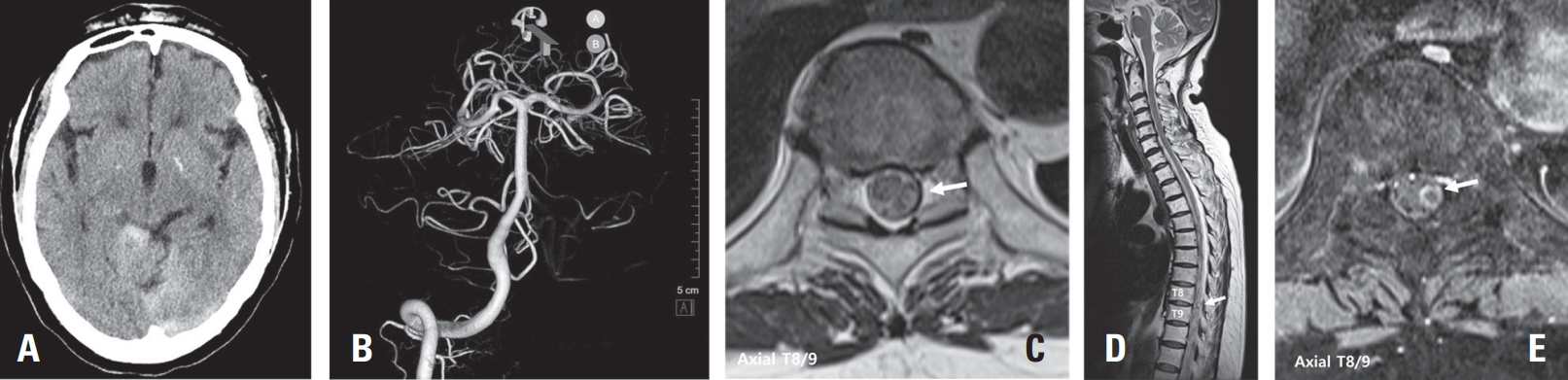
Spinal artery aneurysms are exceedingly rare, and their natural history remains poorly understood. Diagnosis can be challenging due to their small size and the difficulty in detection by MR angiography (MRA) or CT angiography (CTA); Digital Subtraction Angiography (DSA) is considered the gold standard diagnostic tool. This case report presents two cases of ruptured thoracic radicular artery aneurysms leading to subdural hematoma (SDH) and subarachnoid hemorrhage (SAH). The first patient, a 71-year-old female, presented with bilateral leg weakness, headache, and severe back pain, where multiple fusiform dilatations of the left T9 radiculopial artery were identified. She showed significant improvement after surgical intervention. The second patient, a 75-year-old female, presented with paraplegia and severe back pain, and a saccular dilatation in the right T10 radiculopial artery was found. She underwent endovascular embolization but showed no neurological improvement. These cases highlight the diverse clinical presentations, diagnostic challenges, and uncertainties in management strategies for ruptured spinal artery aneurysms, emphasizing the need for prompt intervention, especially in cases with significant or progressive neurological deficits.
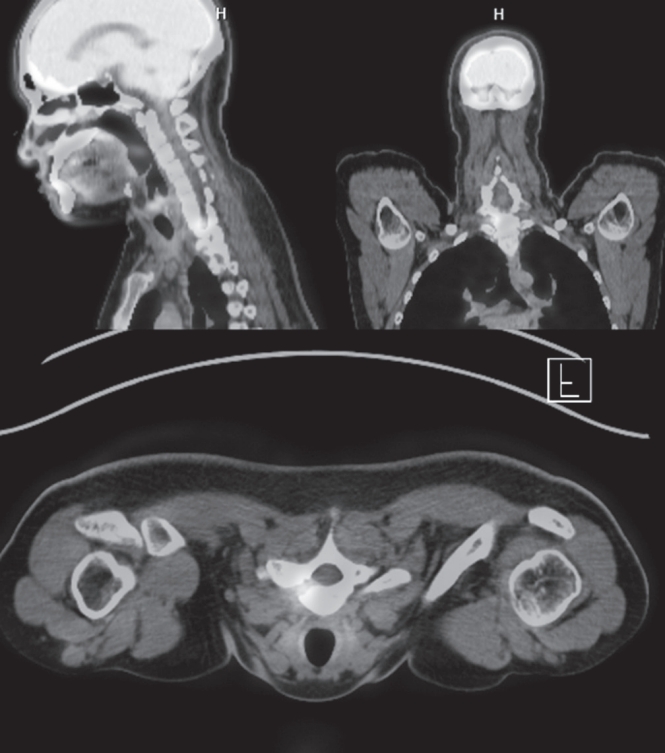
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.

 First
First Prev
Prev

