Department of Neurosurgery, Spine and Spinal Cord Institute, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
Corresponding author: Hyun-Jun Jang, M.D. Department of Neurosurgery, Spine and Spinal Cord Institute, Gangnam Severance Hospital, Yonsei University College of Medicine, 211 Eonju-ro, Gangnam-gu, Seoul 06273, Korea TEL: +82-2-2019-2114, FAX: +82-2-3461-9229, E-mail: janghj0@yuhs.ac
• Received: May 19, 2026 • Revised: June 9, 2026 • Accepted: June 10, 2026
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This study was a retrospective single-center cohort study.
Purpose
This study aimed to compare long-term shunt patency by shunt type (syringo-subarachnoid [SS], syringo-pleural [SP], syringo-peritoneal [SPt]) and disease etiology (post-traumatic, post-infectious, idiopathic) in patients surgically treated for syringomyelia, using Kaplan-Meier survival methodology.
Overview of Literature
Syringomyelia shunting carries a well-documented revision burden, but direct comparative survival data across shunt modalities and etiologic subgroups are scarce, particularly from East Asian centers.
Methods
We retrospectively analyzed 42 patients (mean age, 47.6±11.8 years; 57.1% male) who underwent syringomyelia shunting at a tertiary neurosurgical center (January 2000–December 2020) with ≥12 months follow-up. Shunt type was classified as SS (n=12), SP (n=16), or SPt (n=14); etiology as post-traumatic (n=24), post-infectious (n=10), idiopathic (n=6), or hemorrhage/tumor-related (n=2). The primary endpoint was shunt revision surgery. Kaplan-Meier analysis, log-rank testing, and Cox proportional hazards regression were performed.
Results
Over a median follow-up of 15 months (range, 12 to 184 months), 16 patients (38.1%) underwent shunt revision. Overall 12- and 24-month patency rates were 79.6% and 72.5%, respectively (median shunt survival 72 months). By shunt type, 12-month patency was 75.0% (SS), 81.3% (SP), and 85.7% (SPt); 24-month patency declined to 48.2% for SS while SP and SPt remained at 81.3% and 85.7% (log-rank p=0.248). Post-infectious syringomyelia showed the shortest median shunt survival (36 months) compared with post-traumatic (not reached) and idiopathic (not reached) groups (log-rank p=0.232). No independent predictor of shunt failure was identified on multivariate Cox regression.
Conclusion
All three shunting techniques achieve approximately 80% one-year patency. SS may carry a higher long-term occlusion risk. Post-infectious syringomyelia requires closer postoperative surveillance. Larger prospective studies are needed to establish definitive shunt selection criteria.
Syringomyelia is characterized by a longitudinal fluid-filled cavity (syrinx) within the spinal cord parenchyma that progressively compresses and destroys adjacent neural tissue. The clinical syndrome typically comprises dissociated sensory loss, wasting and weakness of the upper limbs, and—in advanced cases—spastic paraparesis and autonomic dysfunction.1,2) When conservative management fails or neurological deterioration progresses, surgical intervention is required.
The pathophysiology of syrinx formation differs substantially across etiologic categories. In post-traumatic syringomyelia, fibro-arachnoid scarring at the injury site generates abnormal intramedullary pressure gradients that drive fluid accumulation.3-5) In post-infectious cases—commonly following tuberculous or bacterial meningitis—diffuse spinal arachnoiditis produces widespread subarachnoid adhesions that impair cerebrospinal fluid (CSF) circulation.6-8) Idiopathic syringomyelia, by definition, lacks a clearly identified precipitant and often presents with a more indolent course.1)
Current surgical options for syringomyelia include three principal shunting strategies: (1) syringo-subarachnoid shunting (SS), which creates a direct communication between the syrinx and the adjacent subarachnoid space; (2) syringo-pleural shunting (SP), which diverts syrinx contents into the ipsilateral pleural cavity; and (3) syringo-peritoneal shunting (SPt), which drains fluid into the peritoneal cavity.9-12) Each technique exploits different pressure gradients and is subject to distinct failure mechanisms.
Published series on syringomyelia shunting are predominantly small and retrospective.9-11,13-15) Formal survival analyses using Kaplan-Meier methodology—the statistical standard for time-to-event outcomes—are rarely reported in this disease context, and comparative data from East Asian centers remain sparse.
The objectives of the present study were as follows: (1) to characterize overall long-term shunt patency in a single-center cohort; (2) to compare shunt survival across SS, SP, and SPt using Kaplan-Meier analysis; and (3) to evaluate whether disease etiology independently influences the risk of shunt revision.
Methods
This is a single-center, retrospective cohort study. The institutional surgical database was queried for all patients who underwent syringomyelia shunting between January 2000 and December 2020. Inclusion criteria were as follows: (1) radiologically confirmed syringomyelia on magnetic resonance imaging (MRI); (2) primary syrinx shunting procedure performed at our institution; and (3) minimum postoperative follow-up of 12 months. Patients who underwent adhesiolysis alone without shunt insertion, or whose primary surgical objective was tumor resection or Chiari malformation decompression without concomitant shunting, were excluded. The study was approved by the Institutional Review Board of Gangnam Severance Hospital, Yonsei University Health System (IRB No. 3-2022-0461) and individual informed consent was waived given the retrospective design.
1. Surgical technique and shunt classification
All procedures were performed by attending neurosurgeons with spinal subspecialty training. Shunt type was selected at the surgeon's discretion based on the degree of subarachnoid space involvement, prior surgical history, and intraoperative findings. Syringo-subarachnoid shunts were placed via a posterior midline approach, with a T-bar silastic catheter tunneled from the syrinx lumen into the adjacent subarachnoid space. Syringo-pleural and syringo-peritoneal shunts employed a valveless silastic catheter system with the proximal limb positioned within the syrinx cavity and the distal limb tunneled subcutaneously to the ipsilateral pleural cavity or peritoneal cavity, respectively.
