Department of Neurosurgery, Spine and Spinal Cord Institute, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
Corresponding author: Hyun-Jun Jang, M.D. Department of Neurosurgery, Spine and Spinal Cord Institute, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul 06273, Korea TEL: +82-2-2019-2114, FAX: +82-2-3461-9229 E-mail: janghj0@yuhs.ac
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Tethered cord syndrome (TCS) is a condition in which the spinal cord becomes pathologically stretched due to various congenital or acquired etiologies, leading to progressive neurological symptoms. While surgical detethering is the gold standard for pediatric patients, adult-onset recurrent TCS presents a significant surgical challenge. Reoperation carries substantial risks—including spinal cord injury, cerebrospinal fluid leakage, and a high rate of retethering—often resulting in suboptimal long-term outcomes. Recently, spine-shortening osteotomy (SSO) has emerged as an alternative technique to reduce spinal cord tension without direct manipulation of the neural elements. Here, we report a case of recurrent adult TCS associated with a lipomyelomeningocele, which was exacerbated by post-traumatic kyphosis from an L1 compression fracture. The patient was successfully treated with SSO at the L1 level. This case highlights the utility of SSO as a safe and effective alternative to conventional revision detethering, particularly in complex cases involving spinal deformity.
계류척수 증후군(Tethered cord syndrome, TCS)은 다양한 선천적 또는 후천적 원인으로 인해 척수가 병적으로 신장되어 점진적인 신경학적 증상을 유발하는 질환입니다. 소아 환자에서는 수술적 박리술(Surgical detethering)이 표준 치료법(Gold standard)으로 간주되지만, 성인기에 발생한 재발성 TCS는 수술적으로 매우 까다로운 과제입니다. 재수술은 척수 손상, 뇌척수액 유출, 높은 재유착률 등 상당한 위험을 수반하며, 종종 장기적으로 만족스럽지 못한 결과를 초래합니다. 최근 신경 조직을 직접 조작하지 않고도 척수의 긴장을 완화할 수 있는 대안적 기법으로 척추 단축 절골술(Spine-shortening osteotomy, SSO)이 부상하고 있습니다. 본 논문에서는 지방수막척수류(Lipomyelomeningocele)와 관련된 성인 재발성 TCS 환자가 L1 압박 골절로 인한 외상 후 후만증에 의해 증상이 악화된 증례를 보고합니다. 해당 환자는 L1 분절에서 SSO를 시행하여 성공적으로 치료되었습니다. 본 증례는 특히 척추 변형을 동반한 복잡한 사례에서 SSO가 기존의 재교정 박리술을 대체할 수 있는 안전하고 효과적인 선택지임을 시사합니다.
Tethered cord syndrome (TCS) is a clinical condition characterized by pathological stretching of the spinal cord due to congenital or acquired etiologies, resulting in progressive neurological deficits.1) Congenital causes typically involve spinal dysraphism, such as fatty filum terminale, lipomyelomeningocele, or split cord malformation. Acquired tethering often results from postoperative scarring, arachnoiditis, or trauma.2,3)
In pediatric patients, the pathophysiology is driven by the discrepancy between spinal column growth and spinal cord ascent. Early surgical detethering is effective and carries a relatively low complication rate.4) However, the management of adult TCS, particularly recurrent cases, is controversial and challenging. Adult patients frequently present with dense adhesions and altered anatomy from prior surgeries. Complete detethering in these cases is technically demanding and poses significant risks of iatrogenic spinal cord injury and dural tears. Furthermore, symptomatic retethering is common, rendering standard detethering insufficient for definitive treatment in many adults.5)
To address these challenges, spine-shortening osteotomy (SSO) has been introduced as an alternative strategy. This technique aims to reduce longitudinal tension on the neural elements by shortening the spinal column, thereby avoiding the need for extensive intradural dissection.6,7) In this report, we present a case of recurrent adult TCS associated with a lipomyelomeningocele that was exacerbated by a traumatic L1 compression fracture. The patient was successfully managed with SSO, which simultaneously addressed the neural tension and the kyphotic deformity.
