Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
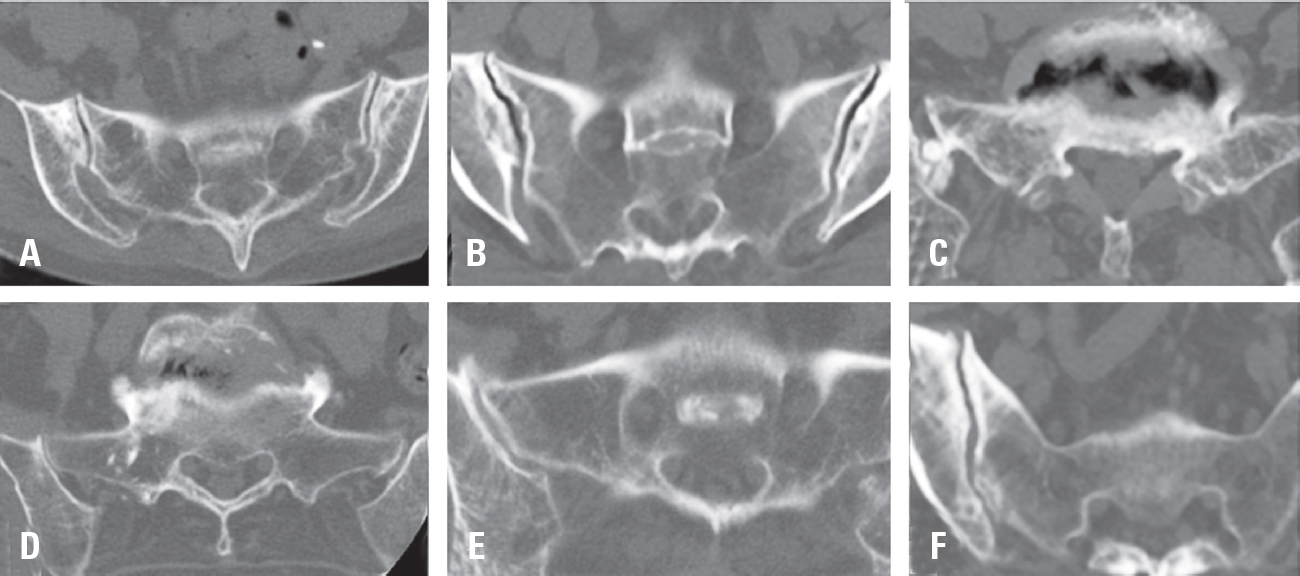
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
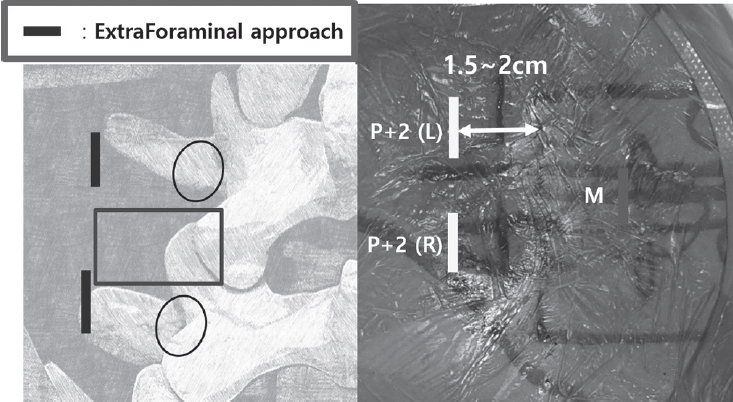
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
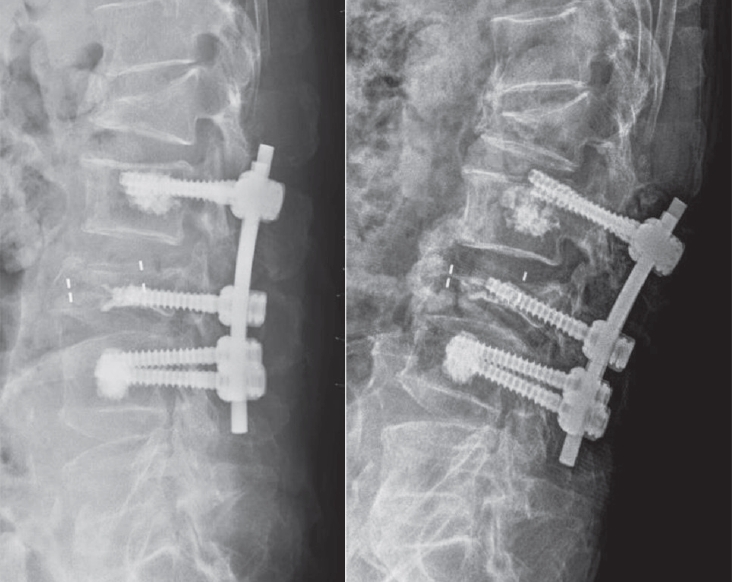
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
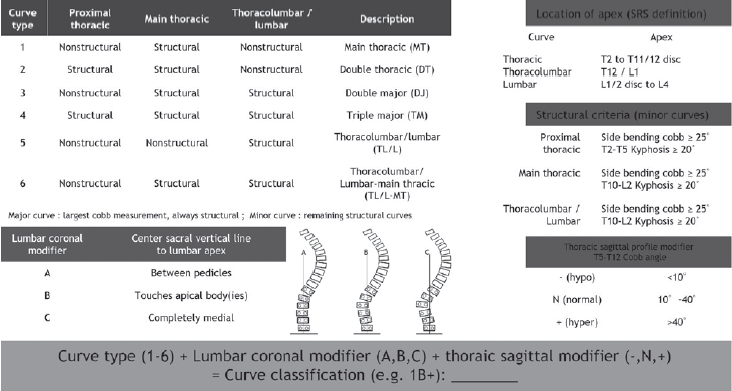
Adolescent idiopathic scoliosis refers to spinal deformity that develops from just before the onset of puberty until the completion of skeletal growth, and the primary goal of treatment is to achieve a well-balanced spine. In the late 1990s, advances in the anatomical understanding of the spine and the development of fixation instruments made posterior pedicle screw insertion feasible, thereby enabling the transmission of powerful corrective forces for deformity correction. Over the subsequent decades, accumulated clinical experience and outcomes have provided a deeper understanding of scoliotic curves and led to the establishment of effective principles for determining the extent of spinal fusion. However, these treatment principles are based on the unique biomechanics and procedural characteristics of scoliosis correction surgery, which can make them difficult to understand without sufficient explanation. In this review, we aim to describe these established treatment principles and surgical processes in detail using schematic illustrations and images. Although these principles will continue to undergo new challenges and validation over time, they will remain a meaningful reference point for those exploring alternative strategies.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
Advanced imaging technologies have revolutionized the diagnosis and management of spinal pathologies by providing superior precision and efficiency. Modalities such as PET-CT, SPECT, diffusion tensor imaging (DTI), and magnetic resonance spectroscopy (MRS) offer unique insights into the metabolic, structural, and functional aspects of spinal diseases, enabling better differentiation of lesions, improved surgical planning, and early detection of pathological changes. Furthermore, the integration of artificial intelligence (AI) has enhanced imaging workflows by enabling automated analysis, prediction of clinical outcomes, and segmentation of spinal structures. Despite these advancements, challenges such as technical limitations, high costs, and ethical concerns, including issues of data privacy and AI-generated inaccuracies, hinder widespread adoption. This review explores the clinical applications, limitations, and future directions of these emerging technologies, highlighting the need for multidisciplinary collaboration and large-scale research to standardize protocols and optimize patient outcomes. The seamless integration of advanced imaging and AI represents a transformative potential for improving diagnostic accuracy and treatment efficacy in spinal care.
