This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Spinal artery aneurysms are exceedingly rare, and their natural history remains poorly understood. Diagnosis can be challenging due to their small size and the difficulty in detection by MR angiography (MRA) or CT angiography (CTA); Digital Subtraction Angiography (DSA) is considered the gold standard diagnostic tool. This case report presents two cases of ruptured thoracic radicular artery aneurysms leading to subdural hematoma (SDH) and subarachnoid hemorrhage (SAH). The first patient, a 71-year-old female, presented with bilateral leg weakness, headache, and severe back pain, where multiple fusiform dilatations of the left T9 radiculopial artery were identified. She showed significant improvement after surgical intervention. The second patient, a 75-year-old female, presented with paraplegia and severe back pain, and a saccular dilatation in the right T10 radiculopial artery was found. She underwent endovascular embolization but showed no neurological improvement. These cases highlight the diverse clinical presentations, diagnostic challenges, and uncertainties in management strategies for ruptured spinal artery aneurysms, emphasizing the need for prompt intervention, especially in cases with significant or progressive neurological deficits.
척수 동맥류는 매우 희귀하며, 병의 유발 빈도나 원인 등이 잘 알려져 있지 않습니다. 영상의학적인 진단은 크기가 작아 자기공명 혈관조영술이나 전산화단층 혈관조영술로 발견하기 어렵기 때문에 까다로우며, 디지털 감산 혈관조영술이 표준 진단 도구입니다. . 본 증례 보고는 흉추부위 뿌리 동맥류 파열로 인해 척수내 경막하 혈종과 두개강내 지주막하 출혈이 발생한 사례를 소개하였습니다. 첫 번째 환자인 두개강내 지주막하 출혈이 진단되어 내원한 환자이나 추가적인 평가로 출혈의 원인이 뇌내 동맥류 파열이 아닌 좌측 흉추 9번 뿌리 동맥의 동맥류 파열로 인한 것임을 확인하여 수술적 치료를 통해 성공적으로 치료하였습니다. 두 번째 환자인 75세 여성은 하반신 마비를 주소로 내원하여, 우측 T10 뿌리 동맥류의 파열로 인한 것을 확인하였으며, 혈관내 색전술로 성공적으로 동맥류를 막았지만 신경학적 호전은 지속되었습니다. 척수 동맥류 파열은 파열된 위치에 따라 다양한 임상 양상이 나타날 수 있으며, 진단적 어려움이 있습니다. 동맥류의 위치 및 신경학적 악화 여부에 따라 다양한 치료 전략을 세워야 할 것으로 생각됩니다.
Spinal artery aneurysms (SAAs) are exceptionally rare vascular lesions of the spinal cord, posing significant diagnostic and therapeutic challenges. Unlike their more common cranial counterparts, SAAs have a low incidence, and their natural history and optimal management guidelines remain largely undefined due to limited research, primarily consisting of case reports and small series.5,6,8,10,11)
Clinical presentation varies based on the hemorrhage location and extent, ranging from severe headache to back pain, with potential for compressive myelopathy or cauda equina syndrome.10,13) Diagnosis is challenging, as conventional magnetic resonance angiogram or computed tomography angiogram often miss these small lesions, making Digital Subtraction Angiography (DSA) the gold standard.1) Optimal SAAs management lacks universal consensus.12) Treatment decisions are individualized, considering etiology, size, location, and neurological status. Options include conservative observation, endovascular embolization, or microsurgical techniques like trapping or excision.8,10,12,14) Intervention carries risks, especially with critical spinal cord feeders.
This report details two cases of ruptured thoracic radicular artery aneurysms presenting with subdural and subarachnoid hemorrhage. By illustrating their varied clinical presentations, diagnostic pathways, and contrasting treatment outcomes, we aim to highlight the complexities in managing these rare and challenging spinal vascular pathologies.