2. Variable definitions
Disease etiology was classified as (1) post-traumatic, defined by documented spinal cord injury antedating syrinx development by ≥6 months;3,16,17) (2) post-infectious, defined by preceding meningitis, spinal cord infection, or tuberculous arachnoiditis confirmed by CSF analysis or imaging;8,9,18) (3) hemorrhage/tumor-related; or (4) idiopathic, when no identifiable underlying cause was found after complete workup. Spinal level was dichotomized as cervical (C1–C7) or thoracic (T1–T12).
The primary endpoint was shunt revision surgery, defined as any return to the operating room for shunt revision, replacement, or externalization necessitated by clinical deterioration (new or worsening neurological symptoms), with or without radiological re-expansion of the syrinx on MRI. Patients who completed follow-up without revision were censored at the date of last clinical contact.
3. Statistical analysis
Continuous variables are presented as mean±standard deviation or median with range; categorical variables as frequency and percentage. Shunt patency was estimated by the Kaplan-Meier product-limit method.19) Between-group differences in survival were assessed by the log-rank test for two-group comparisons and the multivariate log-rank test for three or more groups. Pairwise post-hoc comparisons were performed without adjustment for multiplicity given the exploratory nature of the analysis. Independent predictors of shunt failure were assessed using Cox proportional hazards regression20) with age (continuous), shunt type (ordinal: SS=1, SP=2, SPt=3), disease etiology (ordinal), and spinal level (binary) entered simultaneously. Proportional hazards assumptions were verified graphically using log-log plots. All analyses were performed in Python 3.10 (lifelines v0.27; scipy v1.11). Statistical significance was defined as p<0.05 (two-tailed).
Results
1. Patient demographics and baseline characteristics