Case Presentation
A 74-year-old man presented with a two-month history of bowel dysfunction, progressive right leg weakness, and worsening left leg weakness. His medical history included chronic obstructive pulmonary disease, benign prostatic hyperplasia, and osteoporosis. According to history taking, he had noted dragging of the right foot since his mid-30s and subsequently underwent detethering surgery in Belgium for a suspected spina bifida aperta with meningomyelocele. Despite surgery, right leg weakness persisted, particularly involving ankle dorsiflexion, for which he required an ankle– foot orthosis. In his mid-40s, he developed urinary retention necessitating clean intermittent catheterization, and approximately one year prior to presentation, left leg weakness progressed to the extent that he required a cane for ambulation. Three months prior to admission, the patient sustained a fall and was diagnosed with an L1 compression fracture. Following this trauma, his neurological status deteriorated rapidly. We hypothesized that the pre-existing tethered cord was exacerbated by the traumatic L1 compression fracture. The resulting worsening of the kyphotic deformity likely increased the longitudinal tension on the spinal cord (bowstring effect), contributing to the acute aggravation of bowel dysfunction and bilateral lower extremity weakness.
Plain radiographs demonstrated an L1 compression fracture with focal kyphosis. Magnetic resonance imaging (MRI) revealed findings consistent with TCS associated with a lipomyelomeningocele, along with the L1 compression fracture (Fig. 1). Preoperative electrodiagnostic studies showed the bilateral absence of H-reflexes in the tibial nerves and prolonged P40 latency on tibial somatosensory evoked potentials (SSEP), consistent with myelopathy.
1. Surgical procedure
Given the recurrent nature of the tethering and the concomitant kyphotic deformity, we opted for a SSO at the L1 level rather than revision detethering. The procedure utilized a technique similar to a pedicle subtraction osteotomy (PSO) or posterior vertebral column resection (PVCR).
Under general anesthesia, the patient was positioned prone. A midline incision was made exposing the spinous processes from T10 to L3. Intraoperative neuromonitoring (IONM), including motor evoked potentials (MEP), SSEP, and free-run electromyography (EMG), was utilized throughout the procedure to monitor neural integrity, especially during the shortening maneuver.
Subperiosteal dissection was performed to expose the transverse processes from T11 to L3. Bilateral pedicle screws were placed from T11 to L3. To minimize the risk of spinal cord compression from dural buckling following shortening, a wide laminectomy was performed from T12 to L2. The ligamentum flavum was excised, and a partial medial facetectomy was performed using a Kerrison rongeur.
Subsequently, total facetectomies were performed at T12/L1 and L1/L2, and both L1 transverse processes were excised. The L1 pedicles were removed bilaterally, sparing only a thin rim of the lower margin. The T12/L1 disc space was exposed bilaterally, and the lateral and ventral aspects of the L1 vertebral body were carefully dissected. A total discectomy of T12/L1 was performed, including the removal of the posterior longitudinal ligament (PLL). The cartilaginous endplate of the inferior T12 body was removed.
An osteotomy was performed on the L1 vertebral body parallel to the T12 lower endplate. A temporary rod was placed, and under strict IONM surveillance, the spinal column was gradually shortened by compressing the pedicle screws (Fig. 2). This maneuver brought the T12 lower endplate into contact with the osteotomized surface of the L1 body. Approximately 20 mm of shortening was achieved. Permanent rods were secured, and posterolateral fusion was performed using local autograft (Fig. 3).
2. Postoperative clinical presentation
The patient tolerated the procedure well without any intraoperative adverse events or signal changes in IONM. Immediate postoperative plain radiographs demonstrated a reduction in local kyphosis by approximately 28 degrees and a decrease in the spinal column height of approximately 10 mm at the osteotomy site (Fig. 2). MRI obtained on postoperative day 2 revealed distinct interval relaxation of the spinal cord compared with preoperative images, indicating an effective release of longitudinal tension (Fig. 4).
Clinically, the patient experienced no new neurological deficits. The recently aggravated left leg weakness improved to Motor Grade III, while the chronic right leg weakness remained stable. The patient also reported subjective improvement in bowel sensation. Due to the chronicity of his bladder and bowel dysfunction, he was discharged to a rehabilitation facility for continued therapy and close outpatient follow-up.
