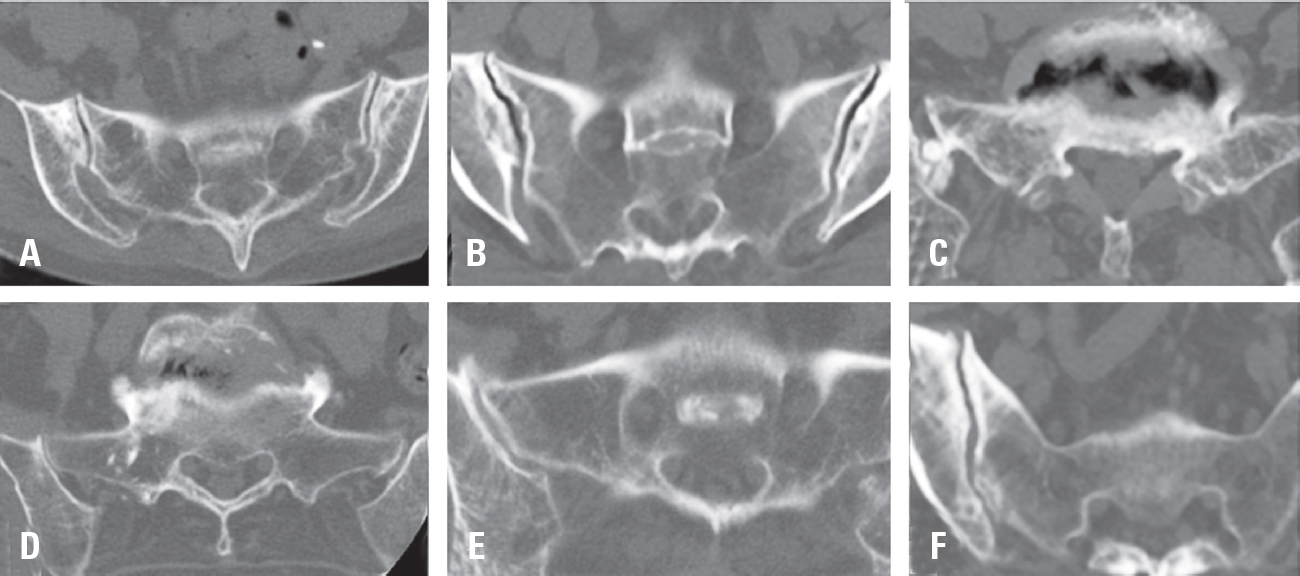
CT scans were performed both preoperatively and 6 months postoperatively to evaluate radiological changes in the sacroiliac joint. The relatively short follow-up period minimized the potential bias from age-related degenerative changes. The radiological assessment of degenerative changes in the sacroiliac joint was based on seven factors: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts (Fig. 1). Postoperative degeneration of the sacroiliac joint was diagnosed if one or more of these CT findings were present. Each of the seven factors was assigned a score: 1 point for unilateral presence, 2 points for bilateral presence, and 0 points for absence. The total score, which could range up to 14 points, was treated as a continuous variable. If the change in the continuous score was 2 points or more at the 6-month CT scan, the patient was diagnosed with postoperative sacroiliac joint degeneration.12-17)
The criteria for radiographic degenerative factors are as follows12-15):
Sclerotic Changes: Sclerotic change in the ilium ≥5 mm, and in the sacrum ≥3 mm.
Erosion: Lysis of subchondral bone >3 mm in the ilium or sacrum.
Osteophyte Formation: Extra-articular bony fragments crossing or forming within the SIJ space.
Joint Space Narrowing: The shortest distance of the SIJ <2 mm.
CT images were analyzed using Centricity (Enterprise Web ver. 3.0; GE Healthcare, Chicago, Illinois, USA). Based on these criteria, the degeneration group and the non-degeneration group were compared in terms of demographic data, surgery-related factors, and spinopelvic radiologic parameters.
3. Radiological parameter definitions
The entire spinal sagittal alignment was assessed using 36-inch lateral radiographs, both preoperatively and 3 months postoperatively. The measured parameters included the sagittal vertical axis (SVA), thoracic kyphosis (TK), thoracolumbar kyphosis (TLK), lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), sacral slope (SS), global tilt (GT), PI-LL, and T1 pelvic angle (T1PA).