Of 149 patients who underwent syringomyelia surgery during the study period, 42 met the inclusion criteria. The remaining 107 patients were excluded due to incomplete follow-up (n=82), adhesiolysis-only procedures (n=12), concurrent tumor resection without shunting (n=6), or combined shunting with adhesiolysis procedures (n=7). Baseline characteristics are summarized in Table 1. The cohort comprised 24 men (57.1%) and 18 women, with a mean age of 47.6±11.8 years (median, 51; range, 18 to 67 years). Disease involved the thoracic spine in 31 patients (73.8%) and the cervical spine in 11 (26.2%). The predominant etiology was post-traumatic (n=24, 57.1%), followed by post-infectious (n=10, 23.8%), idiopathic (n=6, 14.3%), and hemorrhage/tumor-related (n=2, 4.8%). Shunt type distribution was SP (n=16, 38.1%), SPt (n=14, 33.3%), and SS (n=12, 28.6%). Baseline demographics were comparable across shunt type groups (all p>0.05) (Table 1). Median follow-up was 15 months (mean, 36.7±42.3 months; range, 12 to 184 months). During follow-up, 16 patients (38.1%) underwent revision surgery for shunt failure (Table 1).
2. Overall shunt survival
The overall 12- and 24-month Kaplan-Meier shunt patency rates were 79.6% and 72.5%, respectively. The estimated median shunt survival for the entire cohort was 72 months.
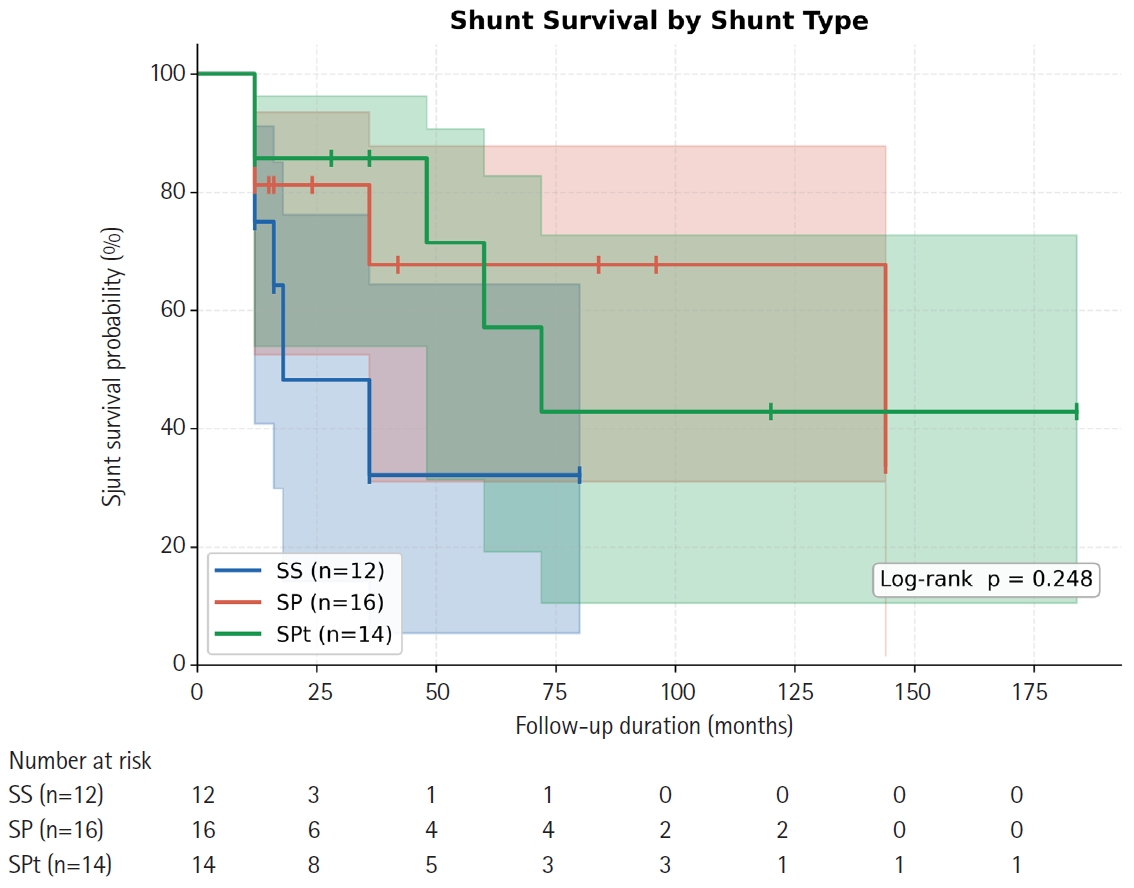
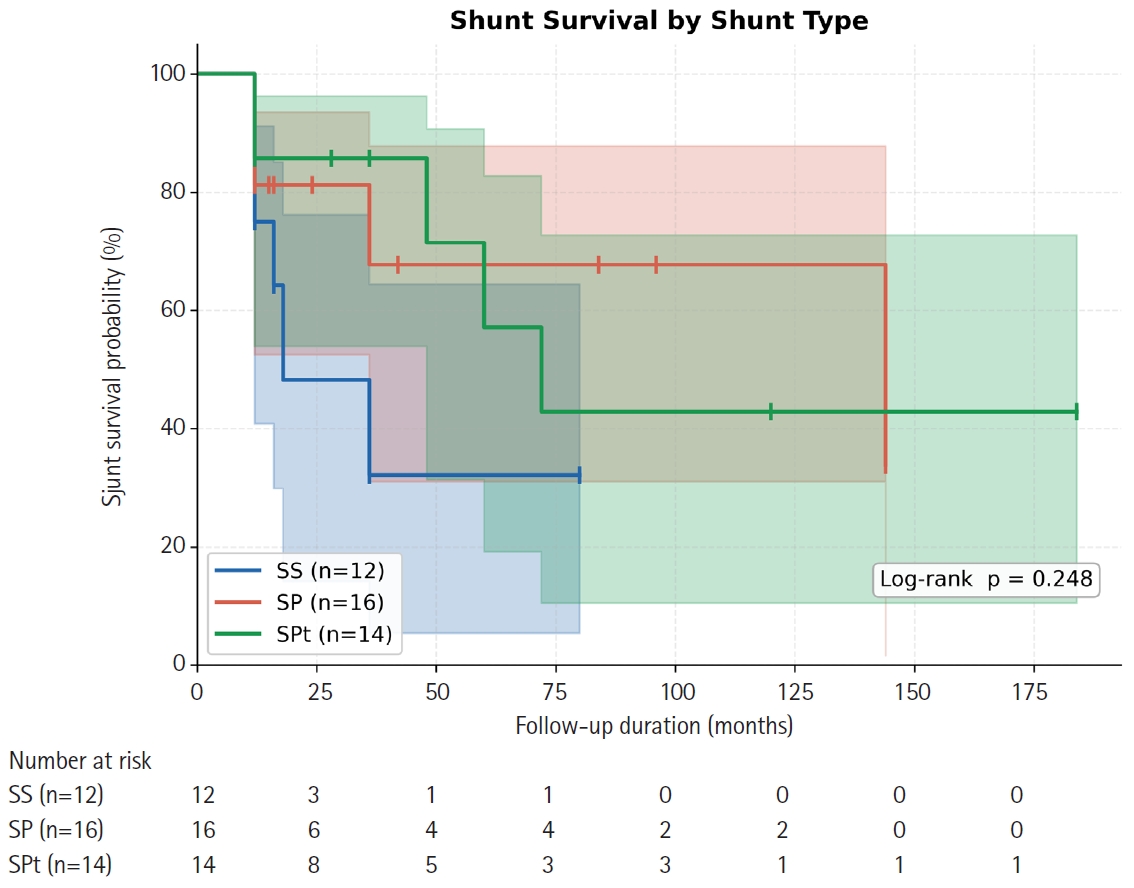
3. Shunt survival by shunt type
Kaplan-Meier survival estimates stratified by shunt type are presented in Table 2 and Fig. 1. The SS group demonstrated 12-month and 24-month patency rates of 75.0% and 48.2%, with a median shunt survival of only 18 months. The SP group achieved 12- and 24-month patency of 81.3% each, with an estimated median survival of 144 months. The SPt group showed 12- and 24-month patency rates of 85.7% each and a median shunt survival of 72 months. Although SS demonstrated a numerically inferior trajectory beyond 12 months, the overall difference across the three groups did not reach statistical significance (log-rank p=0.248) (Fig. 1). Pairwise comparisons also failed to achieve significance: SS vs. SP (p=0.179), SS vs. SPt (p=0.155), and SP vs. SPt (p=0.927) (Table 2, Fig. 1).