Case Presentation
1. Case I: Surgical approach
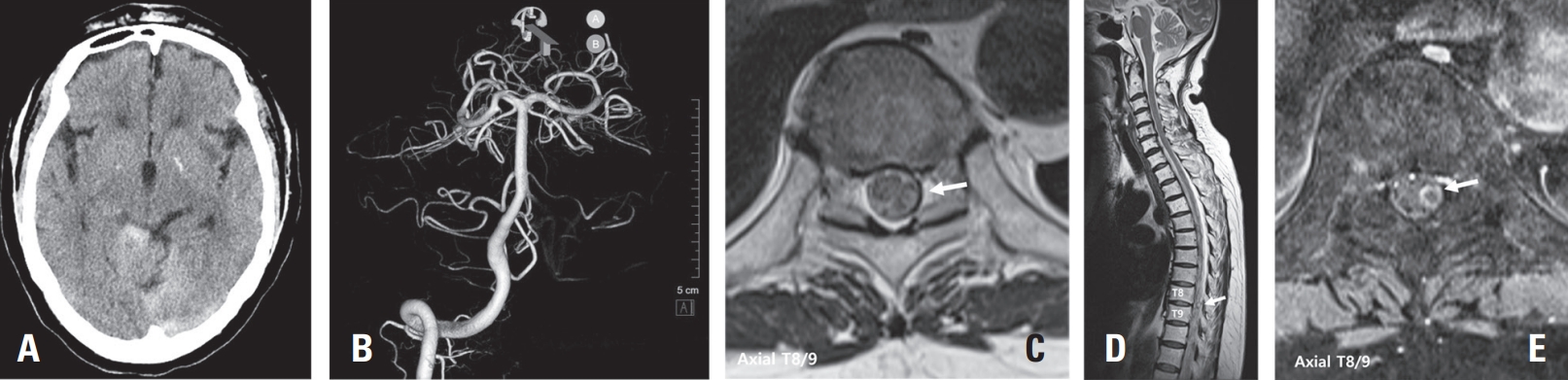
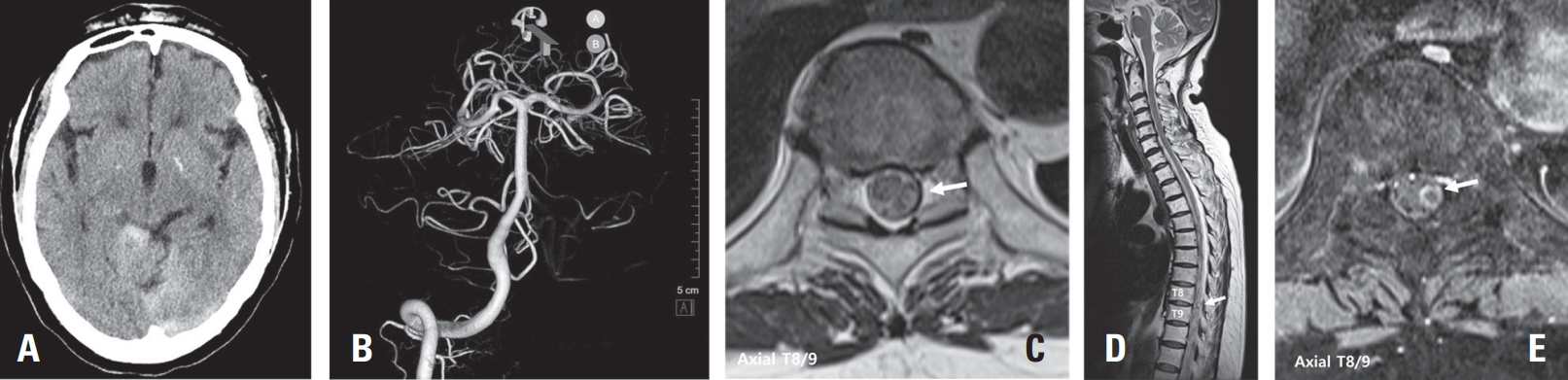
A 71-year-old female patient presented to a local clinic with sudden onset headache and back pain on the day of admission. A brain computed tomography (CT) scan performed at the local clinic diagnosed subarachnoid hemorrhage (SAH) in the basal cistern (Fig. 1A). 3-dimention CT brain angiography was conducted but failed to identify the source of the hemorrhage (Fig. 1B). Consequently, the patient was transferred to our hospital for further evaluation and management. Upon arrival, the patient complained of severe back pain. To investigate the potential spinal origin of the hemorrhage, a contrast-enhanced Magnetic Resonance Imaging (MRI) of the thoracic spine was performed. This revealed an abnormal intradural extramedullary heterogenous lesion located in the T8/9 level suspected as the source of bleeding (Fig. 1C, D, E). Immediately, spinal angiography of the thoracic spinal vascular lesion was performed. Spinal angiography revealed the fusiform aneurysm on a distal segment of a radiculopial artery of the left intercostal artery at left T9 (Fig 2A, B, C). However, the feeding artery was found to be too narrow, precluding endovascular procedures such as embolization.