• SVA was defined as the distance between the C7 plumb line and the posterior-superior corner of the sacrum.
• LL was measured between the upper endplate of L1 and the upper endplate of S1.
• TK was measured between the upper endplate of T5 and the lower endplate of T12.
• TLK was measured between the upper endplate of T10 and the lower endplate of L2.
• T1PA was defined as the angle between the line from the center of the femoral head to the center of the T1 vertebral body and the line from the center of the femoral head to the center of the sacral endplate.
• GT was the angle formed by the line from the center of the sacral endplate to the center of the C7 vertebral body and the line from the center of the femoral head to the center of the sacral endplate.18,19)
Radiographic fusion was assessed using the grading system described by Bridwell et al., based on anteroposterior radiographs obtained with flexion and extension. Grade I indicates complete fusion, with trabecular integration and remodeling observed. Grade II shows an intact graft without any radiolucent areas. Grade III reveals radiolucency around the graft. Finally, Grade IV indicates nonunion, characterized by graft resorption and collapse.20)
4. Statistical analysis
Data analysis was performed using SPSS version 23 (IBM Corp., Armonk, NY). Data were expressed as mean±standard error or percentages. Differences in continuous and categorical variables between subgroups were analyzed using Student’s t-tests and chi-square tests. Multivariable Logistic regression analysis was performed to assess the risk factors for the development of sacroiliac joint degeneration after lumbar or lumbosacral fusion. A p-value of <0.05 was considered statistically significant.
Results
Among the 472 patients, 225 (47.66%) underwent singlelevel surgery, 166 (35.16%) had two-level surgery, and 81 (17.16%) underwent three or more levels of fusion. The number of patients who underwent OLIF (Oblique Lateral Interbody Fusion) was 66 (13.98%) (Table 1). Of the 472 patients, 337 (71.39%) developed sacroiliac joint (SIJ) degeneration postoperatively, while 135 (28.60%) did not (Table 2). A detailed analysis of demographic data between the degeneration and non-degeneration groups revealed no significant differences in gender, BMI, or BMD T-score. These results suggest that the development of SIJ degeneration may not be strongly influenced by basic demographic factors such as sex or body mass index, nor by bone mineral density. Regarding surgery-related data, no significant differences were found in terms of surgery duration, intraoperative blood loss, the approach used, or the number of fused segments between the two groups. These factors, typically considered key surgical variables, did not show a clear association with SIJ degeneration. However, when analyzing the spinopelvic parameters, none of the preoperative measurements showed significant differences between the degeneration and non-degeneration groups. In contrast, a significant difference was found in the percentage of patients who underwent sacrum fixation. Specifically, 44.23% of patients in the sacrum-fixed group developed SIJ degeneration, compared to 34.49% in the non-fixed group, with a p-value of 0.04. This suggests that sacral fixation may play a role in the development of SIJ degeneration postoperatively. Moreover, there were significant differences in lifestyle factors, including alcohol consumption (p=0.001), smoking status (p<0.001), and age (p=0.022), between the degeneration and non-degeneration groups (Table 3). These factors may represent important modifiable risk factors influencing the progression of SIJ degeneration after lumbar fusion.
Interestingly, there was no significant difference in fusion grade between the two groups when evaluated on radiographs taken six months postoperatively. The average Bridwell fusion grade was 1.71±0.71 in the degeneration group and 1.72±0.81 in the non-degeneration group (p=0.872), indicating that the quality of fusion did not significantly differ between patients who developed SIJ degeneration and those who did not. Radiological analysis of post-surgical spinopelvic parameters showed significant differences in pelvic tilt (p=0.049) and thoracic kyphosis (p=0.017). Specifically, the degeneration group exhibited a higher pelvic tilt (6.33±6.85) compared to the non-degeneration group (5.22±5.08), and a higher thoracic kyphosis (8.45±8.42 vs 6.76±6.60) (Table 4). These findings suggest that changes in spinopelvic alignment, particularly in pelvic tilt and thoracic kyphosis, are associated with the development of SIJ degeneration after lumbar fusion. These changes could reflect compensatory adjustments in posture and spinal alignment in response to altered biomechanical forces following fusion surgery. No significant differences were observed in clinical outcomes such as back pain, leg pain, Oswestry Disability Index (ODI), and EQ-5D scores between the degeneration and non-degeneration groups (Table 5). This indicates that, despite the radiological evidence of SIJ degeneration, there was no substantial impact on clinical symptoms or functional outcomes at the 6-month follow-up.