Background The Selective thoracic fusion (STF) may be associated with risk of postoperative coronal decompensation, lumbar decompensation and adding-on phenomenon, which can lead to persistence of the lumbar curve and consequently to deviation of the trunk. Therefore, the STF is the most debatable issue as the optimal surgical correction in adolescent idiopathic scoliosis with Lenke 1C curves.
Methods A total of 30 patients with adolescent idiopathic scoliosis with Lenke 1C curves who underwent STF between 1996 and 2017 were included. Minimum follow-up duration was five years. We analyzed the incidence of coronal decompensation, lumbar decompensation, distal adding-on phenomenon and trunk shift in these patients for radiographic adverse event. Clinical outcome was assessed by using the Scoliosis Research Society (SRS)-22r scores.
Results The mean age at the time of surgery was 13.8±2.9 years. The mean follow-up duration was 80.4±12.3 months.
The Cobb’s angle for main thoracic curve improved by 59.6% (p<0.001), and also The Cobb’s angle for thoracolumbar/ lumbar curve improved by 40.5% comparing preoperative and postoperative values (p<0.001). There was significant improvement in the Cobb’s angle for main thoracic and Thoracolumbar/lumbar curve comparing preoperative and last follow-up values (p<0.001). At last follow-up, the coronal balance was 10.3 ± 9.1 that significant improved from the immediate postoperative value (p=0.033). The incidence of coronal decompensation, lumbar decompensation, adding-on and trunk shift in our cohort was 16.7%, 10.0%, 13.3% and 10.0% respectively. The average SRS score at last follow-up in patients with radiographic adverse events was 4.3±0.5. That of patients without adverse events was 4.4±0.6. All domains between patients with and without adverse events had no statistical significance difference.
Conclusions Selective thoracic fusion in Lenke 1C curves have acceptable risk of coronal decompensation, lumbar decompensation, distal adding-on, trunk shift. However, no revision surgery was required in these patients after long term follow-up. Therefore, STF in Lenke 1C curves seems to be enough.
Background Minimally invasive transpsoas or antepsoas lateral lumbar interbody fusion (MI-LLIF) has been reported as an effective surgical option for various lumbar diseases. Many researchers reported high fusion rate and clinical excellence of LLIF with the use of bone morphogenic protein (BMP). However, there have been paucity of studies regarding LLIF without the use of BMP. Therefore, this study aimed to analyze radiologic and clinical results of patients who underwent minimally invasive lateral lumbar interbody fusion without the use of BMP. Furthermore, a further analysis was conducted regarding the frequency of cage subsidence and its impact on the radiologic and clinical outcome.