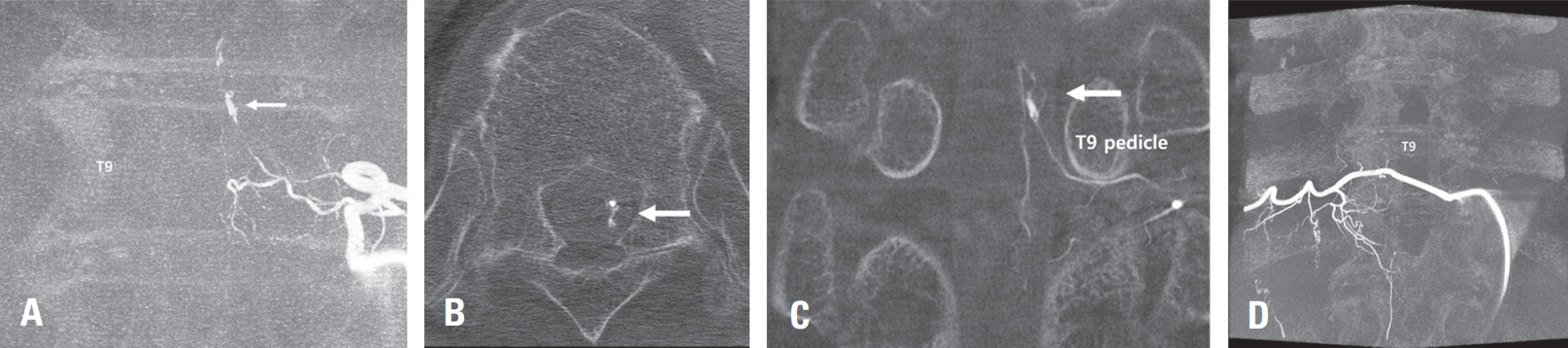
The patient then underwent surgical treatment on the subsequent day. Under general anesthesia, a total laminectomy was performed at thoracic levels 8 and 9, exposing the dura. After dural incision, a relatively small amount of subdural hematoma was identified, and a portion of it was removed. An acute bleeding focus was identified from the radicular artery beneath the left T9 nerve root. Following resection of the T9 root, the surrounding radicular artery was occluded with a clip for hemostasis. Postoperatively, the patient’s severe back pain significantly improved, and she was able to ambulate, leading to discharge in a walking state. Four weeks later, a follow-up Digital Subtraction Angiography (DSA) of the surgical site was performed, confirming the complete absence of the aneurysm (Fig. 2D).
2. Case II: Endovascular approach
A 75-year-old female patient presented with sudden onset back pain and paraplegia of both lower extremities. Upon admission, her mental status was alert, and she complained of severe back pain. Due to the intensity of her symptoms, a contrast-enhanced MRI of the thoracic spine was immediately performed. The MRI finding
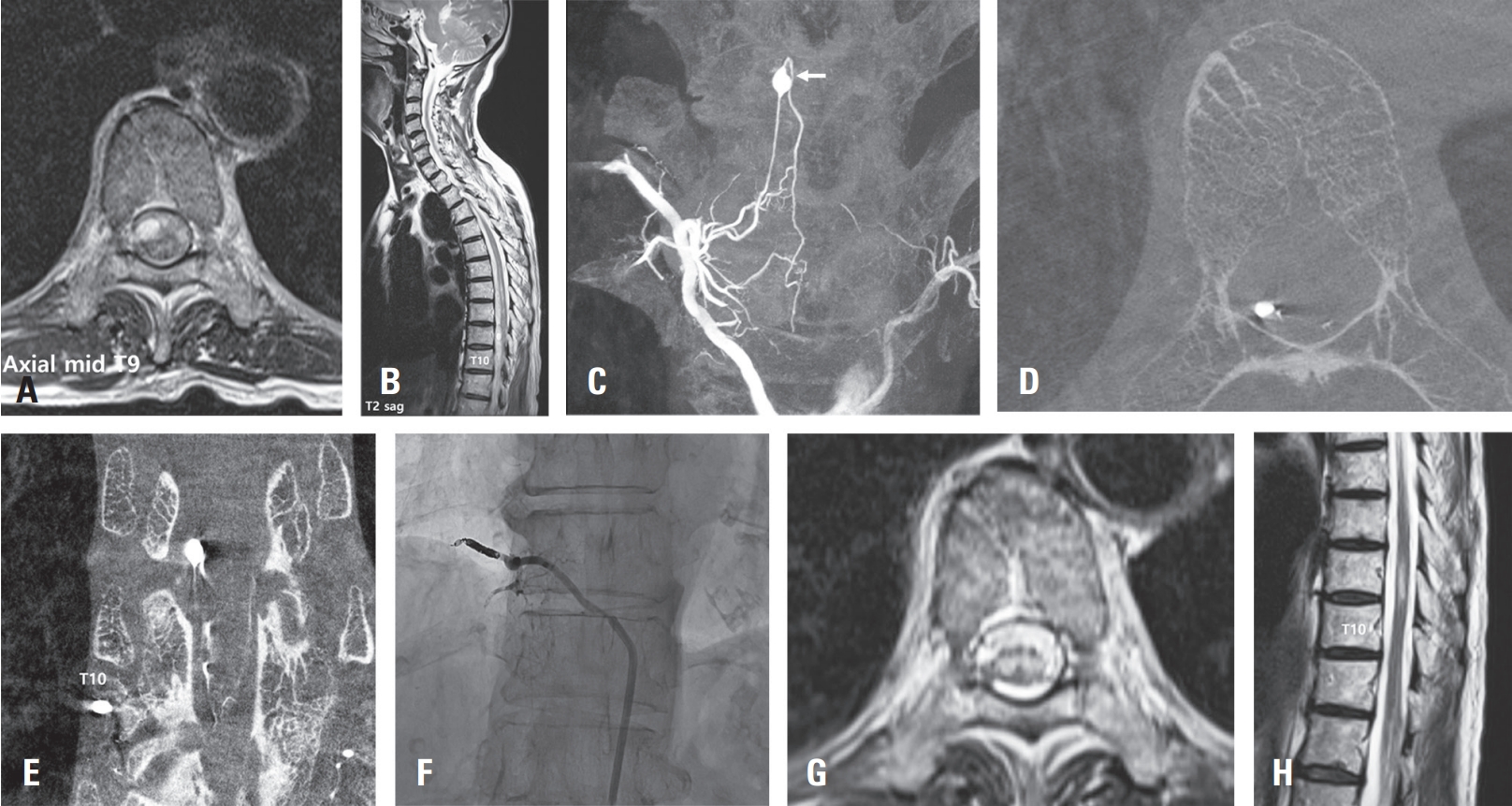