Discussion
Recurrent TCS in adults poses a complex therapeutic dilemma. The primary goal of surgery is to relieve tension on the spinal cord to prevent further neurological deterioration and alleviate pain. However, revision detethering is notoriously associated with high complication rates due to the loss of normal anatomical planes and the presence of dense arachnoid scarring.8-10) In this case, the patient presented with a unique “double-hit” pathology: a chronic congenital tethered cord exacerbated by an acute traumatic deformity. The L1 compression fracture introduced a kyphotic deformity, which increased the distance over the dorsal aspect of the spinal canal (the bowstring effect), thereby intensifying the tension on an already tethered cord.
We selected SSO over revision detethering for several compelling reasons. First, SSO avoids direct manipulation of the scarred neural interface. The safety profile of SSO compared to revision detethering has been highlighted in several studies. In a study by Lee et al. involving 60 adult patients undergoing revision detethering, the rate of woundrelated complications—including cerebrospinal fluid (CSF) leakage and infection—was reported to be as high as 22%, with 15% of patients experiencing CSF leaks specifically.8) Furthermore, neurological deterioration following revision detethering has been reported in approximately 3.3% to 11% of cases.11) In contrast, SSO has demonstrated superior perioperative safety regarding dural integrity and wound healing. Zhang et al. performed a preliminary comparison of perioperative outcomes between spinal column shortening (n=8) and revision detethering (n=8) for recurrent adult TCS. Remarkably, they reported 0% complications in the SSO group, whereas the revision detethering group had a 37.5% rate of wound-related complications (3 patients) and neurological worsening in 37.5% (3 patients).8) Similarly, a systematic review and meta-analysis by Lin et al., which included 57 patients treated with SSO, reported a pooled overall complication rate of only 6% (95% CI 0–17%), with a 0% rate of CSF-related complications.12) Second, SSO addresses the concomitant spinal deformity. By performing a shortening osteotomy at the level of the fracture (L1), we corrected the kyphosis and shortened the anterior column simultaneously. This creates a “slack” in the spinal cord, mimicking the effect of detethering without opening the dura.13) Another critical advantage of SSO is the durability of the outcome. The recurrence rate of retethering after traditional release is estimated to be between 5% and 50% due to the reformation of adhesions.14) However, Theodore et al. reported 0% recurrence of TCS symptoms in their series of 20 patients treated with SSO, with a mean follow-up of 23.3 months.15) These findings suggest that SSO not only reduces the immediate risks of dural tears and nerve injury associated with direct dissection but also provides a more definitive solution for preventing retethering. One technical consideration is the risk of dural buckling compressing the spinal cord after shortening. As demonstrated in our procedure, performing a wide laminectomy extending one level above and below the osteotomy site is crucial to accommodate the redundancy of the dura and prevent iatrogenic stenosis.13) While the technique requires expertise in deformity surgery and may involve greater blood loss than simple detethering, the literature and our experience suggest it provides a definitive and safer biomechanical solution for complex recurrent cases.
Conclusions
SSO as a safe and effective alternative for recurrent adult TCS exacerbated by spinal deformity. By simultaneously correcting kyphosis and relieving longitudinal tension via an extradural approach, SSO minimizes the risks of intradural dissection. Therefore, SSO should be considered a definitive surgical option for complex patients in whom traditional revision detethering poses prohibitive risks.
Fig. 1.
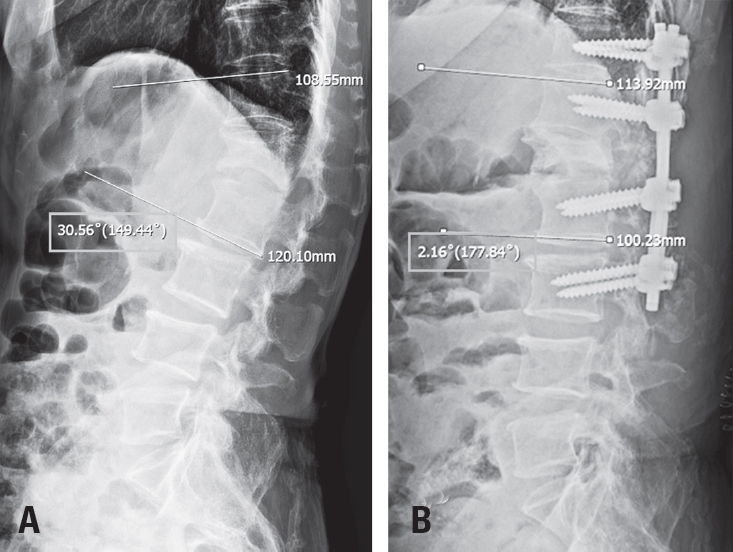
Pre-and post-operative plain radiography. (A) Preoperative plain radiography demonstrates a local kyphotic angle of 30° between T12 and L2. (B) Postoperative plain radiography shows a correction of the local kyphotic angle to lordotic 2° between T12 and L2. So, its change of the cobb angle between T12 and L2 was nearly 32°.
