Study Design This study was a retrospective single-center cohort study.
Purpose This study aimed to compare long-term shunt patency by shunt type (syringo-subarachnoid [SS], syringo-pleural [SP], syringo-peritoneal [SPt]) and disease etiology (post-traumatic, post-infectious, idiopathic) in patients surgically treated for syringomyelia, using Kaplan-Meier survival methodology.
Overview of Literature: Syringomyelia shunting carries a well-documented revision burden, but direct comparative survival data across shunt modalities and etiologic subgroups are scarce, particularly from East Asian centers.
Methods We retrospectively analyzed 42 patients (mean age, 47.6±11.8 years; 57.1% male) who underwent syringomyelia shunting at a tertiary neurosurgical center (January 2000–December 2020) with ≥12 months follow-up. Shunt type was classified as SS (n=12), SP (n=16), or SPt (n=14); etiology as post-traumatic (n=24), post-infectious (n=10), idiopathic (n=6), or hemorrhage/tumor-related (n=2). The primary endpoint was shunt revision surgery. Kaplan-Meier analysis, log-rank testing, and Cox proportional hazards regression were performed.
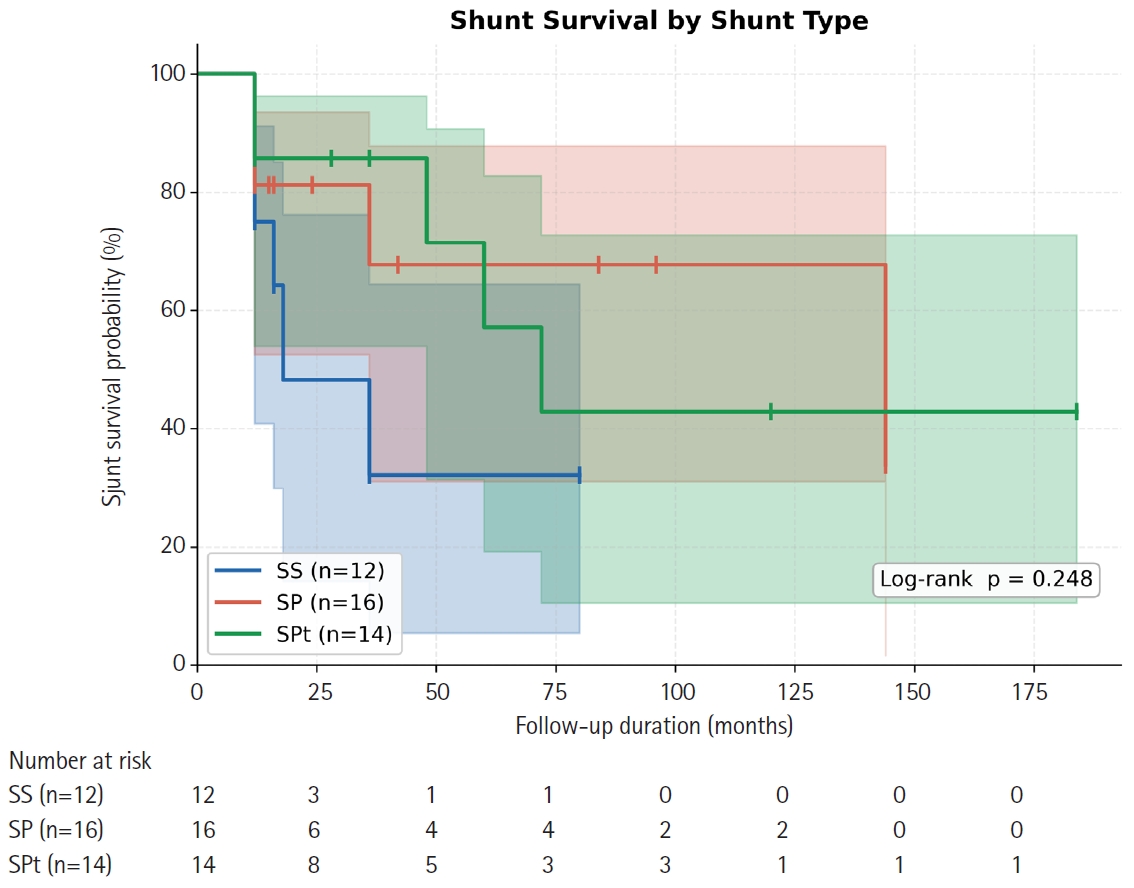
Results Over a median follow-up of 15 months (range, 12 to 184 months), 16 patients (38.1%) underwent shunt revision. Overall 12- and 24-month patency rates were 79.6% and 72.5%, respectively (median shunt survival 72 months). By shunt type, 12-month patency was 75.0% (SS), 81.3% (SP), and 85.7% (SPt); 24-month patency declined to 48.2% for SS while SP and SPt remained at 81.3% and 85.7% (log-rank p=0.248). Post-infectious syringomyelia showed the shortest median shunt survival (36 months) compared with post-traumatic (not reached) and idiopathic (not reached) groups (log-rank p=0.232). No independent predictor of shunt failure was identified on multivariate Cox regression.
Conclusion All three shunting techniques achieve approximately 80% one-year patency. SS may carry a higher long-term occlusion risk. Post-infectious syringomyelia requires closer postoperative surveillance. Larger prospective studies are needed to establish definitive shunt selection criteria.
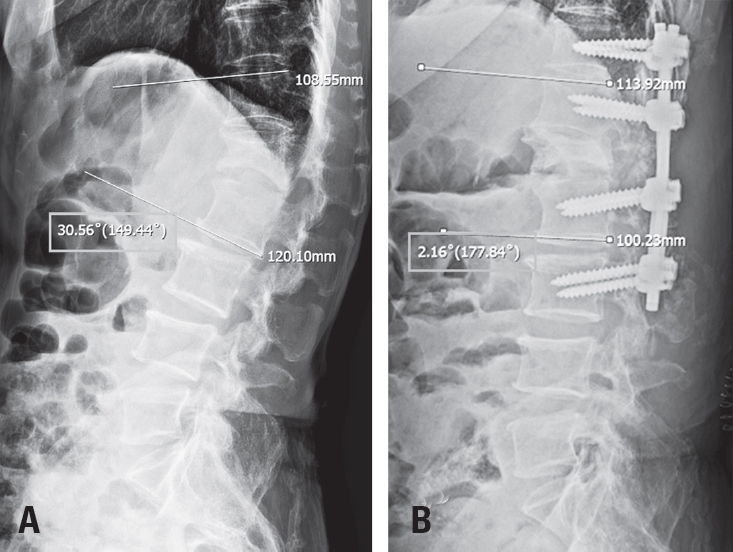
Tethered cord syndrome (TCS) is a condition in which the spinal cord becomes pathologically stretched due to various congenital or acquired etiologies, leading to progressive neurological symptoms. While surgical detethering is the gold standard for pediatric patients, adult-onset recurrent TCS presents a significant surgical challenge. Reoperation carries substantial risks—including spinal cord injury, cerebrospinal fluid leakage, and a high rate of retethering—often resulting in suboptimal long-term outcomes. Recently, spine-shortening osteotomy (SSO) has emerged as an alternative technique to reduce spinal cord tension without direct manipulation of the neural elements. Here, we report a case of recurrent adult TCS associated with a lipomyelomeningocele, which was exacerbated by post-traumatic kyphosis from an L1 compression fracture. The patient was successfully treated with SSO at the L1 level. This case highlights the utility of SSO as a safe and effective alternative to conventional revision detethering, particularly in complex cases involving spinal deformity.

 First
First Prev
Prev