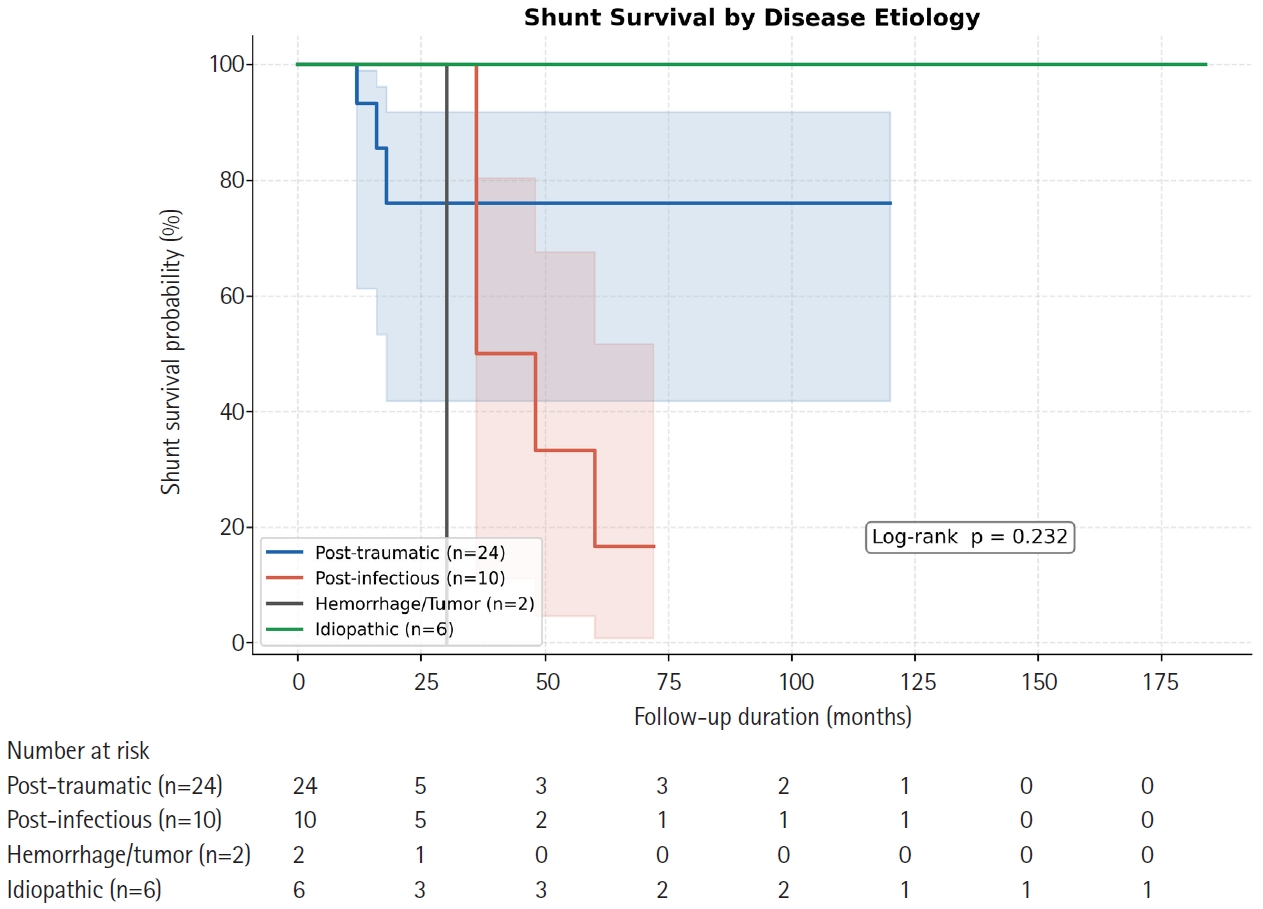
4. Shunt survival by disease etiology
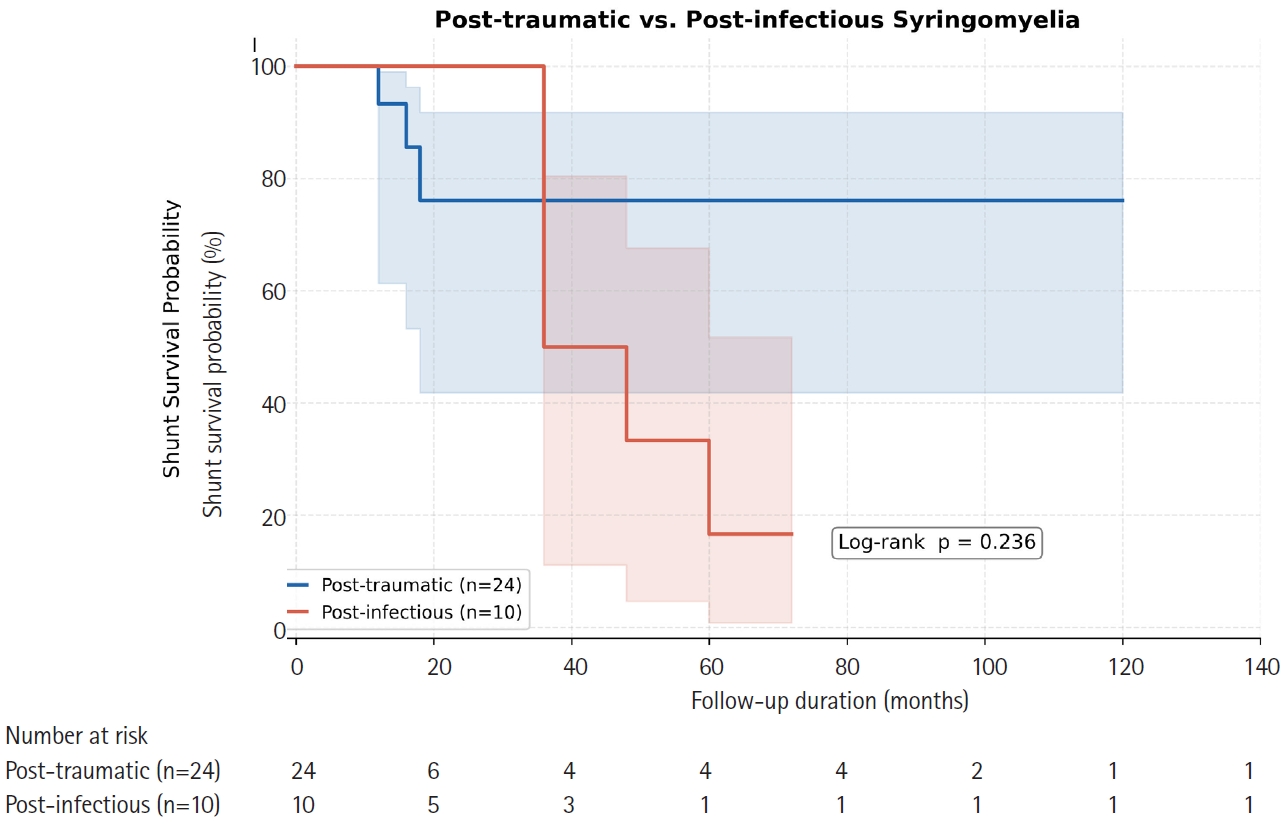
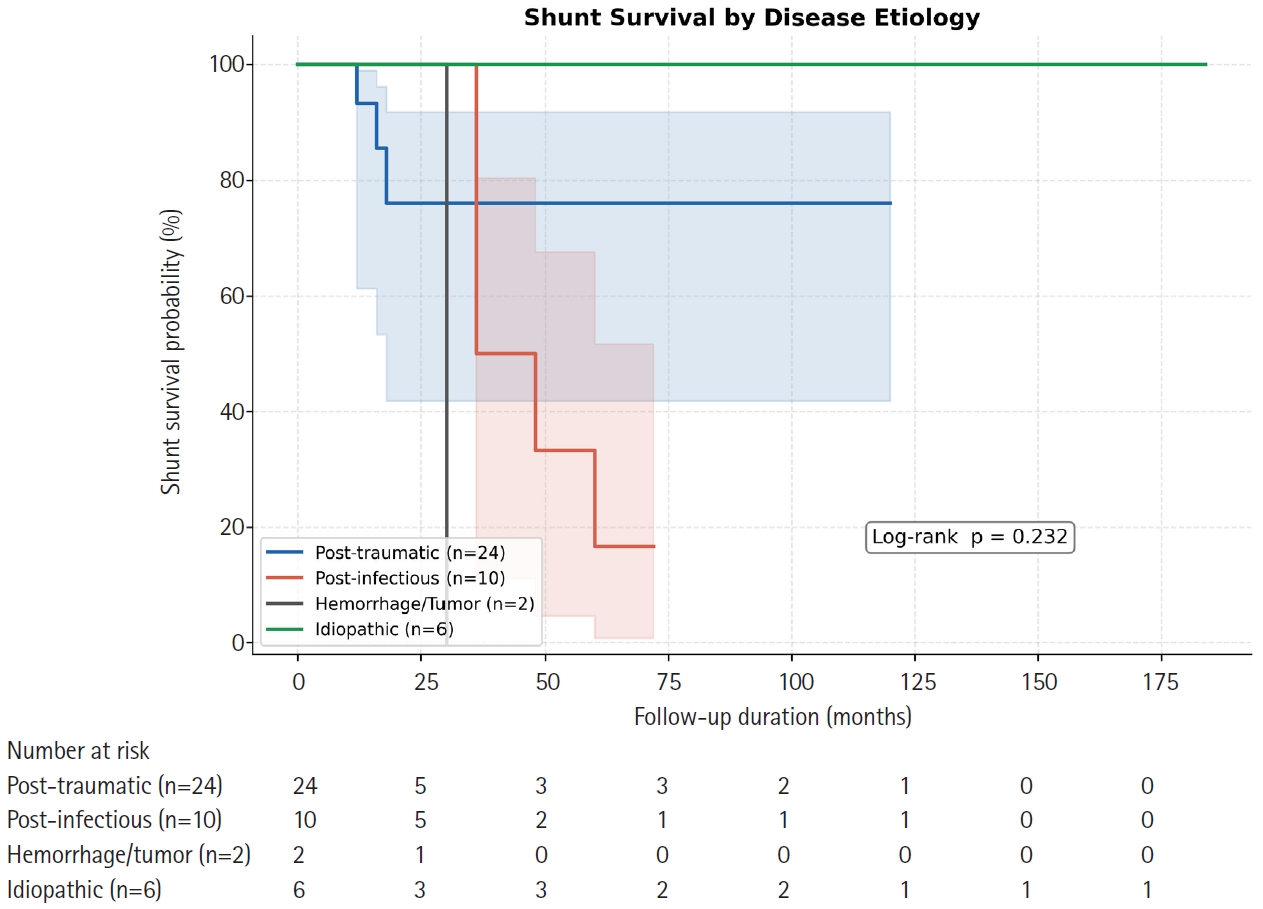
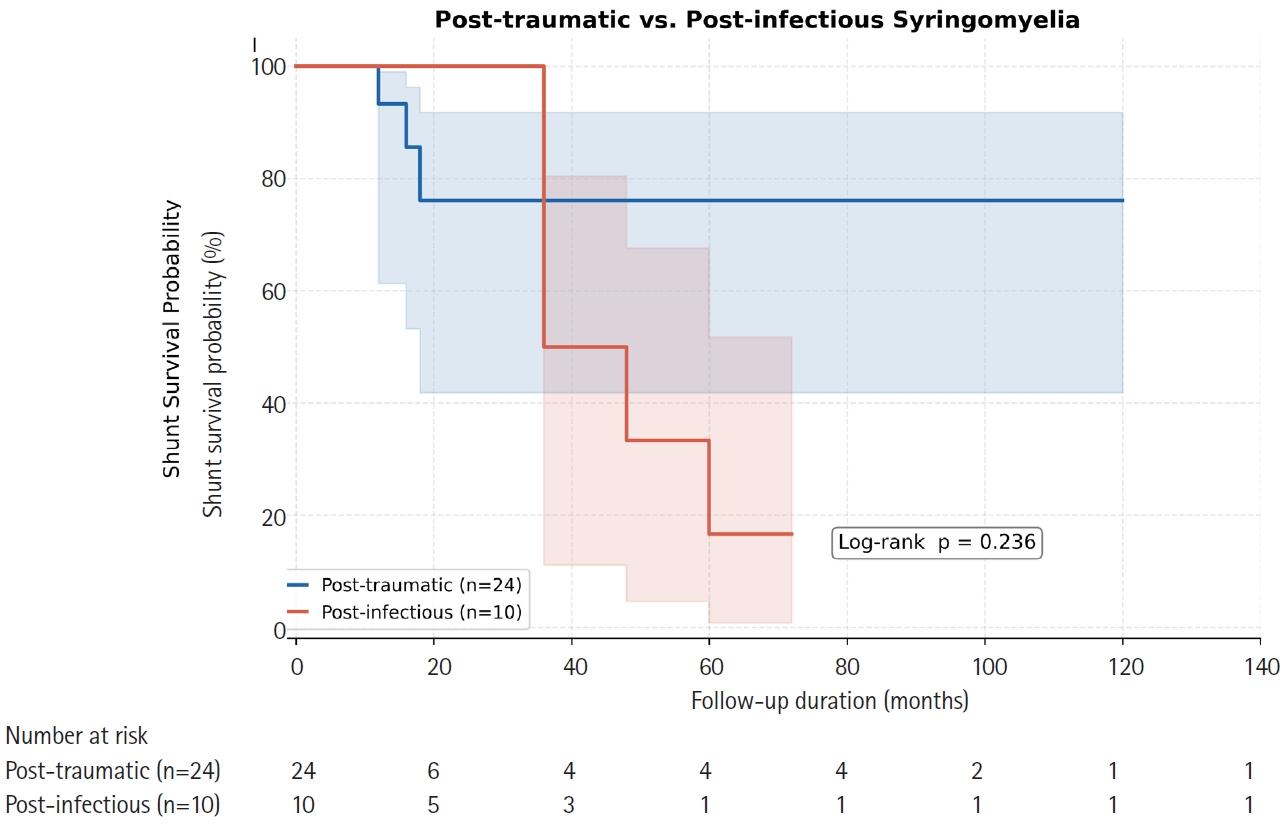
Kaplan-Meier survival curves stratified by etiology are shown in Fig. 2. Post-infectious syringomyelia demonstrated the shortest median shunt survival (36 months) and the highest revision burden (n=10; 12-month patency, 72.7%). Post-traumatic and idiopathic groups both had median survivals that were not reached within the observation period (12-month patency, 82.1% and 83.3%, respectively). The hemorrhage/tumor-related group (n=2) was too small for meaningful survival estimation. No statistically significant difference across etiologic groups was detected (log-rank p=0.232) (Fig. 2). Direct pairwise comparison of post-traumatic versus post-infectious cases showed a consistent trend favoring the post-traumatic group but did not achieve significance (log-rank p=0.236) (Fig. 3), likely reflecting inadequate statistical power (Figs. 2, 3).