Materials and Methods Fifty patients and 109 levels treated by MI-LLIF with postoperative follow-up of at least 2 years were included. Radiologic evaluation included intervertebral disc height, segmental lordosis, lumbar lordosis, fusion rate, cage subsidence grade, and the bone mineral density. Radiologic fusion was determined by modified Bridwell’s grade, and cage subsidence by Marchi’s grade. Clinical outcome was evaluated by VAS of low back pain (LBP) and leg pain, and ODI score. The above clinical and radiologic variables were analyzed statistically for comparison of cage subsidence and nonsubsidence groups.
Results There were 20 male and 30 female patients with the average age of 69 years. Average follow-up period was 29.6 months(24-42 months). Graft material used for PEEK cage was autogenous bone only in 9 levels, autogenous bone and DBM in 19 levels, and DBM only in 81 levels. Twelve patients received surgery on 1 level, 20 patients on 2 levels, 17 patients on 3 levels, and 1 patient on 4 levels, respectively. Operated levels were L1-2 in 7 cases, L2-3 in 27, L3-4 in 41, and L4-5 in 34, respectively. Mean low back pain (LBP) VAS decreased from preoperative 5.5 to 2.2 at the final follow-up, leg pain from 6.1 to 1.7, and ODI score from 25.6 to 13.7, with statistical significance (p<0.001). Mean disc height increased from preoperative 5.9 mm to postoperative 11.5 mm, and subsequently decreased to 9.6mm at the final follow-up. Average lumbar lordosis increased from preoperative 18.6 degrees to postoperative 37.0 degrees, and 35.9 degree at final follow-up. Radiologic union rate was 90.8%. Cage subsidence was observed in 6 levels (5.5%) on immediate postoperative radiographs; and in 20 levels (18.3%) at final follow-up. Comparison between cage subsidence and non-subsidence groups revealed no significant difference in age and BMD. Immediate postoperative segmental lordosis was considered as a risk factor of cage subsidence (p=0.005, odds ratio 0.813, CI 0.703~0.940). Furthermore, the preoperative and the final follow-up measurement of disc height, VAS score of LBP and leg pain, and ODI score were not different between the two groups. However, pseudoarthrosis rate was higher in subsidence group.
Conclusions Minimally invasive LLIF was an effective surgical option with high fusion rate even without the use of BMP.
Although cage subsidence also increases the frequency of pseudarthrosis, it does not significantly deteriorate the lumbar lordosis correction and clinical outcome.
Purpose Minimally invasive technique in spinal surgery have evolved including cortical bone trajectory (CBT) screw technique which is s new lumbar pedicle screw path, as an alternative fixation technique for lumbar spine.
Theoretical advantage is that it provides enhanced screw torque and has biomechanical characteristics, also it minimizes approach-related damages. Midline lumbar fusion (MIDLF) has appeared with CBT screw technique.
Many studies of CBT screw reported the effectiveness of MIDLF. We adopted this technique for lumbar degenerative spondylolisthesis and evaluated early radiological outcomes.
Materials and Methods From May 2014 to March 2015, 17 patients (mean age 65.6±7.5 years; 4 males, 13 females) underwent MIDLF procedures for the treatment of single level lumbar spondylolisthesis. Average follow-up period was 8.8±2.7 months. Initial and last follow-up X-ray and computed tomography (CT) were evaluated for screw malposition, detection of peri-screw halo, loosening of the construct, or signs of spinal instability.
Results The average bone mineral density (BMD) was -1.9±0.8. Eleven patients were fused at L4-5, 5 were at L3-4, and 1 was at L2-3. Five CBT screws were converted into pedicle screws due to intraoperative misposition of screws, so total 63 CBT screws were evaluated for peri-screw halo and malposition. There were no findings of screw pull-out or breakage in all screws. Four out of 63 (6.3%) screws were judged as peri-screw halo, and 20 (41.2%) screws were judged as malposition (1 medial; 2 superior; 17 lateral pedicle violation). But, there were no screw related nerve root injury. In all cases, interbody bony mass were identified. Four out of 17 (23.6%) patients were detected more than 2 degrees motions on flexion-extension lateral X-rays at final follow-up, and 1 out of these 4 patients was identified loss of reduction. There was no operation related complication.
Conclusion There is no doubt that MIDLF with CBT screw is the minimally invasive method. Many numbers of screw malposition identified in our series were thought to be due to our earlier experience of trying free hands technique.
We recommend the use of intraoperative fluoroscopy, which achieve accuracy. Although MIDLF with CBT has theoretical strengths, we must evaluate further long-term clinical follow-up and measure outcome.
Objective To evaluate the efficacy and safety of anorganic bone matrix (ABM)/P-15 compared with local autograft bone in posterior lumbar interbody fusion (PLIF) with pedicle screws for degenerative lumbar diseases.
Methods This is a retrospective analysis of consecutive series of 138 patients undergoing 1 or 2 levels PLIF from 2015 to 2020 in our single institute. Local autograft bone or ABM/P-15 (i-factor, Cerapedics Inc., Westminster, Colorado USA) were used for interbody fusion. The successful fusion was defined as the segmental cobb angle of less than 5 degrees of in flexion/extension X-rays and continuity of the trabecular bony bridging in computed tomography (CT) images.