revealed a subdural hematoma extending from the C6 to T11 level, with evidence of spinal cord compression. On the contrast-enhanced images, a heterogeneously enhancing mass was observed at the T9 level of the thoracic spine (Fig 3A, B). Further spinal angiographic examination revealed a aneurysm originating from the right T10 radicular artery (Fig 3C, D, E). As a catheter could be advanced into the parent artery and considering the severe neurological deficit, an immediate embolization procedure was decided upon. The catheter was positioned in the proximal intercostal artery at the T10 level, and the aneurysm was occluded using a combination of glue and coils at the proximal radiculopial artery (Fig 3F). Three weeks after the procedure, a follow-up MRI scan showed resorption of the subdural hematoma; however, the paraplegia demonstrated no neurological improvement (Fig 3G, H).
Discussion
SAAs represent an exceptionally rare and challenging subset of neurovascular pathologies, characterized by their diverse etiologies, variable clinical presentations, and a lack of standardized management guidelines.1,8,11,12) The two cases presented herein underscore these complexities, illustrating the diagnostic dilemmas and the often-unpredictable outcomes associated with ruptured thoracic radicular artery aneurysms. Both patients presented with acute onset severe back pain and neurological deficits (bilateral leg weakness leading to paraplegia), typical manifestations of spinal subarachnoid or subdural hemorrhage, which can rapidly spread beyond the primary bleeding site.