Discussion
The sacroiliac joint (SIJ) plays a crucial role in distributing loads applied to the body. Its unique L-shaped articular surface and the thick surrounding ligaments primarily contribute to the joint’s stability, enabling it to absorb and transmit forces between the upper body and the lower extremities. However, these anatomical features, while essential for stability, also make it challenging to detect degenerative changes through physical examination alone. As such, early detection and accurate diagnosis of SIJ degeneration are vital for managing postoperative outcomes. CT imaging is indispensable in this regard, providing clear visualization of radiographic features such as subchondral sclerosis, erosions, osteophyte formation, intra-articular loose bodies, joint space narrowing, intra-articular gas formation, and subchondral cysts. These features are indicative of degenerative changes and can be assessed with high accuracy using advanced imaging techniques.3,12,14,15,21)
This study aimed to identify risk factors associated with SIJ degeneration following lumbar fusion surgery. One of the key findings of this study was the significant association between sacrum fixation and SIJ degeneration. Specifically, patients who underwent fusion surgery involving sacral fixation showed a higher prevalence of SIJ degeneration. This suggests that the use of instrumentation extending to the sacrum may alter the biomechanics of the lumbopelvic region, potentially increasing mechanical stress on the SIJ and accelerating degenerative changes. These results are consistent with previous studies, which have shown that distal fixation, especially extending to the sacrum, alters the lumbopelvic motion and increases shear forces at the SI joint, contributing to its degeneration over time.2,6,7) The biomechanical changes resulting from sacral fixation can significantly affect the natural movement of the SIJ, such as nutation and counternutation, which are crucial for shock absorption and load distribution. When these movements are impaired due to surgical intervention, it could lead to the progressive degeneration of the SIJ.
A major strength of this study lies in its relatively large sample size, which increases the reliability of the findings and provides a more comprehensive understanding of the relationship between sacral fixation and SIJ degeneration. Larger sample sizes generally offer more statistical power, allowing for more robust conclusions and better generalizability of the results. The significant association between sacrum fixation and SIJ degeneration, along with the additional consideration of other risk factors, contributes valuable insights to the clinical management of patients undergoing lumbar fusion surgery. In addition to surgical factors, lifestyle factors such as alcohol consumption and smoking were also found to be significantly associated with SIJ degeneration. This finding is consistent with prior research that has demonstrated the impact of these factors on the progression of degenerative conditions, including spondyloarthritis. Smoking and alcohol consumption are known to contribute to systemic inflammation and alter bone metabolism, which can accelerate degenerative changes in joints, including the SIJ. These lifestyle factors are potentially modifiable, and their influence on post-surgical outcomes underscores the importance of perioperative counseling. Encouraging patients to modify their lifestyle, particularly by reducing alcohol intake and quitting smoking, may help mitigate the risk of SIJ degeneration following lumbar fusion surgery.22,23) Given that these factors can often be controlled through patient education and behavioral changes, they offer a practical avenue for improving patient outcomes in clinical practice. Age was another significant factor associated with SIJ degeneration, with older patients exhibiting a higher prevalence of degeneration. This is consistent with the natural progression of degenerative changes that occur with aging, which can be accelerated by surgical interventions like lumbar fusion. The findings suggest that older patients are at an increased risk of developing SIJ-related complications following lumbar fusion. This age-related susceptibility may be attributed to the decreased regenerative capacity of the joints in older individuals, as well as the cumulative effects of prior degenerative changes in the spine and pelvis.5,24) As the aging population continues to grow, understanding the impact of age on postoperative outcomes becomes even more crucial. Surgeons should be particularly cautious when performing lumbar fusion in elderly patients, taking into account their increased risk for adjacent segment degeneration, including SIJ degeneration. Overall, this study highlights the complex interplay between surgical factors, lifestyle choices, and age in the development of SIJ degeneration following lumbar fusion surgery. The findings suggest that a multifactorial approach is needed to address this complication. Tailoring surgical approaches based on individual patient factors, along with proactive lifestyle interventions, could help minimize the risk of SIJ degeneration and improve long-term outcomes for patients undergoing lumbar fusion.