Multivariable Cox regression results are presented in Table 3. None of the preoperative variables entered—age, shunt type, disease etiology, or spinal level—were independently associated with shunt failure at the p<0.05 threshold. The hazard ratio (HR) for shunt type was 0.714 (95% confidence interval [CI], 0.420 to 1.215; p=0.214), suggesting a trend toward lower failure risk with SP and SPt that did not reach significance. The HR for disease etiology was 0.863 (95% CI, 0.533 to 1.399; p=0.551). Age and spinal level were similarly non-significant (Table 3).
Discussion
This retrospective cohort study provides survival analysis data for syringomyelia shunting across three surgical modalities and four etiologic subgroups from a single tertiary East Asian neurosurgical center. The overall 12-month shunt patency of 79.6% and revision rate of 38.1% are consistent with the range of 60%–85% reported in historical series.9-11,13,14)
Our data suggest that SS may carry an inferior long-term patency profile. The 24-month patency of SS declined markedly to 48.2%, compared with 81.3% for SP and 85.7% for SPt, and the median shunt survival of SS (18 months) was substantially shorter. The physiological rationale for this observation relates to the pressure dynamics exploited by each technique. SS shunts rely on the pressure differential between the high-pressure syrinx and the adjacent subarachnoid space; in patients with ongoing arachnoid fibrosis or subarachnoid adhesions—conditions inherent to post-traumatic and post-infectious disease—this gradient may be insufficient or unstable.8,15,18,21) SP and SPt shunts, conversely, drain into large-capacity body cavities with consistently lower pressure (pleural cavity, −5 to 0 cmH2O; peritoneum, ≈0 cmH2O), providing theoretically more reliable sustained drainage.13,14,22) These findings align with the series by Tator et al.,12) who reported early occlusion as the primary limitation of the syringosubarachnoid technique, and with the comparative data of Batzdorf et al.10)
Nonetheless, the log-rank test did not detect a statistically significant difference across shunt types (p=0.248). This should not be interpreted as equivalence; the sample sizes in each arm (n=12–16) are substantially underpowered to detect the magnitude of difference observed between SS and SP at 24 months (48.2% vs. 81.3%). A sample of >80 patients per arm would be required for 80% power at α=0.05 under these effect assumptions, underscoring the need for multicenter collaboration.