Fig. 2.
Intraoperative photographs demonstrating the gradual spinal shortening maneuver. (A) Partial compression between the T12 and L2 pedicle screws (approximately 50% closure). (B) Near-complete compression of the osteotomy site.
Fig. 3.
Preoperative and postoperative measurements of the L1 vertebral body. (A) The preoperative posterior height of the L1 vertebral body was approximately 31 mm. (B) Postoperatively, the height was reduced to 12 mm, indicating that a total spinal shortening of approximately 19 mm was achieved via the spinal shortening osteotomy.
Fig. 4.
Pre-and post-operative sagittal T2WI MR image. (A) The marked kyphosis between T12 and L2 results in visible stretching of the spinal cord. (B) After reduction of the T12–L2 kyphosis and lowering of the spinal column height, the spinal cord appears slightly loosened and less tensioned.
References
1. Phuong LK, Schoeberl KA, Raffel C. Natural history of tethered cord in patients with meningomyelocele. Neurosurgery 2002;50:989-95.
6. Kanno H, Aizawa T, Ozawa H, Hoshikawa T, Itoi E, Kokubun S. Spine-shortening vertebral osteotomy in a patient with tethered cord syndrome and a vertebral fracture. Case report. J Neurosurg Spine 2008;9:62-6.
7. Grande AW, Maher PC, Morgan CJ, et al. Vertebral column subtraction osteotomy for recurrent tethered cord syndrome in adults: a cadaveric study. J Neurosurg Spine 2006;4:478-84.
12. Lin W, Xu H, Duan G, et al. Spine-shortening osteotomy for patients with tethered cord syndrome: a systematic review and meta-analysis. Neurol Res 2018;40:340-63.
14. Samuels R, McGirt MJ, Attenello FJ, et al. Incidence of symptomatic retethering after surgical management of pediatric tethered cord syndrome with or without duraplasty. Childs Nerv Syst 2009;25:1085-9.
15. Theodore N, Cottrill E, Kalb S, et al. Posterior Vertebral Column Subtraction Osteotomy for Recurrent Tethered Cord Syndrome: A Multicenter, Retrospective Analysis. Neurosurgery 2021;88:637-47.
Spine-Shortening Osteotomy for Recurrent Adult Tethered Cord Syndrome Exacerbated by Traumatic Kyphosis: A Case Report
Fig. 1. Pre-and post-operative plain radiography. (A) Preoperative plain radiography demonstrates a local kyphotic angle of 30° between T12 and L2. (B) Postoperative plain radiography shows a correction of the local kyphotic angle to lordotic 2° between T12 and L2. So, its change of the cobb angle between T12 and L2 was nearly 32°.
Fig. 2. Intraoperative photographs demonstrating the gradual spinal shortening maneuver. (A) Partial compression between the T12 and L2 pedicle screws (approximately 50% closure). (B) Near-complete compression of the osteotomy site.
Fig. 3. Preoperative and postoperative measurements of the L1 vertebral body. (A) The preoperative posterior height of the L1 vertebral body was approximately 31 mm. (B) Postoperatively, the height was reduced to 12 mm, indicating that a total spinal shortening of approximately 19 mm was achieved via the spinal shortening osteotomy.
Fig. 4. Pre-and post-operative sagittal T2WI MR image. (A) The marked kyphosis between T12 and L2 results in visible stretching of the spinal cord. (B) After reduction of the T12–L2 kyphosis and lowering of the spinal column height, the spinal cord appears slightly loosened and less tensioned.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Spine-Shortening Osteotomy for Recurrent Adult Tethered Cord Syndrome Exacerbated by Traumatic Kyphosis: A Case Report