Sexual dimorphism in sacroiliac joint (SIJ) anatomy and biomechanics has been well-documented. Generally, women tend to exhibit a wider and less curved pelvis, a more posteriorly tilted sacrum, and greater SIJ mobility compared to men. These anatomical differences have been implicated in an increased susceptibility to SIJ dysfunction and pain. For instance, the greater SIJ mobility in women is thought to contribute to higher stress concentrations in the joint, making it more prone to degenerative changes under certain conditions. However, despite these inherent anatomical and biomechanical distinctions, our study found no significant sex-based differences in SIJ degeneration following lumbosacral fusion surgery. This suggests that while sexual dimorphism plays a role in the baseline structure and function of the SIJ, pre-existing anatomical variations may have a diminished influence when the biomechanics of the entire lumbopelvic region are altered due to underlying pathology that necessitates surgical intervention. Specifically, the structural changes induced by lumbar fusion, such as altered load transmission and restricted sacral mobility, may override baseline sex-related differences, resulting in a comparable risk of SIJ degeneration in both sexes.25-27) This highlights the importance of considering the overall spinopelvic alignment rather than just anatomical differences when evaluating the risk of SIJ degeneration following surgery.
Spinopelvic radiographic parameters offer critical insights into sagittal alignment and its relationship with pelvic mechanics, both of which are essential for efficient load distribution during normal activities. In this study, radiological analysis revealed significant postoperative differences in pelvic tilt (PT) and thoracic kyphosis (TK) between the degeneration and non-degeneration groups. These differences suggest that changes in spinopelvic alignment may play a role in the development of SIJ degeneration following lumbar fusion[28]. Greater changes in PT in the degeneration group may indicate compensatory pelvic retroversion, which could arise as an adaptive response to altered load transmission through the sacrum and pelvis due to the fusion. Pelvic retroversion can help offset changes in spinal balance but may also increase stress on the SIJ, contributing to its degeneration over time. Furthermore, a reduction in sacral mobility due to SIJ degeneration could lead to secondary alterations in sagittal balance, which would further contribute to the degenerative process by disturbing the natural load distribution. Similarly, the differences in TK observed between the two groups may reflect compensatory adjustments in overall spinal alignment following lumbar fusion. These adjustments, while necessary for maintaining balance, may affect SIJ biomechanics, further exacerbating degeneration.18,19,29)
From a biomechanical perspective, the role of sacroiliac joint (SIJ) nutation and counternutation in degeneration must also be considered. Nutation, the forward tilting of the sacrum relative to the ilium, is essential for maintaining lumbopelvic stability during weight-bearing activities. It helps in the distribution of forces across the pelvis and spine, contributing to shock absorption and maintaining the normal posture of the lumbopelvic complex. In contrast, counternutation, the opposite motion, involves the backward tilt of the sacrum, which provides the necessary movement and flexibility for proper pelvic and spinal function. Both movements are crucial for mitigating mechanical stress on the SIJ and ensuring optimal spinal alignment and function.30) When fusion surgery involves S1, it may restrict the natural nutation-counternutation mechanism of the sacrum. By immobilizing the sacrum, fusion alters its ability to adapt to changes in mechanical loading, resulting in increased stress on the SIJ. This increased mechanical load may lead to the accelerated degeneration of the SIJ. Specifically, the postoperative increase in pelvic tilt (PT) observed in the SIJ degeneration group may reflect a compensatory mechanism in response to the restricted sacral motion caused by fusion. When the sacrum’s natural motion is compromised, the pelvis may adjust by tilting backward to maintain sagittal balance, which in turn increases the load on the SIJ and contributes to its degeneration. Additionally, the observed changes in thoracic kyphosis (TK) may suggest alterations in overall spinal alignment following lumbar fusion. These changes could be linked to SIJ dysfunction, as the imbalance in nutation-counternutation mechanics may affect the overall spinal posture. The adjustment in TK could be a compensatory response to altered load transmission through the sacrum and pelvis, which may subsequently impact SIJ biomechanics and lead to degeneration. Despite these significant radiological findings, there were no significant differences in clinical outcomes between the degeneration and non-degeneration groups, including measures of back pain, leg pain, Oswestry Disability Index (ODI), and EQ-5D scores. This suggests that, while radiographic evidence of SIJ degeneration is present in a significant proportion of patients, it does not necessarily correlate with symptomatic deterioration in the short term. It implies that some degree of degeneration may not immediately translate into clinically significant symptoms. However, longer-term follow-up studies are warranted to determine whether SIJ degeneration might contribute to the progressive development of pain, functional disability, or other long-term complications over time. Such studies would help clarify the full clinical implications of SIJ degeneration and its potential role in chronic pain syndromes or disability in post-fusion patients.