The rarity of SAAs makes their diagnosis particularly challenging. As demonstrated in Case I, initial cerebral imaging (Brain CT and 3D CT brain angiography) often fails to identify the source of hemorrhage, necessitating a high index of suspicion for spinal etiologies in cases of unexplained SAH, especially when accompanied by back pain. Spinal MRI, particularly with contrast enhancement, plays a crucial role in localizing hematomas and identifying potential vascular abnormalities within the spinal canal. However, due to the small size of these lesions, definitive diagnosis frequently relies on DSA, which remains the gold standard for visualizing the intricate spinal arterial anatomy and precisely identifying the aneurysm.
SAAs can arise from diverse etiologies, including circulatory factors3,7,15)(e.g., arteriovenous malformations, pregnancy, intraspinal neoplasms, coarctation of the aorta, moyamoya disease) and arterial wall factors4)(e.g., collagen vascular diseases, inflammatory vasculopathy). A significant number are idiopathic or isolated, often presenting as small (<3mm) dissecting aneurysms without a distinct neck, typically originating where radiculomedullary or radiculopial arteries pierce the dura in the thoracic region.12)
The management of SAAs is highly individualized, reflecting the absence of a broad consensus on optimal treatment.1,12,14) Current strategies often depend on the presumed etiology. SAAs attributed to circulatory factors (e.g., AVMs) are considered to have a high risk of rupture due to increased blood flow, and treatment of the underlying cause may lead to aneurysm regression.2,10) Aneurysms arising from arterial wall factors may be fragile and prone to dilatation even without significant flow alterations, with medical treatment sometimes leading to resolution. For idiopathic or isolated SAAs, especially dissecting aneurysms of small vessels like radiculopial or radiculomedullary arteries, options range from observation (as spontaneous occlusion/healing can occur without sacrificing the parent artery) to aggressive intervention.9)
Our two cases illustrate the therapeutic dilemma. In Case I, a 71-year-old female with a ruptured left T9 radicular artery aneurysm presented with bilateral leg weakness and severe back pain. Despite the feeding artery being too narrow for endovascular embolization, successful surgical ligation of the feeding artery and partial evacuation of the subdural hematoma led to significant symptomatic improvement and neurological preservation. The follow-up DSA confirmed complete obliteration of the aneurysm. This outcome highlights that surgical intervention can be a highly effective treatment, particularly when endovascular options are limited or when there is a significant mass effect from hematoma.
Conversely, Case II involved a 75-year-old female with paraplegia due to a ruptured right T10 radicular artery aneurysm, complicated by an extensive subdural hematoma and spinal cord compression. Endovascular embolization with glue and coils was performed due to the severe neurological deficit and catheter accessibility. While the subdural hematoma showed resorption on follow-up MRI, the patient’s paraplegia did not improve neurologically. This unfortunate outcome underscores the potential for irreversible neurological damage following spinal cord injury from hemorrhage, even with successful aneurysm occlusion. It also suggests that the timing of intervention, the extent of initial neurological compromise, and the location of the aneurysm relative to critical spinal cord supply arteries (e.g., dominant radiculomedullary arteries, which can cause ischemia if occluded) are crucial prognostic factors.
In conclusion, these cases reinforce the existing understanding that ruptured thoracic radicular artery aneurysms are challenging to diagnose and manage. While surgical and endovascular approaches can successfully treat the vascular lesion, neurological outcomes remain highly variable, particularly in cases of significant initial neurological deficit. The experience from these cases further supports the notion that surgical intervention may be indicated in cases of mass effect, significant neurological deficit, progressive neurological decline, or failure of conservative/endovascular treatment. Further accumulation of detailed case reports and multicenter studies is crucial to better understand the natural history, optimize diagnostic algorithms, and establish evidence-based treatment guidelines for these rare and complex spinal vascular anomalies.
Conclusions
Ruptured thoracic radicular artery aneurysms are rare but can lead to severe neurological symptoms. The two cases presented herein demonstrate the diverse clinical manifestations and treatment outcomes of this condition, emphasizing the importance of accurate diagnosis and timely intervention. However, a unified guideline for the management of spinal artery aneurysms is still lacking, necessitating careful treatment decisions based on each patient’s unique clinical characteristics and neurological status.
Fig. 1.