The etiology-stratified analysis yielded a clinically meaningful finding: post-infectious syringomyelia was associated with the highest revision burden (n=10) and the shortest median shunt survival, markedly inferior to post-traumatic (not reached) and idiopathic (not reached) groups. Post-infectious cases in our cohort predominantly involved a history of tuberculous meningitis or bacterial meningitis resulting in spinal arachnoiditis. The dense fibroinflammatory adhesions in this setting impair CSF circulation bidirectionally: proximally, generating the pressure that drives syrinx formation, and distally, by progressively encasing and obstructing the shunt catheter following implantation.6,8,9,18) These findings are consistent with the series by Klekamp et al.,9) who similarly reported higher revision rates in arachnoiditis-related syringomyelia compared with other etiologies. Clinically, this mandates a lower threshold for MRI surveillance and symptom reassessment in post-infectious patients.
Post-traumatic syringomyelia demonstrated the most durable shunt longevity in our cohort, with a median survival not reached over a maximum follow-up of 184 months. The predominantly focal nature of the pathological process in post-traumatic syringomyelia—centered on the injury-level fibro-arachnoid scar rather than diffuse spinal arachnoiditis—likely explains the relatively favorable shunt durability observed.5-7,16,17) This is consistent with earlier series by Klekamp et al.,21) who noted better outcomes after shunting in post-traumatic compared with post-infectious arachnoiditis.
The absence of significant independent predictors on Cox regression is likely attributable to the small sample size rather than a genuine absence of effect. Unmeasured confounders—including intraoperative extent of arachnoid adhesions (graded by some authors as Klekamp grade I–IV),8) catheter type and gauge, CSF pressure measurement, and surgeon volume—may also have diluted true associations. The ordinal coding of shunt type and etiology additionally imposes linearity assumptions that may not reflect the underlying biology.
Several limitations of this study merit acknowledgment. First, the retrospective single-center design introduces selection and confounding biases, particularly because shunt type was non-randomly assigned. Second, data collection spanning two decades introduces temporal heterogeneity in surgical technique, catheter materials, and postoperative imaging protocols. Third, only 42 of 149 patients in the database met full inclusion criteria, reducing representativeness. Fourth, our primary endpoint of revision surgery may underestimate true shunt failure if subclinical dysfunction was not systematically investigated by surveillance imaging. Fifth, the hemorrhage/tumor-related subgroup (n=2) was too small for meaningful subgroup analysis. Future prospective multicenter registries with standardized outcome definitions, mandatory surveillance MRI protocols, and intraoperative arachnoid adhesion grading are needed to overcome these limitations.
Syringomyelia shunting with SS, SP, or SPt achieves approximately 80% 1-year shunt patency. Syringo-subarachnoid shunts appear to carry a higher long-term occlusion risk, with a 24-month patency of only 48.2% compared with 81%–86% for SP and SPt, though this finding requires confirmation in larger series. Post-infectious syringomyelia is associated with the highest revision burden and shortest median shunt survival, warranting heightened postoperative surveillance. Multicenter prospective studies with standardized protocols are required to definitively guide shunt type selection and postoperative management in syringomyelia.
Bong Ju Moon, a contributing editor of the Journal of Advanced Spine Surgery, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Funding
None.
Acknowledgments
None.
Fig. 1.
Kaplan-Meier shunt survival curves stratified by shunt type. Tick marks indicate censored observations. Numbers at risk at each time point are shown below the x-axis. SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
Fig. 2.
Kaplan-Meier shunt survival curves by disease etiology. Tick marks on the curves indicate censored observations. Numbers at risk at each time point are shown below the x-axis.
Fig. 3.
Head-to-head Kaplan-Meier comparison: post-traumatic vs. post-infectious syringomyelia (log-rank p=0.236). Tick marks on the curves indicate censored observations. Numbers at risk at each time point are shown below the x-axis.
Table 1.
Baseline characteristics by shunt type
Variable
Total (n=42)
SS (n=12)
SP (n=16)
SPt (n=14)
p-value
Age (years)
47.6±11.8
46.3±14.2
48.9±11.1
47.1±10.8
0.838
Male sex
24 (57.1)
7 (58.3)
9 (56.3)
8 (57.1)
>0.99
Thoracic level
31 (73.8)
8 (66.7)
12 (75.0)
11 (78.6)
0.824
Etiology
Post-traumatic
24 (57.1)
6 (50.0)
10 (62.5)
8 (57.1)
0.976
Post-infectious
10 (23.8)
4 (33.3)
3 (18.8)
3 (21.4)
-
Hemorrhage/tumor-related
2 (4.8)
0 (0)
1 (6.3)
1 (7.1)
-
Idiopathic
6 (14.3)
2 (16.7)
2 (12.5)
2 (14.3)
-
Shunt revision
16 (38.1)
6 (50.0)
5 (31.3)
5 (35.7)
0.667
Follow-up (months)
15 (12–184)
16 (12–80)
16 (12–144)
32 (12–184)
0.180
Values are presented as mean±standard deviation, number (%), or median (range). p-values by one-way ANOVA (continuous) or Fisher exact test (categorical). SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
Table 2.
Kaplan-Meier shunt survival estimates by shunt type
Outcome
SS (n=12)
SP (n=16)
SPt (n=14)
p-value (log-rank)
Shunt revisions, n (%)
6 (50.0)
5 (31.3)
5 (35.7)
0.471
12-Month patency (%)
75
81.3
85.7
0.248
24-Month patency (%)
48.2
81.3
85.7
Shunt survival (months), median
18
144
72
Follow-up (months), median (range)
16 (12–80)
16 (12–144)
32 (12–184)
Patency rates are Kaplan-Meier estimates. Overall p-value by three-group log-rank test. SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
Table 3.
