Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
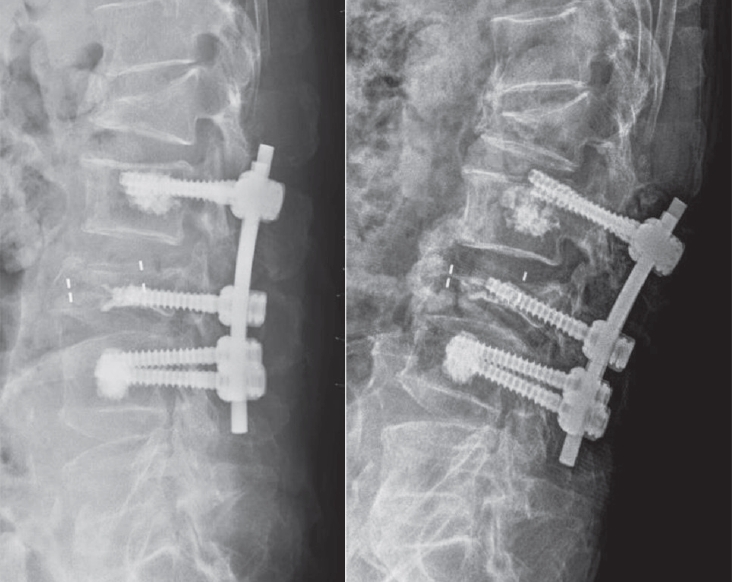
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Background Percutaneous-short segment screw fixation (SSSF) without bone fusion has proven to be a safe and effective modality for thoracolumbar spine fractures (TLSFs). When fracture consolidation is confirmed, pedicle screws are no longer essential, but clear indications for screw removal following fracture consolidation have not been established.
Methods In total, we enrolled 31 patients with TLSFs who underwent screw removal following treatment using percutaneous-SSSF without fusion. Plain radiographs, taken at different intervals, measured local kyphosis using Cobb’ angle (CA), vertebra body height (VBH), and the segmental motion angle (SMA). A visual analogue scale (VAS) and the Oswestry disability index (ODI) were applied pre-screw removal and at the last follow-up.
Results The overall mean CA deteriorated by 1.58º (p<0.05) and the overall mean VBH decreased by 0.52 mm (p=0.001). SMA preservation was achieved in 18 patients (58.1%) and kyphotic recurrence occurred in 4 patients (12.9%). SMA preservation was statistically significant in patients who underwent screw removal within 12 months following the primary operation (p=0.002). Kyphotic recurrence occurred in patients with a CA ≥20º at injury (p<0.001) with a median interval of 16.5 months after screw removal. No patients reported worsening pain or an increased ODI score after screw removal.
Conclusion Screw removal within 12 months can be recommended for restoration of SMA with improvement in clinical outcomes. Although, TLSFs with CA ≥20º at the time of injury can help to predict kyphotic recurrence after screw removal, the clinical outcomes are less relevant.
Purpose Minimally invasive technique in spinal surgery have evolved including cortical bone trajectory (CBT) screw technique which is s new lumbar pedicle screw path, as an alternative fixation technique for lumbar spine.
Theoretical advantage is that it provides enhanced screw torque and has biomechanical characteristics, also it minimizes approach-related damages. Midline lumbar fusion (MIDLF) has appeared with CBT screw technique.
Many studies of CBT screw reported the effectiveness of MIDLF. We adopted this technique for lumbar degenerative spondylolisthesis and evaluated early radiological outcomes.
Materials and Methods From May 2014 to March 2015, 17 patients (mean age 65.6±7.5 years; 4 males, 13 females) underwent MIDLF procedures for the treatment of single level lumbar spondylolisthesis. Average follow-up period was 8.8±2.7 months. Initial and last follow-up X-ray and computed tomography (CT) were evaluated for screw malposition, detection of peri-screw halo, loosening of the construct, or signs of spinal instability.