(A) brain CT scan showing subarachnoid hemorrhage in the basal cisterns. It indicates acute bleeding. (B) 3-dimention reconstruction of CT brain angiography revealing no obvious aneurysmal source of hemorrhage in the cerebral vasculature. (C) Axial T2-weighted MRI at the T8/9 level. This image showing the intradural mass of heterogenous signal intensity in the spinal cord and surrounding structures (arrow). (D) Sagittal T2-weighted MRI of the thoracic spine showing extensive subdural hematoma extending from T1 to S1 level and a mass causing spinal cord compression at the T8/9 level (arrow). (E) Axial T1-weighted post-contrast MRI at the T8/9 level. A focal rim-enhancing lesion in the left intradural or subarachnoid space of the thecal sac at the T8/9 level (arrow).
Fig. 2.
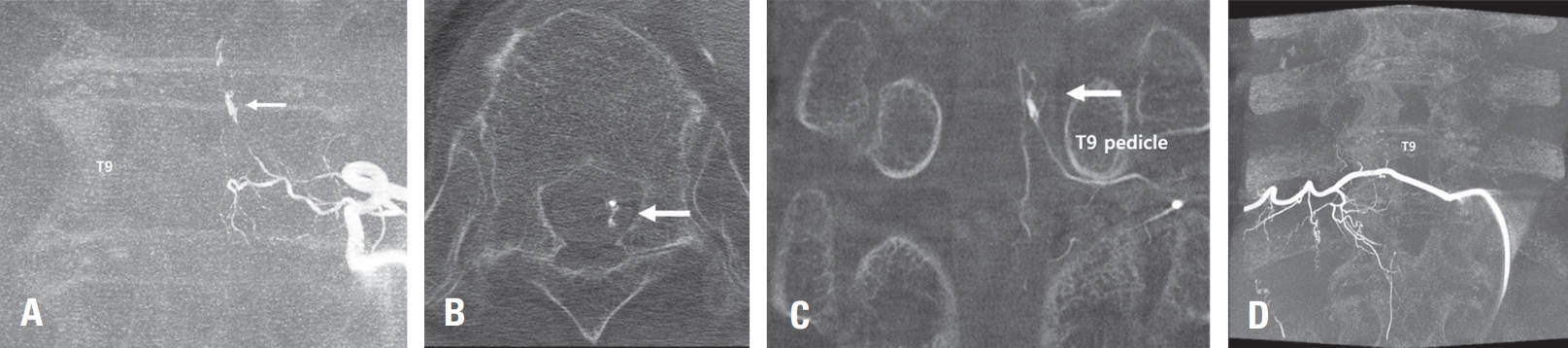
Angiogram of the left T9 intercostal artery in the left anterior oblique view showing a focal fusiform dissecting aneurysm in left T9 radiculopial artery (A, arrow). 3-dimention reconstruction of CT angiogram showing 2 mmx2.5 mm sized aneurysm and network of vessels in relation to left T9 pedicle (B, C, arrow). Followup angiography was performed after POD 4 weeks and confirmed the non-visualization of aneurysm sac and feeding artery from left T9 radiculopial artery the complete absence of the aneurysm (D).
Fig. 3.
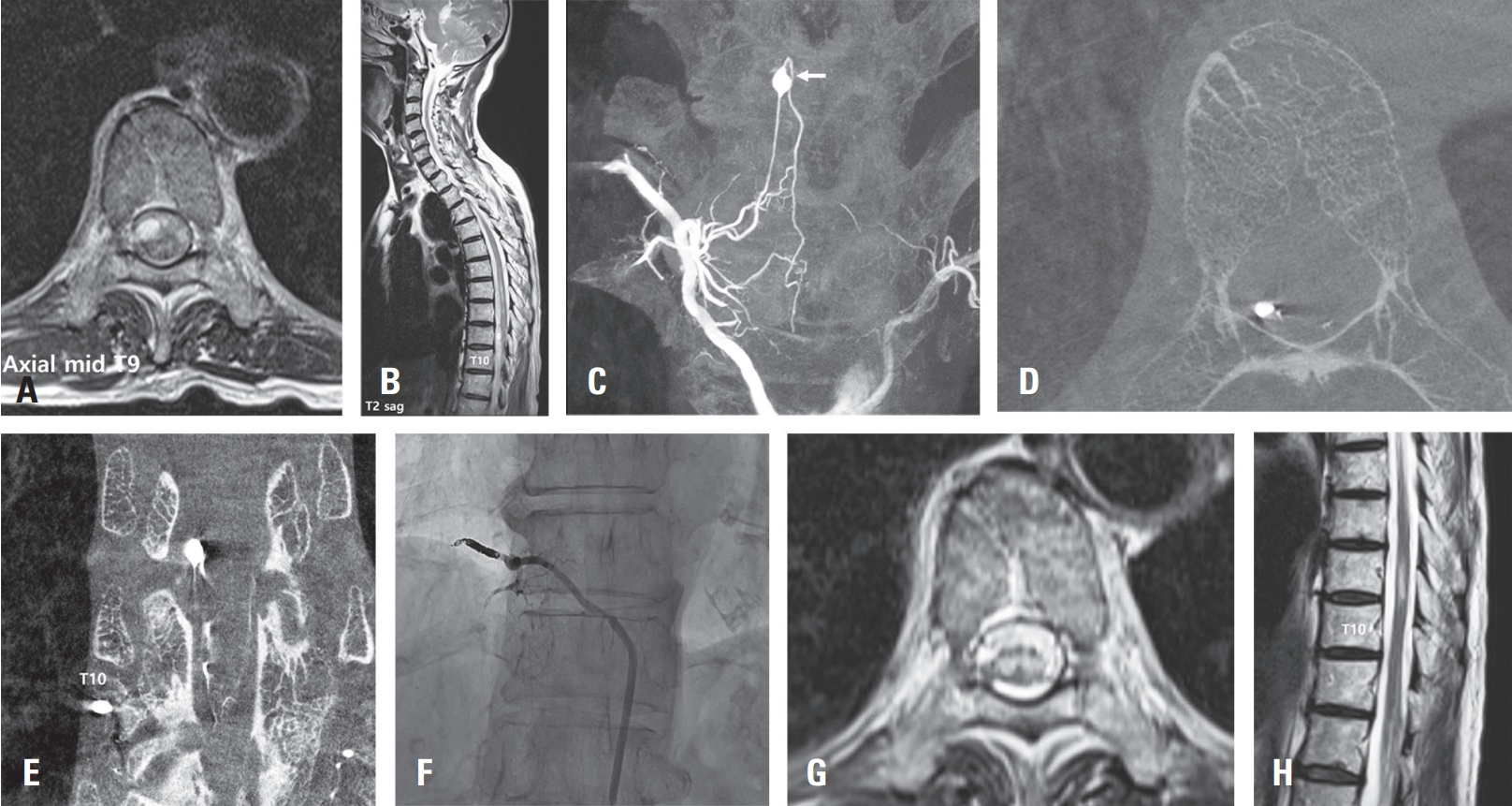
