Purpose This study aimed to evaluate whether percutaneous vertebroplasty (PVP) contributes to vertebral height restoration and sagittal alignment correction in osteoporotic vertebral compression fractures (OVCF), focusing on thoracolumbar junction fractures.
Methods A retrospective review of 40 patients with single-level OVCF at T10–L2 treated with PVP was performed. Vertebral heights (anterior, middle, and posterior) and sagittal alignment (thoracic kyphosis, lumbar lordosis, sagittal vertical axis, and segmental Cobb's angle) were measured preoperatively, at 3 months, and at 6 months. Clinical outcomes included visual analog scale and EuroQol-5 Dimensions.
Results Significant pain relief and improvement in quality of life were observed at 6 months postoperatively. Vertebral height restoration, particularly in the anterior and middle portions, was noted at 3 months; however, partial loss of the restored height occurred by 6 months. Most sagittal alignment parameters showed no significant postoperative change, although lumbar lordosis significantly increased, resulting in a reduced pelvic incidence–lumbar lordosis mismatch.
Conclusion PVP provides meaningful clinical improvement in thoracolumbar OVCFs and offers early vertebral height restoration; however, this radiologic benefit is not sustained over time. While limited improvement in lumbar lordosis was observed, PVP does not substantially correct global sagittal alignment. These findings suggest that PVP should be considered primarily a pain-relieving and stabilizing procedure rather than a deformity-correcting intervention.
Purpose To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
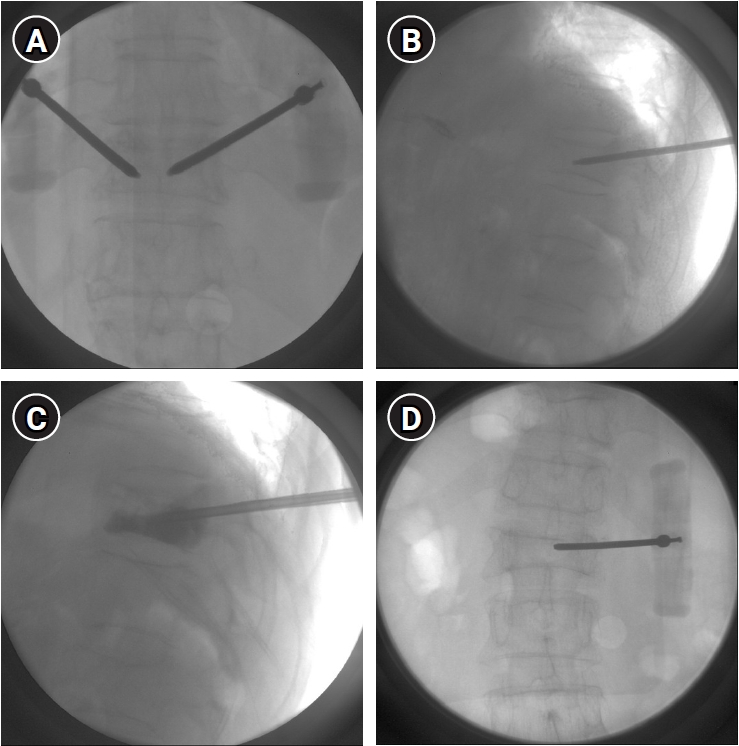
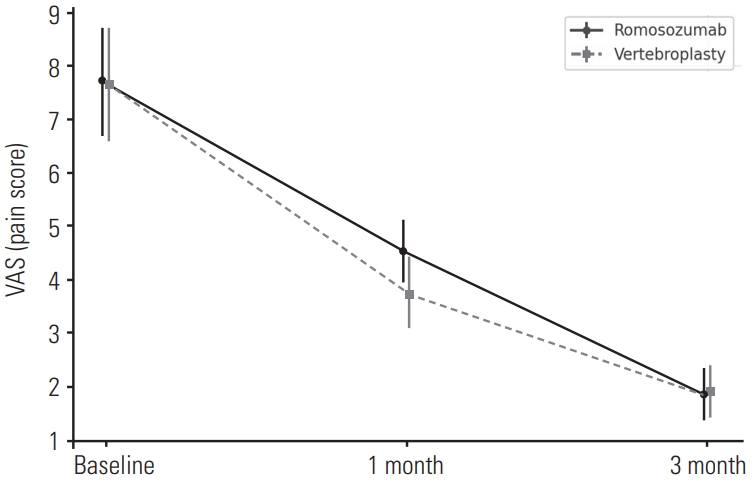
Material and Methods: This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.