Results Among a total of 138 patients, total levels of fusion were 202, of which 74 were in 1 level fusion and 128 were in 2 level fusion. And 93 used ABM/P-15 and 109 used local autograft bone. The evaluation time of fusion status was 1 year after surgery. Successful fusion based on X-ray images was achieved 84.1% (90/107) for local autograft bone and 91.3% (84/92) for ABM/P-15 (p=0.127). Based on CT images, 86.9% (93/107) of autograft group and 95.6%(87/91) of AMP/P-15 group showed successful fusion respectively (p=0.034). Occurrence rate of autolysis was 14% (15/107) for local autograft bone and 17.6% (16/91) for ABM/P-15. Subsidence rates were 11.2% (12/107) for local autograft bone and 9.99% (9/91) for ABM/P-15. Hollow formation around pedicle screw was noted in 9.3% (10/107) for local autograft bone and 2.2% (2/91) for ABM/P-15.
Conclusions The use of AMP/P-15 for lumbar interbody fusion surgery can be a good substitute for local autograft bone in terms of better fusion rate and similar complication rate on radiologically.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Purpose To evaluate whether the contralateral radiating pain improved after unilateral decompression and minimally invasive transforaminal lumbar interbody fusion (TLIF) in the patients with bilateral radiating pain due to degenerative lumbar disease.
Materials and Methods Patients with the degenerative lumbar disease who underwent unilateral minimally invasive TLIF and were followed for more than 1 year were included. Clinically, low back pain and radiating pain on the dominant symptom side and the contralateral side were evaluated by the visual analogue score (VAS), and the Oswestry disability index (ODI) score was also evaluated.
Results ODI and VAS of low back pain and radiating pain were effectively reduced in a total of 57 cases. Thirty cases having bilateral radiating pain, among these patients, unilateral decompression was performed in 15 cases and bilateral decompression thru unilateral approach in 15 patients. In unilateral decompression group, radiating pain on the dominant symptom side, and radiating pain on the contralateral side were also improved at the final followup. In 15 cases who underwent bilateral decompression, radiating pain on the dominant symptom side and the contralateral side were improved at the final follow-up. There was no significant difference between the two groups in terms of preoperative ODI, VAS of low back and radiating pain.
Conclusions Minimally invasive TLIF via unilateral approach with or without contralateral decompression showed good clinical results in patients having unilateral or bilateral radiating pain. Minimally invasive TLIF could be an useful option even if there is bilateral radiating pain in degenerative lumbar disease.
Background Oblique and anterior lumbar interbody fusion have been widely performed in the lumbar spinal disease but we cannot get a direct decompression effect with these procedure.
Objective: The purpose of this study is to report clinical and imaging outcomes of microscope assisted direct decompression combined with oblique lumbar interbody fusion (OLIF) or anterior lumbar interbody fusion (ALIF).
Methods Twelve patients who received microscope assisted direct decompression during OLIF or ALIF for lumbar spinal stenosis were enrolled. The OLIF was performed for the lesion upper than the L4-5 or in the case of multisegmental disease. The ALIF was performed for the lesion at the L5-S1. After anterior-approaching surgery, percutaneous fixation of pedicle screw was performed and we did not perform an additional decompression posteriorly in all cases. For the clinical outcomes, we evaluated short form 36 (SF-36), Oswestry disability index (ODI) score and visual analog scale (VAS) pain score. For the imaging outcomes, we obtained postoperative lumbar magnetic resonance imaging (MRI).
Results The OLIF was performed for 9 patients and the ALIF was performed for 3 patients. In the clinical outcomes, SF-36 was improved from 25.40 to 69.83 and ODI score was also improved from 69.83 to 16.50. VAS pain score of back was improved from 4.3 to 1.6 and VAS pain score of leg was improved from 7.5 to 2.2. In the imaging outcomes, all patients had severe stenosis before surgery. After surgery the severity of the stenosis was reduced to mild state in 9 cases and moderate state in 3 cases postoperatively.
Conclusions We could obtain the good clinical outcomes and effective decompression through microscope assisted direct decompression during OLIF or ALIF.
Purpose Spinal fusion is useful method of treatment of degenerative lumbar diseases, and is divided into anterior and posterior surgery. Each approach has advangages and disadvantages. Recently, minimally invasive lateral lumbar interbody fusion (LLIF) supplemented disadvantages of anterior and posterior surgery is interested. We introduce LLIF and present about application and indication of LLIF.
Materials and Methods A 76-year-old female was diagnosed by degenerative disc disease on L2-3. A 66-year-old male was diagnosed by central spinal stenosis on L2-3-4-5. A 86-year-old female was diagnosed by foraminal stenosis on L3-4-5 and degenerative scoliosis. A 73-year-old male was diagnosed by spinal stenosis on L3-4-5 and spondylolisthesis. A 70-year-old male was diagnosed nonunion on L4-5. On past history, the patient was operated by fusion because of L2 burst fracture. A 75-year-old female was diagnosed by infective spondylodiscitis on L3-4.
Results Degenerative disc disease, severe central and foraminal spinal stenosis, degenerative scoliosis, spondylolisthesis and infective spondylodiscitis were application and indication of LLIF.
Conclusions LLIF merges the advantages and covers the disadvantages of anterior and posterior surgery. However, approach-related lumbar plexus injury and L5-S1 approach were remained obstacles.
Introduction A spondylitis developed after a surgery has been usually treated with drainage and curettage through anterior approach and autoiliac strut bone graft. However, anterior support with titanium cage combined with posterior pedicle screw fixation has been attempted. Implanting a foreign material is usually prohibited at an active pyogenic infection site. We tried to prove the usefulness of chip bone graft with metal cages in surgical treatment of spondylitis developed in posterior lumbar intebody fusion cases.