Results The average bone mineral density (BMD) was -1.9±0.8. Eleven patients were fused at L4-5, 5 were at L3-4, and 1 was at L2-3. Five CBT screws were converted into pedicle screws due to intraoperative misposition of screws, so total 63 CBT screws were evaluated for peri-screw halo and malposition. There were no findings of screw pull-out or breakage in all screws. Four out of 63 (6.3%) screws were judged as peri-screw halo, and 20 (41.2%) screws were judged as malposition (1 medial; 2 superior; 17 lateral pedicle violation). But, there were no screw related nerve root injury. In all cases, interbody bony mass were identified. Four out of 17 (23.6%) patients were detected more than 2 degrees motions on flexion-extension lateral X-rays at final follow-up, and 1 out of these 4 patients was identified loss of reduction. There was no operation related complication.
Conclusion There is no doubt that MIDLF with CBT screw is the minimally invasive method. Many numbers of screw malposition identified in our series were thought to be due to our earlier experience of trying free hands technique.
We recommend the use of intraoperative fluoroscopy, which achieve accuracy. Although MIDLF with CBT has theoretical strengths, we must evaluate further long-term clinical follow-up and measure outcome.
Background Oblique and anterior lumbar interbody fusion have been widely performed in the lumbar spinal disease but we cannot get a direct decompression effect with these procedure.
Objective: The purpose of this study is to report clinical and imaging outcomes of microscope assisted direct decompression combined with oblique lumbar interbody fusion (OLIF) or anterior lumbar interbody fusion (ALIF).
Methods Twelve patients who received microscope assisted direct decompression during OLIF or ALIF for lumbar spinal stenosis were enrolled. The OLIF was performed for the lesion upper than the L4-5 or in the case of multisegmental disease. The ALIF was performed for the lesion at the L5-S1. After anterior-approaching surgery, percutaneous fixation of pedicle screw was performed and we did not perform an additional decompression posteriorly in all cases. For the clinical outcomes, we evaluated short form 36 (SF-36), Oswestry disability index (ODI) score and visual analog scale (VAS) pain score. For the imaging outcomes, we obtained postoperative lumbar magnetic resonance imaging (MRI).
Results The OLIF was performed for 9 patients and the ALIF was performed for 3 patients. In the clinical outcomes, SF-36 was improved from 25.40 to 69.83 and ODI score was also improved from 69.83 to 16.50. VAS pain score of back was improved from 4.3 to 1.6 and VAS pain score of leg was improved from 7.5 to 2.2. In the imaging outcomes, all patients had severe stenosis before surgery. After surgery the severity of the stenosis was reduced to mild state in 9 cases and moderate state in 3 cases postoperatively.
Conclusions We could obtain the good clinical outcomes and effective decompression through microscope assisted direct decompression during OLIF or ALIF.
Lumbar fusion surgery for lumbar degenerative diseases has increased in the past several decades and many techniques for fusion surgery have been introduced. Recently lateral lumbar interbody fusion with minimally invasive technique was introduced and accepted as a useful method for various lumbar degenerative disease. It can produce good correction for sagittal and coronal imbalance with relatively decreased morbidity. The advantage of lateral lumbar interbody fusion is that it can avoid injury to the abdominal large vessels and neural structures which is more common during posterior approaches. However various complications had been reported. Complications related with lateral lumbar interbody fusion include neurologic complications including thigh pain and numbness, vascular complications including arterial injury, cage related complication such as cage subsidence and vertebral body fractures. Therefore special care should be taken to avoid possible complications in lateral lumbar interbody fusion surgery.
A 77-year-old female suffering from severe degenerative scoliosis, spinal stenosis and lumbar disc herniation underwent Direct lateral lumbar interbody fusion (DLIF) at L2-4. On the 3rd postoperative day, she complained of severe back pain without any trauma history. Simple radiograph revealed L3 vertebral fracture and cage subsidence.