Initial T2 weighted MRI showing a large amount of subdural hematoma extending from C6 to T11, along with evidence of spinal cord edema due to neural compression (A, B). Spinal angiogram image showing a saccular aneurysm in the right T10 radiculopial artery, which was identified as the ruptured aneurysm (C, arrow). CT reconstruction image of spinal angiogram showing the anatomical position of spinal aneurysm (D, E). Intraoperative angiogram image showing catheter position and embolization materials (coil and glue) used to occlude the aneurysm (F). Follow-up MRI at three weeks post-procedure demonstrating resorption of subdural hematoma and persistent T2 hyperintensity in the spinal cord at T9/10 level, suggestive of sequelae of compressive myelopathy (G, H).
References
1. Abdalkader M, Samuelsen BT, Moore JM, Cervantes-Arslanian A, Ong CJ, Setty BN, et al. Ruptured spinal aneurysms: diagnosis and management paradigms. World Neurosurgery 2021;146:e368-e77.
2. Alomari S, Xu R, Huang J, Tamargo R, Bydon A, et al. Isolated aneurysms of the spinal circulation: a systematic review of the literature. Neurosurgical Review 2022;1-20.
3. Aoun SG, El Ahmadieh TY, Soltanolkotabi M, Ansari SA, Marden FA, Batjer HH, et al. Ruptured spinal artery aneurysm associated with coarctation of the aorta. World Neurosurg 2014;81:441 e417-22.
4. Bahar S, Coban O, Gurvit IH, Akman-Demir G, Gokyigit A. Spontaneous dissection of the extracranial vertebral artery with spinal subarachnoid haemorrhage in a patient with Behcet’s disease. Neuroradiology 1993;35:352-4.
