Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
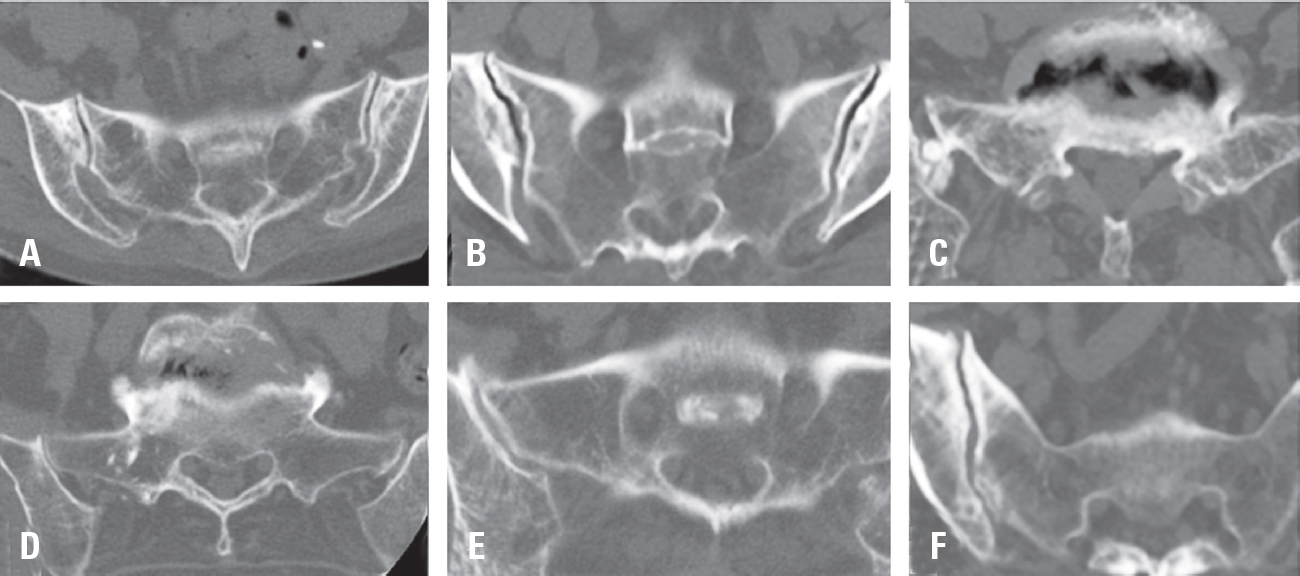
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Among the complex causes of chronic low back pain, suboptimal injury of ligament in the lumbosacral spine is common. Injured ligaments can become a primary pain source and raise secondary pain with referred pain pattern.
Due to the low blood supply to the ligaments, ligaments are notoriously poor healer. In order to compensate the poor healing of ligament, prolotherapy has been introduced and used for more 60 years. To date, no definite recommendations have not been made based on literature available. However, if conventional treatment modalities have failed in patient with chronic back pain in lumbosacral spine, prolotherapy targeted on ligaments around lumbosacral spine should be considered in appropriate patients.
Background Owing to its new introduction, there are few documents on pit-falls of biportal endoscopic spine surgery (BESS) clinically. The authors reported etiologies in need of early exploration after BESS for lumbar degenerative diseases and strategies to overcome them.
Methods BESS were performed for lumbar spine diseases (LSDs) by two spine surgeons from December 2013 to March 2016. Postoperative MRI was checked for all cases and following-up MRIs in the case in need of revision surgery within six months after the first surgery due to pain intolerable, sustained or recurred. The complicated cases were reviewed and classified as radiographic and operative findings to reveal the main reasons for early explorations.
Results The 562 cases (M:295, F:267, Age 58.5±14.1 yrs, 20~88 yrs) included lumbar disc herniation (LDH) (255 cases), extraforaminal disc herniation (22 cases), spinal stenosis (218 cases), degenerative spondylolisthesis (27 cases), revision surgery after recurred disc herniation or restenosis after open surgery (24 cases), juxtafacet cyst (11 cases), adjacent segment stenosis with fusion surgery (3 cases), and spondylolytic spondylolisthesis (2 cases). Early explorations were needed in 43 cases (7.7%) at 26.1±31.5 days after the initial operations. Causative etiologies were listed as recurred LDH (12 cases, 27.9%), remnant stenosis (7 cases, 16.3%), remained ruptured disc fragment (6 cases, 14.0%), root edema (5 cases, 11.6%), synovitis (4 cases, 9.3%), hematoma (3 cases, 7.0%), dura tear (2 cases, 4.7%), recurred stenosis (2 cases. 4.7%), wrong level (1 case, 2.3%) and postoperative fungal infection (1 case, 2.3%).
Thirty-one cases (72.1%) were revised within 4 weeks and most conditions (40 cases, 93.0%) were improved after early exploration using BESS. Two cases of dura tear were conversed to open repair. One case of fungal infection was suspected to related with the patient’s medical illness including long-term steroid use for chronic lung disease with pulmonary fibrosis and Diabetes mellitus.
Conclusions Preoperative planning should be prepared carefully to decrease early exploration. It was helpful to comparing MRIs immediately postoperative and early following-up to find the reasons. Don’t hesitate to explore the operated site again using BESS, because most etiologies are supposed to be controlled by early exploration without need of converting to open surgery except in the case of dura tear in need of dural repair.

 First
First Prev
Prev