Vertebral compression fracture is one of the most common osteoporotic fractures along with hip fractures. In some patients, pain was improved through conservative treatment including pharmaceuticals, bracing and physiotherapy. But it has been reported that conservative therapy is insufficient in many patients with vertebral compression fracture. Accordingly, interest in vertebroplasty has increased and many studies have been reported that vertebroplasty have therapeutic effects in acute vertebral compression fracture. On the other hand, some studies have been reported that the effect of vertebroplasty was not significant. So whether vertebroplasty is useful or not is still controversial. Therefore, in this review article, we will review open-label randomized controlled trials and blinded randomized controlled trials that provide high-level evidence and provide an opinion on which patients it is appropriate to perform vertebroplasty.
Introduction We describe the complications that can occur after percutaneous vertebroplasty using bone cement for osteoporosis vertebral compression fracture.
Main subject: The most common complication of percutaneous vertebroplasty is the leakage of bone cement.
Leakage of bone cement has been reported variously and could leak into the spinal or neural foramen, adjacent intervertebral disc and soft tissues around the spine, and venous systems. The most serious complications are neurologic symptoms due to spinal cord and nerve root compression and complications associated with death due to heart and pulmonary embolism. In addition, recompression fracture or adjacent vertebral compression fracture might occur and various treatment methods have been proposed.
Conclusion The complications that can occur after percutaneous vertebroplasty have been reported variously, including neurologic deficits due to the leakage of bone cement and lung and heart embolism. In addition, there is a possibility of recompression fracture or adjacent compression fracture. Therefore, you should be careful about percutaneous vertebroplasty. Finally, patients with many risk factors regarding complications of vertebroplasty would need close observation and follow-up.
Percutaneous vertebroplasty and balloon kyphoplasty are both safe and effective procedures in case of patients with osteoporotic vertebral compression fractures. The authors have already reported a new technique called lordoplasty using polymethylmethacrylate to manage vertebral osteoporotic compression fractures. The purpose and indication of lordoplasty do not differ from that of percutaneous vertebroplasty or balloon kyphoplasty. However, there are advantages of lordoplasty in terms of restoration of the wedge and kyphotic angle and cost-effectiveness compared with the other procedures mentioned above. For the advantages of lordoplasty, authors thereby introduce the detailed procedure of lordoplasty.
Purpose Osteoporosis is an age-related systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone contents, with a consequent increase in bone fragility. In severe osteoporosis progressive collapse of multiple vertebrae is and unsolved problem. Medical treatment appears to be too slow to prevent the course. Recently, there are some reports on the results of the percutaneous vertebroplasty (VP) in treating the multi-level osteoporotic vertebral compression fractures (VCFs). we reviewed painful multi-level osteoporotic VCFs treated by percutaneous VP and assess the efficacy and safety of multiple percutaneous cement VP in the treatment of multi-level osteoporotic VCFs.
Materials and Methods From January 2008 to August 2010, the clinical cases and radiographic records were reviewed retrospectively for 28 patients treated for the multi-level painful osteoporotic VCFs by percutaneous cement VP.
Initially radiography and MRI of the spine were performed. Spine radiographs were repeated at post-operation, 1,3 months and final follow-up. The patient’s outcomes of demographic, clinical, radiologic and procedural data were analyzed and assessed using self-report and physiological measures. A t-test was used for means of VAS, anterior vertebral height and kyphotic angle. Statistical analysis was performed with the SPSS(Version 15.0.1, Chicago, Illinois). The p-values of < 0.001 were deemed significant.