Materials and Methods This is a retrospective study. The patients who received posterior lumbar interbody fusion (PLIF) between Jan. 2007 and Dec 2017 and had a spondylitis around the cage were reviewed. There were 1,831 PLIFs during the study period. There were 32 cases of surgical site infection and 20 of them were spondylitis around the cage. Ten out of the 20 cases had a revision surgery. All implants removal, drainage and curettage were done and interbody bone graft and pedicle screw re-fixation was done simultaneously. Five cases used autoiliac strut bone (Group I) and the other 5 cases used titanium cage and autoiliac chip bone (Group II) as interbody graft materials.
The demographic, diagnostic and microbiological characteristics were investigated and the results of treatment were compared between the two groups.
Results The diagnosis of infection was made at 282.0±106.1 (180~410) days in group I and 209±118.4 (75~335) days in group II after the PLIF. All cases had neither general fever nor local manifestations like heating and redness etc.
All patients had back pain, however, only 2 cases of group II had neurological symptoms. C-reactive protein (CRP) level was elevated at 2 weeks from the PLIF in all cases (p<0.001). All cases had implant loosening at the time of their diagnosis. There was no failure of infection control. All cases showed normalization of CRP and radiological interbody fusion. The final Oswestry disability index (ODI) showed no difference between the two groups. ODI improved from 54.6±11.5 to 42.2±6.8 in group I (p=0.095) and from 63.6±6.9 to 44.8±11.7 in group II (p=0.025).
Conclusion For the surgical treatment of spondylitis that were developed in PLIF, a comprehensive one stage operation that comprised all implants removal, drainage and curettage followed by simultaneous intebody bone graft with metal cages and pedicle screw re-fixation was useful to control the infection.
Background Proximal junctional kyphosis (PJK) following long instrumented fusion is a well-recognized complication that does not negatively affect the clinical outcomes. However, there were few studies with regard to the long-term consequences of PJK.
Objective: To investigate the long-term clinical and radiographic consequences of proximal junctional kyphosis (PJK) following the long instrumented fusion for elderly patients with sagittal imbalance.
Methods Patients older than 60 years who underwent ≥4 fusion including the sacrum for sagittal imbalance were followed up longer than five years. PJK was defined as proximal junctional angle (PJA) >10° without any bony compromise or myelopathy. The radiographic and clinical outcomes were compared between PJK and non-PJK groups. Clinical outcome measures included visual analog scale (VAS) for back and leg, Oswestry disability index (ODI), and Scoliosis Research Society (SRS)-22 scores.
Results A mean age was 69.2 years. An average follow-up duration was 92.4 months. There were 30 patients in PJK group and 43 in non-PJK group. At the final follow-up, pelvic incidence-lumbar lordosis mismatch, pelvic tilt, and sacral vertical axis were not different between the two groups. In PJK group, PJA significantly increased from 6.5° postoperatively to 21.2° at the final follow-up. At the final follow-up, clinical outcomes were worse in PJK group than in non-PJK group with regard to VAS for back, ODI, and SRS-22 scores except satisfaction domain. Three (10%) of 30 patients underwent a revision surgery for PJK progression.
Conclusions PJK progressed with time and negatively affect the clinical outcomes in a long-term follow-up after ASD surgery.
Lumbar fusion surgery for lumbar degenerative diseases has increased in the past several decades and many techniques for fusion surgery have been introduced. Recently lateral lumbar interbody fusion with minimally invasive technique was introduced and accepted as a useful method for various lumbar degenerative disease. It can produce good correction for sagittal and coronal imbalance with relatively decreased morbidity. The advantage of lateral lumbar interbody fusion is that it can avoid injury to the abdominal large vessels and neural structures which is more common during posterior approaches. However various complications had been reported. Complications related with lateral lumbar interbody fusion include neurologic complications including thigh pain and numbness, vascular complications including arterial injury, cage related complication such as cage subsidence and vertebral body fractures. Therefore special care should be taken to avoid possible complications in lateral lumbar interbody fusion surgery.
Purpose of Study: Purpose of this study is to summarize the technique of UBE surgery in lumbar interbody fusion and review the clinical outcomes and complications of UBE surgery in lumbar interbody fusion.
Materials and Methods Medical databases were searched for the key words of unilateral biportal endoscopic surgery and lumbar spinal stenosis using PubMed from 2005 to the present.
Conclusion UBE spinal surgery is a new technique that can be a feasible alternative and an effective treatment modality for spinal degenerative diseases and can achieve the necessary surgical skills for experienced microscopic surgeons, which is still expanding the indications for lumbar spinal surgery.
Objectives We report the new minimally invasive technique and its clinical results of oblique lumbar interbody fusion (OLIF) combined with central decompression using biportal endoscopic spinal surgery (BESS).
Summary of Literature Review: The OLIF procedure is one of the minimally invasive spine surgeries and is being frequently attempted recently to treat lumbar degenerative disease. It has been reported that it effectively decompresses foraminal stenotic lesions indirectly by inserting a large cage anteriorly, which reduces spondylolisthesis and widens the disc space. However, OLIF has limited effect for severe central canal stenosis, since it cannot achieve direct decompression. Therefore, authors report a new minimally invasive technique of OLIF combined with direct central decompression using BESS for severe central stenosis along with its clinical results as a pilot study.