1. Limitations
This study has several limitations. First, its retrospective design limits the ability to draw causal conclusions. While retrospective studies can provide valuable insights, they do not allow for the establishment of cause-and-effect relationships. Second, SIJ degeneration was assessed based on radiological criteria without direct evaluation of SIJ-related pain. As a result, the clinical relevance of the radiological changes may not be fully captured, as degenerative changes observed on imaging may not always correlate with symptomatic presentation. Third, the follow-up period in this study may not have been long enough to assess the longterm impact of SIJ degeneration on functional outcomes. A longer follow-up period would provide a better understanding of how SIJ degeneration progresses over time and its potential effects on pain and disability. Future prospective studies with extended follow-up periods and more comprehensive clinical assessments are needed to clarify the relationship between SIJ degeneration and patient outcomes more conclusively.
Conclusions
Sacrum fixation, smoking, alcohol consumption, and age may serve as significant risk factors for SIJ degeneration following lumbar fusion surgery. Additionally, postoperative changes in pelvic tilt and thoracic kyphosis appear to be associated with the development of SIJ degeneration. These findings suggest that optimizing surgical techniques to minimize excessive stress on the SIJ, alongside proactive management of perioperative risk factors, may help reduce the incidence of SIJ degeneration and improve long-term outcomes for patients undergoing lumbar fusion surgery.
Fig. 1.
Evaluation factors for radiographic degeneration. Bone cyst (A). Bone erosion and intra-articular gas formation (B). Intra-articular bone formation (C). Joint space narrowing (D). Osteophyte (E). Sclerotic change (F).
Table 1.
Enrolled patient demographics
Number
472
Age
69.52±8.49
Sex (F/M)
258/214
BMI
25.09±5.02
Surgical time
224.47±82.22
Bleeding
682.56±503.84
S1 involved
178
37.71%
1 level
225
47.66%
2 level
166
35.16%
more than 3 level
81
17.16%
OLIF
66
13.98%
Preoperative Back VAS
5.80±2.50
Preoperative Leg VAS
5.85±2.64
Preoperative ODI
50.45±22.77
Preoperative EQ5D
0.70±1.10
Table 2.
Ratio of SI joint degeneration
Scoring change
No.
percentage %
2 >
337
71.39%
2 ≤
135
28.60%
Total
472
Table 3.
Comparison of demographic and radiologic parameter between si degeneration group and non-degeneration group
Degeneration group
Non-Degeneration group
p-value
Sex (F/M)
179/137
79/77
0.217
Age (years)
70.15±8.33
68.25±8.70
0.022*
BMI
25.07±5.64
25.13±3.47
0.882
Surgical time (min)
221.68 ±83.96
230.09±78.56
0.296
Intra-operative Bleeding (cc)
669.07±531.08
709.80±444.16
0.381
fusion level
1.77±0.89
1.77±1.12
0.973
BMD (T-score)
-1.438±1.227
-1.49±1.19
0.656
Alcohol
27.56%
15.19%
0.001*
Smoking
28.85%
12.97%
<0.001*
S1 involved
44.23%
34.49%
0.04*
OLIF
14.10%
13.92%
0.958
preT1PA
24.42±11.33
22.81±10.40
0.138
preGT
28.77±12.96
26.83±11.61
0.116
prePI
55.22±11.54
53.45±10.46
0.106
preSS
30.02±10.06
29.54±9.28
0.612
prePT
25.14±10.54
23.98±10.67
0.263
preLL
35.01±15.98
34.83±13.64
0.895
preTLK
9.98±8.32
9.48±8.80
0.547
preSVA
49.56±47.09
45.61±46.39
0.392
preTK
20.84±12.04
22.21±10.79
0.23
prePI-LL
20.26±16.98
18.16±13.90
0.153
Table 4.