Pain was subsided after conservative treatment including TLSO and medication. Radiographic union was achieved at fractured vertebra after 3 months. Solid fusion was observed at operated level after 6 months. Patient has visited our clinic without any pain. DLIF is one of novel minimally invasive spine procedures available today. It is designed to maximize benefits and minimize risks of other traditional techniques such as anterior approach and posterior approach. However, there can be some risk of cage subsidence and vertebral fracture after DLIF. Therefore, care should be taken to avoid cage subsidence during the operation.
Minimally invasive TLIF has been reported to be a useful treatment option for the patients with various degenerative lumbar diseases. Many studies have reported the favorable clinical results of MIS TLIF. However it remains technically demanding, leading to higher complication rates and longer operative times during the early period of the learning curve. It showed some potential complications due to small working space and visual field. In this study, authors tried to find out various possible complications and some tips avoiding these complications through the review of various articles and authors’ clinical experiences. In many studies, the general complication fusion rates of MIS TLIF have been reported to be similar to that of open fusion. The technical difficulty of the procedure, combined with inadequate training, is evident in initial studies of MIS TLIF. A difficult learning curve of MIS TLIF demands that surgeons have sufficient preclinical training, and education is obtained before the application of MIS TLIF in clinical practice.
Purpose Pull-out of pedicle screw in posterior pedicle fixation for thoracic and lumbar burst fractures causes delayed rehabilitation, persistant pain, and imblance of sagittal plane. In this study we try to analyse the factors that cause the pull-out of pedicle screw.
Materials and Methods From March 01, 2006 to December 31, 2009, we assorted into two group; Group I for pullout pedicle, Group II for control. Plane lateral x-ray view film of thoracolumbar spine was taken on preoperation, postoperation, the first time when screw was pulled out and last follow up. we measure inserted angle for the upper endplate of screw, convergency angle and change of body height loss and kyphotic angle. We analysed corelation between these measuring values and pedicle screw pull-out by Mann-Whitney test and T-test.
Results Pull-out of pedicle screw was found at mean 5weeks among nine cases. For inserted pedicle screws, which place in upper and lower vertebral body of fractured one, Value of inserted angle for upper end plate and convergency angle was found non-significant(p>0.05, Mann-Whitney test). Restoration of height loss and kyphotic angle of fractured vertebral body was statically significant(p<0.05, T-test).
Conclusion In posterior pedicle fixation for thoracic and lumbar burst fractures, sufficient restoration of height loss and kyphotic angle is important factor for prevention of screw pull-out than inserted angle for upper end plate and convergency angle at a short period of time. Therefore we think that sufficient anterior fixation of vertebral body and restoration of kyphotic angle have a decisive effect on prognosis of patients.
Purpose To evaluate the method of inserting cortical bone trajectory pedicle screws (cortical screws) and potential complications when performing lumbar fusion.
Methods Lumbar fusion with cortical screw fixation in the hard cortical bone of the pars interarticularis of vertebrae was introduced to replace conventional pedicle screws. We review the literature on the biomechanics of cortical screw insertion and on the clinical outcomes.
Results In vitro biomechanical testing has shown that cortical screws have greater pullout strength than traditional pedicle screws due to the strong bone–screw interface in cortical bone. Cortical screws have the advantages of requiring minimal muscle dissection and shortening the surgery. However, early screw loosening and loss of reduction have been reported.
Conclusions When inserting cortical screws, the entry point and trajectory of the screws are important and a meticulous surgical technique is needed to prevent potential screw-related complications.
We reviewed literatures relating to minimally invasive lateral lumbar interbody fusion for the treatment of adult degenerative spinal deformity. Most of literatures were retrospective case series with a small numbers of patients.
A prospective multicenter study was published in two separate papers. This procedure was effective in treating the coronal deformity. On the other hand, restoring the sagittal plane remains an issue. Pseudarthrosis was problematic, especially in the cases without use of the human recombinant bone morphogenetic protein-2 (rhBMP-2) and bilateral pedicle screw fixation. Temporary sensory deficits and transient leg weakness was the most common complication after lateral lumbar interbody fusion. Careful patient selection is important for the application of lateral minimally invasive techniques for adult degenerative scoliosis.