Materials and Methods For patients who were candidate for fusion surgery due to spondylolisthesis (more than one segment) or foraminal stenosis, authors performed OLIF and central decompression using BESS simultaneously, when the patients had concomitant severe central canal stenosis. From June to December, 2017, 8 patients (16 levels) were enrolled, the operative time, blood loss, complications and clinical results have been evaluated. The clinical results were analyzed by Visual analog scale (VAS) scores, Oswestry disability index (ODI) and Roland Morris Disability Questionnaire (RMDQ) of preoperative, 1month, 3month postoperative and final follow-up.
Results Mean operative time and blood loss were 238.4 minutes and 173.3ml, respectively. In all cases, there were no operative complications, and mean follow-up period was 7.1 months. The mean back VAS, lower extremity VAS, ODI, and RMDQ at the final follow-up were improved from 5.4±2.4 to 2.0±0.9, 7.0±1.1 to 1.6±1.7, 64.2±11.8 to 44.2±10.6, and from 17.5±4.2 to 12.9±4.0.
Conclusion A new combination technique of OLIF and BESS for direct decompression can be regarded as effective alternative procedure to treat the foraminal and central stenotic lesions of lumbar degenerative disease.
Many techniques have been introduced and performed, with different strengths and benefits. The lateral lumbar interbody fusion techniques (direct lateral lumbar interbody fusion [DLIF] and oblique lateral interbody fusion [OLIF]) have yielded good results for elderly patients. These are useful options for elderly patients with high risk of complications with traditional approaches.
A 77-year-old female suffering from severe degenerative scoliosis, spinal stenosis and lumbar disc herniation underwent Direct lateral lumbar interbody fusion (DLIF) at L2-4. On the 3rd postoperative day, she complained of severe back pain without any trauma history. Simple radiograph revealed L3 vertebral fracture and cage subsidence.
Pain was subsided after conservative treatment including TLSO and medication. Radiographic union was achieved at fractured vertebra after 3 months. Solid fusion was observed at operated level after 6 months. Patient has visited our clinic without any pain. DLIF is one of novel minimally invasive spine procedures available today. It is designed to maximize benefits and minimize risks of other traditional techniques such as anterior approach and posterior approach. However, there can be some risk of cage subsidence and vertebral fracture after DLIF. Therefore, care should be taken to avoid cage subsidence during the operation.
Minimally invasive TLIF has been reported to be a useful treatment option for the patients with various degenerative lumbar diseases. Many studies have reported the favorable clinical results of MIS TLIF. However it remains technically demanding, leading to higher complication rates and longer operative times during the early period of the learning curve. It showed some potential complications due to small working space and visual field. In this study, authors tried to find out various possible complications and some tips avoiding these complications through the review of various articles and authors’ clinical experiences. In many studies, the general complication fusion rates of MIS TLIF have been reported to be similar to that of open fusion. The technical difficulty of the procedure, combined with inadequate training, is evident in initial studies of MIS TLIF. A difficult learning curve of MIS TLIF demands that surgeons have sufficient preclinical training, and education is obtained before the application of MIS TLIF in clinical practice.
Purpose To assess the volume of fusion mass after posterior lumbar interbody fusion (PLIF) using Hounsfield units methods.
Methods The present study was within the frame work about a prospective observational cohort study to compare the surgical outcomes of a single-level PLIF for LSS between the local bone (LbG) and local bone plus hydroxyapatite groups (LbHa). The fusion material for each case was determined by the amount of available local bone. After the fusion material was chosen, patients were assigned to either the LbG group (n=20) or the LbHa group (n=20). The primary outcome was the assessment of fusion mass volume in each group.
Results We used the new method using Hounsfield units for volumetric assessments of interbody fusion mass. There was no difference in fusion rates or volume of the fusion mass between the 2 groups.
Conclusions Hounsfield unit method, that is the CT-based summation method using a cross-sectional slice, can be applied usefully to other areas of orthopaedics.
Purpose To evaluate the method of inserting cortical bone trajectory pedicle screws (cortical screws) and potential complications when performing lumbar fusion.
Methods Lumbar fusion with cortical screw fixation in the hard cortical bone of the pars interarticularis of vertebrae was introduced to replace conventional pedicle screws. We review the literature on the biomechanics of cortical screw insertion and on the clinical outcomes.
Results In vitro biomechanical testing has shown that cortical screws have greater pullout strength than traditional pedicle screws due to the strong bone–screw interface in cortical bone. Cortical screws have the advantages of requiring minimal muscle dissection and shortening the surgery. However, early screw loosening and loss of reduction have been reported.
Conclusions When inserting cortical screws, the entry point and trajectory of the screws are important and a meticulous surgical technique is needed to prevent potential screw-related complications.
Objectives The aim of this study was to monitor the quality control of pedicle screw fixation using a cumulative summation test (CUSUM).
Overview of Literature: CUSUM test has already been used in several different surgical settings including the assessment of outcomes in transplant, laparoscopic, and total hip replacement surgeries. However, there has been no data regarding CUSUM analysis for spine surgery.
Methods Patients with lumbar spinal stenosis who underwent lumbar fusion surgery were included in this study.