Multivariable Cox proportional hazards analysis for shunt failure
Variable
Hazard ratio
95% Confidence interval
p-value
Age (per year increase)
1.035
0.988–1.084
0.146
Shunt type (SS→SP→SPt)
0.714
0.420–1.215
0.214
Disease etiology
0.863
0.533–1.399
0.551
Spinal level (thoracic vs. cervical)
0.955
0.327–2.786
0.933
Hazard ratio <1 indicates lower hazard of revision (longer patency) for higher-coded category. SS=1, SP=2, SPt=3 for shunt type coding. SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
References
1. Milhorat TH. Classification of syringomyelia. Neurosurg Focus 2000;8:E1.
14. Padovani R, Cavallo M, Gaist G. Surgical treatment of syringomyelia: favorable results with syringosubarachnoid shunting. Surg Neurol 1989;32:173-80.
17. Carroll AM, Brackenridge P. Post-traumatic syringomyelia: a review of the cases presenting in a regional spinal injuries unit in the north east of England over a 5-year period. Spine (Phila Pa 1976) 2005;30:1206-10.
18. Davidoff CL, Liu S, Wong JH, Koustais S, Rogers JM, Stoodley MA. Treatment of syringomyelia in patients with arachnoiditis at the craniocervical junction. World Neurosurg 2017;107:565-73.
21. Klekamp J, Batzdorf U, Samii M, Bothe HW. Treatment of syringomyelia associated with arachnoid scarring caused by arachnoiditis or trauma. J Neurosurg 1997;86:233-40.
22. Isik N, Elmaci I, Isik N, et al. Long-term results and complications of the syringopleural shunting for treatment of syringomyelia: a clinical study. Br J Neurosurg 2013;27:91-9.
Survival Analysis of Syringopleural, Syringoperitoneal, and Syringosubarachnoid Shunts for Syringomyelia: A Single-Center Retrospective Cohort Study
Fig. 1. Kaplan-Meier shunt survival curves stratified by shunt type. Tick marks indicate censored observations. Numbers at risk at each time point are shown below the x-axis. SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
Fig. 2. Kaplan-Meier shunt survival curves by disease etiology. Tick marks on the curves indicate censored observations. Numbers at risk at each time point are shown below the x-axis.
Fig. 3. Head-to-head Kaplan-Meier comparison: post-traumatic vs. post-infectious syringomyelia (log-rank p=0.236). Tick marks on the curves indicate censored observations. Numbers at risk at each time point are shown below the x-axis.
Fig. 1.
Fig. 2.
Fig. 3.
Survival Analysis of Syringopleural, Syringoperitoneal, and Syringosubarachnoid Shunts for Syringomyelia: A Single-Center Retrospective Cohort Study
Variable
Total (n=42)
SS (n=12)
SP (n=16)
SPt (n=14)
p-value
Age (years)
47.6±11.8
46.3±14.2
48.9±11.1
47.1±10.8
0.838
Male sex
24 (57.1)
7 (58.3)
9 (56.3)
8 (57.1)
>0.99
Thoracic level
31 (73.8)
8 (66.7)
12 (75.0)
11 (78.6)
0.824
Etiology
Post-traumatic
24 (57.1)
6 (50.0)
10 (62.5)
8 (57.1)
0.976
Post-infectious
10 (23.8)
4 (33.3)
3 (18.8)
3 (21.4)
-
Hemorrhage/tumor-related
2 (4.8)
0 (0)
1 (6.3)
1 (7.1)
-
Idiopathic
6 (14.3)
2 (16.7)
2 (12.5)
2 (14.3)
-
Shunt revision
16 (38.1)
6 (50.0)
5 (31.3)
5 (35.7)
0.667
Follow-up (months)
15 (12–184)
16 (12–80)
16 (12–144)
32 (12–184)
0.180
Outcome
SS (n=12)
SP (n=16)
SPt (n=14)
p-value (log-rank)
Shunt revisions, n (%)
6 (50.0)
5 (31.3)
5 (35.7)
0.471
12-Month patency (%)
75
81.3
85.7
0.248
24-Month patency (%)
48.2
81.3
85.7
Shunt survival (months), median
18
144
72
Follow-up (months), median (range)
16 (12–80)
16 (12–144)
32 (12–184)
Variable
Hazard ratio
95% Confidence interval
p-value
Age (per year increase)
1.035
0.988–1.084
0.146
Shunt type (SS→SP→SPt)
0.714
0.420–1.215
0.214
Disease etiology
0.863
0.533–1.399
0.551
Spinal level (thoracic vs. cervical)
0.955
0.327–2.786
0.933
Table 1. Baseline characteristics by shunt type
Values are presented as mean±standard deviation, number (%), or median (range). p-values by one-way ANOVA (continuous) or Fisher exact test (categorical). SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
Table 2. Kaplan-Meier shunt survival estimates by shunt type
Patency rates are Kaplan-Meier estimates. Overall p-value by three-group log-rank test. SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.
Table 3. Multivariable Cox proportional hazards analysis for shunt failure
Hazard ratio <1 indicates lower hazard of revision (longer patency) for higher-coded category. SS=1, SP=2, SPt=3 for shunt type coding. SS: syringo-subarachnoid shunt, SP: syringo-pleural shunt, SPt: syringo-peritoneal shunt.

 , Dongkyu Kim, M.D., Ph.D.
, Dongkyu Kim, M.D., Ph.D.