Purpose The purpose of the study was to investigate the effect of obesity on the accuracy of percutaneous pedicle screw placement.
Materials and Methods We performed a retrospective analysis on the first 89 patients undergoing minimally invasive lumbar fusion with percutaneous pedicle screw placements for the treatment of degenerative lumbar spinal disorder.
Based on patient’s body mass index (BMI), patients were divided into 3 groups: group 1 – normal weight (BMI<25, 38 patients, 157 screws); group 2 – overweight (25≤BMI<30, 29 patients, 124 screws); group 3 – obese (BMI≥30, 22 patients, 89 screws). Using postoperative computed tomography (CT) scans, the position of placed screws to the pedicle or anterior body perforation was evaluated using the following grading method: Grade A, completely in the range without pedicle cortex violation; Grade B, pedicle wall violation<2 mm; Grade C, pedicle wall violation 2 to 4 mm; and Grade D, pedicle wall violation>4 mm.
Results Among the 370 pedicle screws, 308 screws (83%) were perfectly placed within the pedicle. Among the 62 misplaced screws, 45 screws were grade B pedicle breaches (73%, 45/62), and 45 screws were misplaced in lateral direction (73%, 45/62). 36 screws (10%) perforated the anterior vertebral cortex. Twenty eight screws were misplaced in overweight group, 12 screws in obese group, and 22 screws in normal weight group. With the number of screws available, subgroup analysis did not reveal a significant difference in the grade (p=0.10) or the direction (p=0.97) of pedicle breaches among groups.
Conclusion Our data suggest that obesity does not affect the accuracy of percutaneous pedicle screw placement. We do not hesitate or deny the surgery because of patient’s heavy body habitus, which seems to be a apparent benefit of minimally invasive spinal surgery.
Introduction Recently, minimally invasive lateral approach for the lumbar spine is revived and getting popularity under the name of XLIF or DLIF by modification of mini-open method using sequential tubular dilator and special expandable retractor system.
Purpose s: The purposes of this study were to introduce the mini-open lateral approach for the anterior lumbar interbody fusion (ALIF), and to investigate the advantages, technical pitfalls and complications & to provide basic knowledge on XLIF or DLIF
Materials and Methods Seventy-four patients who underwent surgery by the mini-open lateral approach from September 2000 to April 2008 with various disease entities were included. Blood loss, operation time, incision size, postoperative time to mobilization, length of hospital stay, technical problems and complications were analyzed.
Results With this approach, we can reach form T12 to L5 subdiaphragmatically. The blood loss and operation time of patients who underwent simple ALIF were 61.2 ml and 86 minutes for one level, 107 ml and 106 minutes for two levels, 250 ml and 142.8 minutes for three levels, and 400 ml and 190 minutes for four levels of fusion, respectively.
The incision sizes were on average 4.5cm for one level, 6.3 cm for two levels, 8.5 cm for three levels and 10.0 cm for four levels of fusion. The complications were retroperitoneal hematoma in two cases, pneumonia in one case and transient lumbosacral plexus palsy in three cases.
Conclusion The mini-open lateral approach is simpler & safer than XLIF or DLIF with very short learning curve. Trial of mini-open lateral approach would be helpful before trial of XLIF or DLIF. However, special attention is required to complications such as transient lumbosacral plexus palsy.
A 45 year-old male was brought to our hospital with severe back pain and motor, sensory impairment in both lower extremities. He had no underlying diseases including coagulapathy. Motor weakness below both hip joint and decreased sensory below T12 dermatome, voiding dysfunction were examined. The MRI showed a spinal subdural hematoma at the thoracolumbar region, which was extremely rare. Medical treatment was applied without surgical interventions. After two weeks, motor weakness, sensory impairment, and voiding dysfunction were improved. And he returned to his daily activities. We present this case and literature reviews because traumatic spinal subdural hematoma is an extremely rare disease and the condition was treated successfully in conservative manner.

 First
First Prev
Prev

