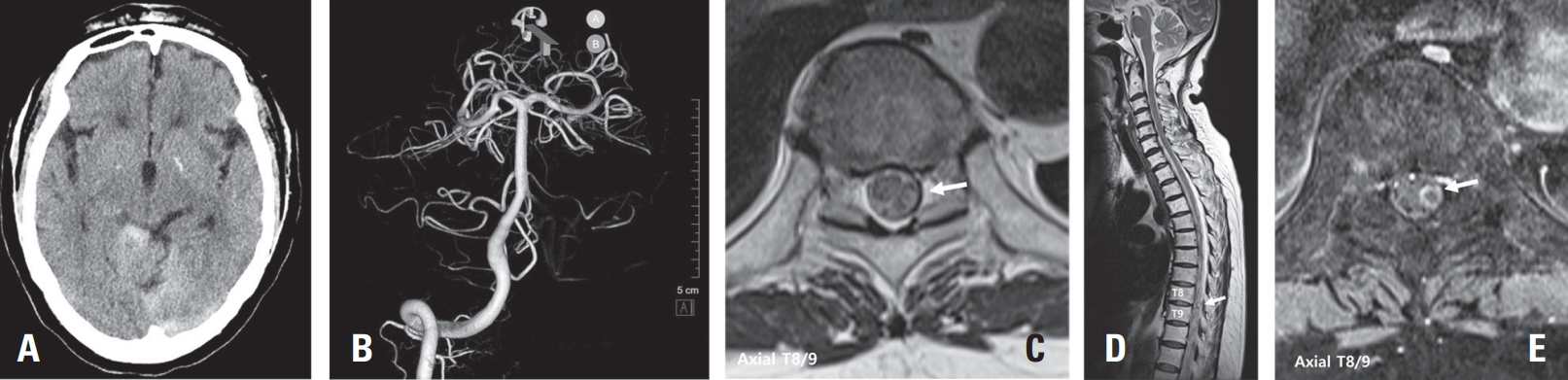
Spinal artery aneurysms are exceedingly rare, and their natural history remains poorly understood. Diagnosis can be challenging due to their small size and the difficulty in detection by MR angiography (MRA) or CT angiography (CTA); Digital Subtraction Angiography (DSA) is considered the gold standard diagnostic tool. This case report presents two cases of ruptured thoracic radicular artery aneurysms leading to subdural hematoma (SDH) and subarachnoid hemorrhage (SAH). The first patient, a 71-year-old female, presented with bilateral leg weakness, headache, and severe back pain, where multiple fusiform dilatations of the left T9 radiculopial artery were identified. She showed significant improvement after surgical intervention. The second patient, a 75-year-old female, presented with paraplegia and severe back pain, and a saccular dilatation in the right T10 radiculopial artery was found. She underwent endovascular embolization but showed no neurological improvement. These cases highlight the diverse clinical presentations, diagnostic challenges, and uncertainties in management strategies for ruptured spinal artery aneurysms, emphasizing the need for prompt intervention, especially in cases with significant or progressive neurological deficits.
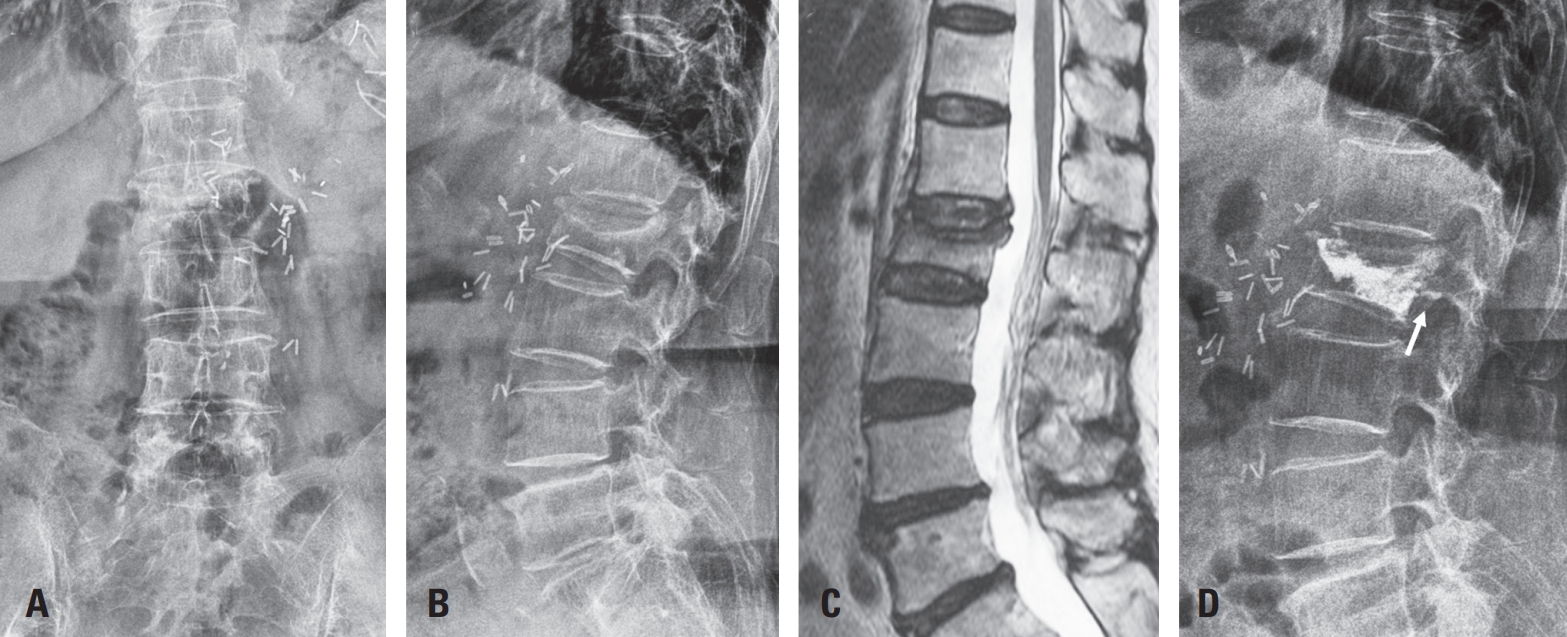
Vertebroplasty or kyphoplasty is a widely accepted minimally invasive procedure for treating painful vertebral compression fractures. Although considered safe, rare but serious complications such as spinal subdural hematoma (SDH) can occur, particularly in patients receiving long-term anticoagulation therapy. We present a rare case of spinal SDH following kyphoplasty in a 78-year-old woman with a mechanical aortic valve on chronic warfarin therapy. Anticoagulation was managed perioperatively with warfarin discontinuation and bridging enoxaparin. Postoperative X-ray showed subtle posterior cement leakage. MRI on postoperative day 1 revealed lumbar SDH, which progressed cranially by day 2. The patient remained neurologically intact and was treated conservatively with corticosteroids and temporary suspension of anticoagulation. Follow-up imaging showed gradual hematoma resolution, and she was discharged without deficits. This case suggests the importance of maintaining a high index of suspicion for spinal hematoma in anticoagulated patients, especially when new symptoms or even minor cement leakage are present. Careful perioperative planning, including early imaging and multidisciplinary management, is crucial in such high-risk patients.

 First
First Prev
Prev