Results The back pain recorded using the VAS improved significantly in all cases, from 7.7±1.0(6-10), points preoperatively to 2.0±0.7(1-3) points postoperatively (p<0.001) and then 2.8±0.8(1-4) points at the follow-up (p<0.001).
The anterior heights increased from 17.40±4.98 to 21.02±5.36 after VP procedures (p<0.001) and finally 19.49±5.28 (p<0.001). The kyphotic angle was 12.58º preoperatively and improved to 4.39º postoperatively, but kyphotic deformities became worse in 12.80º.
Conclusion The vertebroplasty for patients with multiple osteoporotic vertebral compression fractures may improve pain and can be effective for preventing adjacent fractures, restoration of vertebral height and maintenance of sagittal alignment. Patients with multiple osteoporotic compression fractures have many comorbidity, the surgeon should be conscious to all procedure.
Purpose Higher viscous cement can be injected through larger-diametered tubes with lower pressure. The lower the cement modulus is, the less the stress-transfer would be. The lower-pressure percutaneous vertebroplasty with blood-mixed cement(LP-PVPblood ) was devised to overcome technical problems in conventional percutaneous vertebroplasty(C-PVP). We would like to prove the validity of technical modifications to increase viscosity of cement being injected and reduce final modulus of cement.
Methods Nineteen C-PVPs, 51 kyphoplasty (KPs), 23 LP-PVPs and 70 LP-PVPblood s were analyzed in radiologic point of view. The successful cases with sufficient cement volume(≥ 5ml) were also analyzed as a subgroup.
Results Asymptomatic cement leakage(CL) showed a similar tendency in LP-PVblood (17.1%) compared to other groups(21.1~27.5%, p=0.514), even though the injected cement volume in LP-PVPblood (6.9ml) was much more than that of C-PVP(3.5ml, p=0.000). Vertebral height restoration(VHR) was significantly higher(11.7%) than C-PVP(4.7%, p=0.024). Vertebral body subsidence(VS) was less in KP(1.1%) than others(2.1~5.9%, p=0.000). But, adjacent vertebral compression fractures(VCFs) happened more frequently in KP(15.7%) than others (0~5.3%, p=0.001).
In subgroup analysis, the rates of successful cases were significantly higher in LP-PVPblood (85.7%) than in C-PVP(5.3%, p=0.000). CLs and VHRs showed no significant differences. VS was significantly less in KP(1.0%, p=0.000) but adjacent VCF developed more frequently in KP(21.1%) than LP-PVPblood (0%, p=0.001).
Conclusions The LP-PVPblood which stands for larger diameter tubes for injecting sufficient volume of higher viscous cement and more interdigitation by omitting balloon and lower modulus blood-mixed cement was appraised to reduce risk of cement leakage than C-PVP and decrease stress transfer to adjacent vertebrae than KP.
Purpose To find the factors that affecting surgical outcome after vertebroplasty and kyphoplasty in osteoporotic compression fracture.
Materials and Methods Pre-operative, post-operative, technical, radiological factors of patients who diagnosed osteoporotic compression fracture and treated with vertebroplasty or kypholasty during from January 2008 to December 2010, were compared by outcomes that acute and chronic back pain, refracture rate and maintenance of the reduction of body height.
Results The period of acute pain after the operation was less than 3 days in groups of trauma( p=0.0262) and hospital treatment(p=0.0113) before the operation as pre-operative factors. When it comes to technical factors, the cases of vertebroplasty(p<0.0001), injection of cement(p=0.0053), the case without leakage of cement(p=0.007) and the case being under anesthesia (p<0.005)achieved statistical significance. In the groups who got conservative treatment less than 1 week (p=0.0119) and local anesthetics(p=0.0246), refractures occurred many times. The groups of non-trauma(p=0.0105), having had more than 30% compression(p=0.0244) and the group that prescribed bisphosphonate(p=0.0286) statistical significantly maintained restoration.
Conclusion Conservative treatment in the hospital for more than 1 week before the operation, operation being under anesthesia and intake of bisphosphonate after the operation put positive effects on the outcome of vertebroplasty and kyphoplasty.

 First
First Prev
Prev