The primary outcome was the CUSUM analysis for monitoring the quality control of the accuracy of pedicle screw insertion.
Results Seven screws of the 100 pedicle screw insertions were considered to have failed in the lumbar fusion surgery, respectively. Throughout the monitoring period, there was no indication by the CUSUM test that the quality of performance of the pedicle screw fixation procedure was inadequate.
Conclusions Thisstudy demonstrates the CUSUM test can be a useful tool for monitoring of the quality of procedures related with spine surgery.
Purpose of study: The purpose of this study is to evaluate the effect of blow flow originated from transverse process after posterolateral lumbar fusion (PLF) in rabbit.
Materials and Methods Bilateral PLFs using autogenous iliac bone, 3 mm3 on each operated site, were done in 20 rabbits. In group A, PLFs were done on the decorticated transverse processes. In group B, no decortications were done before PLFs. In group C, PLFs were done after application of Bone wax® on the transverse processes. In group D, PLFs were done after application of Surgicel® on the decorticated transverse processes. The five rabbits and 10 operated sites were used in each group. The computed tomography (CT) was done for each group at postoperative 6 and 12 weeks. To evaluate bony union, the status of PLF was divided into ‘union’ and ‘nonunion’ . And, the volumes of grafted bones were counted at each follow up period in each group. The values were analysed statistically.
Results The union rates of PLFs were observed 90% in group A, 80% in group B, 20% in group C, 70% in group D.
Group C showed lowest union rate than other group with statistical signification (p<0.05). The of volumes of grafted bones at postoperative 6 weeks were calculated to 2.8±0.2 mm3 , 2.6±0.3 mm3 , 1.6±0.8 mm3 , 1.8±0.7 mm3 in group A, B, C, D, retrospectively. At postoperative 12 weeks, the volumes were checked as 2.1±0.6 mm3 , 1.8±0.5 mm3 , 1.2±0.9 mm3 , 1.6±0.4 mm3 in group A, B, C, D, retrospectively. The volumes of grafted bones were checked in order to group A, B, D, and C at 6 and 12 weeks postoperatively. And the volumes in group C were mostly reduced at postoperative 6 and 12 weeks (p<0.05). In group C and D, there were statistically significant reduction in volumes of grafted bones at each follow up period comparing to group A and B (p<0.05).
Conclusions In the PLF of rabbit, the transverse process-grafted bone contact and blood flow originated from transverse process may play major roles in bony union. Among them, the blood flow originated from transverse process might be more important than the bony contact in the union process of PLF.
Extreme lateral interbody fusion (XLIF) and direct lateral interbody fusion (DLIF) are novel minimally invasive transpsoas approaches to the lumbar spine for performing fusions. Advantages of DLIF include easier technique, faster recovery, minimal complication, high fusion rate, and possibility of achieving better alignment. Many previous reports have evaluated outcomes of DLIF. The authors described surgical procedure of DLIF and reviewed clinical outcomes, radiological outcomes, and complications from various literatures. In conclusion, the DLIF seems to be a valuable minimally invasive surgical tool for the fusion in patients with various diseases, including degenerative disc disease, instability, stenosis, scoliosis, tumor, infection, and adjacent segment degeneration.
Intraoperative blood loss volume increases due to soft tissue injury or excessive traction generated by extensive approach including posterior fusion or posterior lumbar interbody fusion, leading to the occurrence of complication and delay in postoperative recovery, On the other hand, MI-TLIF minimizes injuries in soft tissue and surrounding muscle by approaching between multifidus muscles and longissimus dorsi after separating them, and reaching intervertebral disc from lateral vertebral foramen. The advantages of this surgical procedure are minimization of muscle or soft tissue injuries incurred by lateral approach, reduction of surgically related muscle damage, and decrease of postoperative blood loss. However, The size of cages are limited by transforaminal approach in MI-TLIF, eventually it could be difficult to maintain the correction of deformity(disc height, segmental and lumbar lordosis).
Recently, DLIF(Direct lateral interbody fusion) is developed to improve the disadvantages of TLIF. DLIF allows to insert larger cage than TLIF, as a result larger cage have a advantage to maintain correction of disc height and lordosis because it can support both apophyseal rings of endplates.
However, Transpsoas approach is essential for DLIF, so we need to understand the anatomy lumbosacral plexus in psoas, because nerve injury during the transpsoas approach is the most common and potentially the most devastating complication of the DLIF procedure. And many authors reported that various frequency of nerve injury according to surgeon’s skill. Therefore, surgeon’s skill and accurate understanding about the procedure are important factors to prevent the complications of DLIF.
Introduction Recently, minimally invasive lateral approach for the lumbar spine is revived and getting popularity under the name of XLIF or DLIF by modification of mini-open method using sequential tubular dilator and special expandable retractor system.
Purpose s: The purposes of this study were to introduce the mini-open lateral approach for the anterior lumbar interbody fusion (ALIF), and to investigate the advantages, technical pitfalls and complications & to provide basic knowledge on XLIF or DLIF
Materials and Methods Seventy-four patients who underwent surgery by the mini-open lateral approach from September 2000 to April 2008 with various disease entities were included. Blood loss, operation time, incision size, postoperative time to mobilization, length of hospital stay, technical problems and complications were analyzed.