Changes in spinopelvic parameters after surgery due to SI joint degeneration
Degeneration group
Non-Degeneration group
p-value
Δ T1PA
7.94±7.73
7.09±8.39
0.289
Δ GT
9.24±8.23
8.03±7.71
0.11
Δ PI
3.40±5.28
3.25±5.23
0.77
Δ SS
5.88±5.51
5.31±5.33
0.28
Δ PT
6.33±6.85
5.22±5.08
0.049*
Δ LL
9.26±9.26
9.03±8.10
0.77
Δ TLK
5.07±5.37
4.60 ±4.59
0.32
Δ SVA
34.03±28.95
35.23 ±33.38
0.704
Δ TK
6.45±8.42
6.76±6.60
0.17
Table 5.
Clinical outcome
Degeneration group
Non-Degeneration group
p-value
back VAS
1.77±0.89
1.76±1.12
0.645
Leg VAS
2.64±3.69
2.70±3.47
0.88
ODI
26.04±25.74
20.34±24.40
0.07
EQ5D
0.67±0.18
0.71±0.16
0.09
References
1. Dengler J, et al. Randomized trial of sacroiliac joint arthrodesis compared with conservative management for chronic low back pain attributed to the sacroiliac joint. JBJS 2019;101(5):400-11.
2. Ha KY, Lee JS, Kim KW. Degeneration of sacroiliac joint after instrumented lumbar or lumbosacral fusion: a prospective cohort study over five-year follow-up. Spine 2008;33(11):1192-8.
3. Ziegeler K, et al. Impact of age, sex, and joint form on degenerative lesions of the sacroiliac joints on CT in the normal population. Scientific Reports 2021;11(1):5903.
6. Etebar S, Cahill DW. Risk factors for adjacentsegment failure following lumbar fixation with rigid instrumentation for degenerative instability. Journal of Neurosurgery: Spine 1999;90(2):163-9.
7. Eck J, Humphreys S, Hodges S. Adjacent-segment degeneration after lumbar fusion: a review of clinical, biomechanical, and radiologic studies. American journal of orthopedics (Belle Mead, NJ) 1999;28(6):336-40.
8. Murata Y, et al. Origin and pathway of sensory nerve fibers to the ventral and dorsal sides of the sacroiliac joint in rats. Journal of Orthopaedic Research 2001;19(3):379-83.
9. Cohen SP, Chen Y, Neufeld NJ. Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis and treatment. Expert review of neurotherapeutics 2013;13(1):99-116.
15. Shibata Y, Shirai Y, Miyamoto M. The aging process in the sacroiliac joint: helical computed tomography analysis. Journal of Orthopaedic Science 2002;7(1):12-8.
17. Resnick D, Niwayama G, Goergen T. Comparison of radiographic abnormalities of the sacroiliac joint in degenerative disease and ankylosing spondylitis. American Journal of Roentgenology 1977;128(2):189-96.
18. Obeid I, et al. The global tilt: evaluation of a parameter considering the global spinopelvic alignment. Le Journal medical libanais. The Lebanese medical journal 2016;64(3):146-51.
19. Protopsaltis TS, et al. The lumbar pelvic angle, the lumbar component of the T1 pelvic angle, correlates with HRQOL, PI-LL mismatch, and it predicts global alignment. Spine 2018;43(10):681-7.
20. Bridwell KH, et al. Anterior fresh frozen structural allografts in the thoracic and lumbar spine: do they work if combined with posterior fusion and instrumentation in adult patients with kyphosis or anterior column defects? Spine 1995;20(12):1410-8.
22. Zhang S, et al. Effect of cigarette smoking and alcohol consumption on disease activity and physical functioning in ankylosing spondylitis: a cross-sectional study. International journal of clinical and experimental medicine 2015;8(8):13919.
23. Fatica M, et al. The Effects of Smoking, Alcohol, and Dietary Habits on the Progression and Management of Spondyloarthritis. Journal of Personalized Medicine 2024;14(12):1114.
24. Helgeson MD, Bevevino AJ, Hilibrand A.S. Update on the evidence for adjacent segment degeneration and disease. The spine journal 2013;13(3):342-51.