5. Berlis A, Scheufler KM, Schmahl C, Rauer S, Götz F, Schumacher M. Solitary spinal artery aneurysms as a rare source of spinal subarachnoid hemorrhage:: Potential etiology and treatment strategy. American Journal of Neuroradiology 2005;26:405-10.
6. Chen CC, Bellon RJ, Ogilvy CS, Putman CM. Aneurysms of the lateral spinal artery: report of two cases. Neurosurgery 48:949-53. discussion. 2001;953-944.
9. Harapan BN, Forbrig R, Liebig T, Schichor C, Thorsteinsdottir J. Diagnostic and Therapeutic Approaches for Spinal Subarachnoid Hemorrhage Due to Spinal Aneurysms and Other Etiologies. J Clin Med 2025;14.
10. Madhugiri VS, Ambekar S, Kumar VRR, Sasidharan GM, Nanda A. Spinal aneurysms: clinicoradiological features and management paradigms A systematic review. Journal of Neurosurgery-Spine 2013;19:34-48.
11. Massand MG, Wallace RC, Gonzalez LF, Zabramski JM, Spetzler RF. Subarachnoid hemorrhage due to isolated spinal artery aneurysm in four patients. American Journal of Neuroradiology 2005;26:2415-9.
12. McGuire LS, Fuentes A, Charbel FT, Alaraj A, Amin-Hanjani S. Ruptured isolated spinal artery aneurysms: Case series of five patients and a review of the literature on management strategies. Interventional Neuroradiology 2023;15910199221149562.
13. Nogueira RG, Kasper E, Walcott BP, Nahed BV, Redjal N, Coumans J-V, et al. Lateral sacral artery aneurysm of the lumbar spine: hemorrhage resulting in cauda equina syndrome. Journal of NeuroInterventional Surgery 2010;2:399-401.
Rupture of Thoracic Radicular Artery Aneurysm Presenting with Subdural Hematoma and Subarachnoid Hemorrhage: Two Case Reports
Fig. 1. (A) brain CT scan showing subarachnoid hemorrhage in the basal cisterns. It indicates acute bleeding. (B) 3-dimention reconstruction of CT brain angiography revealing no obvious aneurysmal source of hemorrhage in the cerebral vasculature. (C) Axial T2-weighted MRI at the T8/9 level. This image showing the intradural mass of heterogenous signal intensity in the spinal cord and surrounding structures (arrow). (D) Sagittal T2-weighted MRI of the thoracic spine showing extensive subdural hematoma extending from T1 to S1 level and a mass causing spinal cord compression at the T8/9 level (arrow). (E) Axial T1-weighted post-contrast MRI at the T8/9 level. A focal rim-enhancing lesion in the left intradural or subarachnoid space of the thecal sac at the T8/9 level (arrow).
Fig. 2. Angiogram of the left T9 intercostal artery in the left anterior oblique view showing a focal fusiform dissecting aneurysm in left T9 radiculopial artery (A, arrow). 3-dimention reconstruction of CT angiogram showing 2 mmx2.5 mm sized aneurysm and network of vessels in relation to left T9 pedicle (B, C, arrow). Followup angiography was performed after POD 4 weeks and confirmed the non-visualization of aneurysm sac and feeding artery from left T9 radiculopial artery the complete absence of the aneurysm (D).
Fig. 3. Initial T2 weighted MRI showing a large amount of subdural hematoma extending from C6 to T11, along with evidence of spinal cord edema due to neural compression (A, B). Spinal angiogram image showing a saccular aneurysm in the right T10 radiculopial artery, which was identified as the ruptured aneurysm (C, arrow). CT reconstruction image of spinal angiogram showing the anatomical position of spinal aneurysm (D, E). Intraoperative angiogram image showing catheter position and embolization materials (coil and glue) used to occlude the aneurysm (F). Follow-up MRI at three weeks post-procedure demonstrating resorption of subdural hematoma and persistent T2 hyperintensity in the spinal cord at T9/10 level, suggestive of sequelae of compressive myelopathy (G, H).
Fig. 1.
Fig. 2.
Fig. 3.
Rupture of Thoracic Radicular Artery Aneurysm Presenting with Subdural Hematoma and Subarachnoid Hemorrhage: Two Case Reports