Results With this approach, we can reach form T12 to L5 subdiaphragmatically. The blood loss and operation time of patients who underwent simple ALIF were 61.2 ml and 86 minutes for one level, 107 ml and 106 minutes for two levels, 250 ml and 142.8 minutes for three levels, and 400 ml and 190 minutes for four levels of fusion, respectively.
The incision sizes were on average 4.5cm for one level, 6.3 cm for two levels, 8.5 cm for three levels and 10.0 cm for four levels of fusion. The complications were retroperitoneal hematoma in two cases, pneumonia in one case and transient lumbosacral plexus palsy in three cases.
Conclusion The mini-open lateral approach is simpler & safer than XLIF or DLIF with very short learning curve. Trial of mini-open lateral approach would be helpful before trial of XLIF or DLIF. However, special attention is required to complications such as transient lumbosacral plexus palsy.
Purpose The purpose of this study is to decrease the frequency of the perioperative complication and improve the clinical outcomes of multilevel lumbar degenerative disease by multilevel minimally invasive transforaminal lumbar interbody fusion.
Materials and Methods 317 patients(Minimally invasive transforaminal lumbar interbody fusion : 161, Conventional open surgery : 156) were followed up for more than 1 year. The age of each patient, the amount of intraoperative blood loss, the postoperative drainage, the transfusion requirement, surgery time, using of Intensive care unit, ambulation day, admission day and perioperative complications were investigated and analyzed.
Results Minimally invasive transforaminal lumbar interbody fusion was found to have a less blood loss, less using of Intensive care unit. And as the levels of union increase, disparities were increased(p<0.05).
But, surgery time of Minimally invasive transforaminal lumbar interbody fusion was longer, and as the levels of union increase, disparities were increased(p<0.05).
Conclusions Multilevel Minimally invasive transforaminal lumbar interbody fusion can be the better way, If surgery time of Multilevel Minimally invasive transforaminal lumbar interbody fusion can be reduced.
Purpose Anterior lumbar interbody fusion (ALIF) is widely accepted surgical technique in the treatment of lumbar degenerative disc disease, especially with foraminal stenosis. But many surgeons suspect the effectiveness of ALIF in one or multi-level lumbar degenerative disease. The aim of this study is to evaluate the effectiveness of the two-level ALIF in lumbar degenerative disease.
Materials and Methods Included were the patients who had foraminal stenosis or spinal stenosis with segmental instability (e.g. spondylolisthesis). All patients were studied with plain radiographs and MRI before surgery and plain radiographs at 1 week, 6, 12 and 24 months after surgery. Radiographic measurements included disc height, global lumbar lordosis and existence of lateral fusion mass. To investigate the changes in lumbar global lordosis, the Cobb angle was evaluated on pre- and postoperative standing lateral radiographs from L1 superior endplate to S1 endplate.
Union was defined as the presence of trabecular osseous continuity and/or less than 4° mobility between the segments on a flexion and extension radiograph. Details of blood loss, operative time, transfusions during hospitalization, hospital day, and perioperative complications were evaluated. Clinical outcomes were assessed using Visual Analogue Scale (VAS) scores for leg and back pain and Oswestry disability index (ODI) before surgery and at 6, 12 and 24 months after surgery. Paired t-test was used for statistical analysis.
Results 37 patients (10 men and 27 women; age 33-76 years, mean 61.1 years) who had undergone ALIF combined with PLF or percutaneous pedicle screw fixation (PPF) during January 2007 and January 2009 were studied retrospectively. The mean follow-up period was 34.2 months (48-25 months). The affected levels were L3-4-5 in 14 cases and L4-5-S1 in 23 cases. The average hospital days are 10.7 days, showing no difference between PLF and PPF surgery. The average operation time is 286 minutes. Blood loss was variable from 130 mL to 1200 mL (average 621.2 mL). But Blood loss during the ALIF operation was minimal. (220 mL ; range 120-540 mL). Global lumbar lordosis was improved from 29.2 to 37.8. Postoperatively all patients had relief of sciatic pain, and there were no techniqueassociated complications. Complications included sensory deficit (hypo/dysesthesia) in 4 patients, DVT in one patient, ileus in one patient and transient sympathetic symptom in 11 patients. Two patients had wound problem but were treated easily. The VAS score in leg pain was improved from 6.9 to 2.3 with statistical significance at 24 months after surgery. Also, ODI score was decreased from 30.8 to 9.2 significantly at 24 months after surgery. Radiologic evidence of solid fusion was observed in all patients on the basis of motion and screw loosening. The lateral bone mass was observed bilaterally in 26 of the 28 patients (92%). Radiologic ASD was found in 10/37(27%), but only one patient showed symptom and had minor surgery.
Conclusion ALIF is an effective surgical strategy for the treatment of two-level lumbar degenerative disease and could be a useful alternative to posterior fusion surgery.
Protecting cranially located facet joints during pedicle screw placement is one of the modifiable factors that could prevent possible adjacent level problems related with spinal fusion procedure. Placing pedicle screws percutaneously appears to be more challenging in the technical aspect than performing with traditional open technique because of its limited selecting entry point for screw placement. The authors have reported surprisingly higher incidence and risk factors of cranial facet joint violations by percutaneously placed pedicle screws. The purpose of this literature was to illustrate the surgical technique focusing on the tips to avoid cranial facet joint violation during percutaneous placement of pedicle screws.

 First
First Prev
Prev