25. Joukar A, et al. The Sacroiliac Joint: A Review of Anatomy, Biomechanics, Diagnosis, and Treatment Including Clinical and Biomechanical Studies (In Vitro and In Silico). Handbook of Spine Technology 2021;349-74.
29. Kumar M, Baklanov A, Chopin D. Correlation between sagittal plane changes and adjacent segment degeneration following lumbar spine fusion. European spine journal 2001;10(4):314-9.
30. Toyohara R, Ohashi T. A literature review of biomechanical studies on physiological and pathological sacroiliac joints: Articular surface structure, joint motion, dysfunction and treatments. Clinical Biomechanics 2024;106233.
Sacroiliac Joint Degeneration Following Lumbar Fusion: What are the Risk Factors?
Fig. 1. Evaluation factors for radiographic degeneration. Bone cyst (A). Bone erosion and intra-articular gas formation (B). Intra-articular bone formation (C). Joint space narrowing (D). Osteophyte (E). Sclerotic change (F).
Fig. 1.
Sacroiliac Joint Degeneration Following Lumbar Fusion: What are the Risk Factors?
Number
472
Age
69.52±8.49
Sex (F/M)
258/214
BMI
25.09±5.02
Surgical time
224.47±82.22
Bleeding
682.56±503.84
S1 involved
178
37.71%
1 level
225
47.66%
2 level
166
35.16%
more than 3 level
81
17.16%
OLIF
66
13.98%
Preoperative Back VAS
5.80±2.50
Preoperative Leg VAS
5.85±2.64
Preoperative ODI
50.45±22.77
Preoperative EQ5D
0.70±1.10
Scoring change
No.
percentage %
2 >
337
71.39%
2 ≤
135
28.60%
Total
472
Degeneration group
Non-Degeneration group
p-value
Sex (F/M)
179/137
79/77
0.217
Age (years)
70.15±8.33
68.25±8.70
0.022*
BMI
25.07±5.64
25.13±3.47
0.882
Surgical time (min)
221.68 ±83.96
230.09±78.56
0.296
Intra-operative Bleeding (cc)
669.07±531.08
709.80±444.16
0.381
fusion level
1.77±0.89
1.77±1.12
0.973
BMD (T-score)
-1.438±1.227
-1.49±1.19
0.656
Alcohol
27.56%
15.19%
0.001*
Smoking
28.85%
12.97%
<0.001*
S1 involved
44.23%
34.49%
0.04*
OLIF
14.10%
13.92%
0.958
preT1PA
24.42±11.33
22.81±10.40
0.138
preGT
28.77±12.96
26.83±11.61
0.116
prePI
55.22±11.54
53.45±10.46
0.106
preSS
30.02±10.06
29.54±9.28
0.612
prePT
25.14±10.54
23.98±10.67
0.263
preLL
35.01±15.98
34.83±13.64
0.895
preTLK
9.98±8.32
9.48±8.80
0.547
preSVA
49.56±47.09
45.61±46.39
0.392
preTK
20.84±12.04
22.21±10.79
0.23
prePI-LL
20.26±16.98
18.16±13.90
0.153
Degeneration group
Non-Degeneration group
p-value
Δ T1PA
7.94±7.73
7.09±8.39
0.289
Δ GT
9.24±8.23
8.03±7.71
0.11
Δ PI
3.40±5.28
3.25±5.23
0.77
Δ SS
5.88±5.51
5.31±5.33
0.28
Δ PT
6.33±6.85
5.22±5.08
0.049*
Δ LL
9.26±9.26
9.03±8.10
0.77
Δ TLK
5.07±5.37
4.60 ±4.59
0.32
Δ SVA
34.03±28.95
35.23 ±33.38
0.704
Δ TK
6.45±8.42
6.76±6.60
0.17
Degeneration group
Non-Degeneration group
p-value
back VAS
1.77±0.89
1.76±1.12
0.645
Leg VAS
2.64±3.69
2.70±3.47
0.88
ODI
26.04±25.74
20.34±24.40
0.07
EQ5D
0.67±0.18
0.71±0.16
0.09
Table 1. Enrolled patient demographics
Table 2. Ratio of SI joint degeneration
Table 3. Comparison of demographic and radiologic parameter between si degeneration group and non-degeneration group
Table 4. Changes in spinopelvic parameters after surgery due to SI joint degeneration