Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
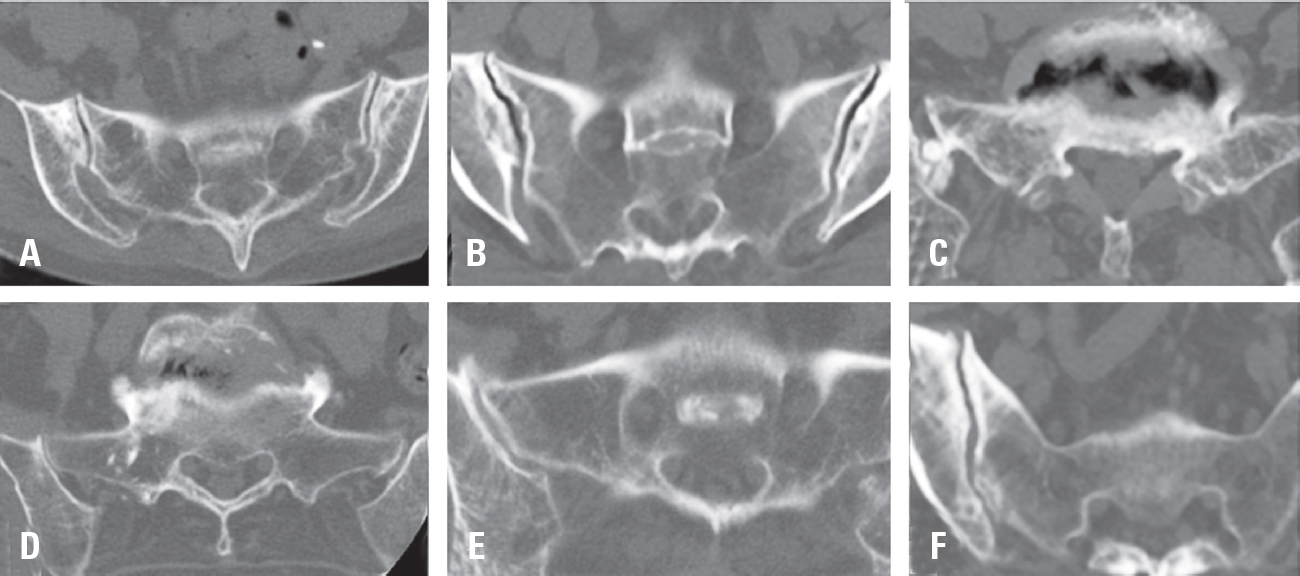
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
Purpose To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
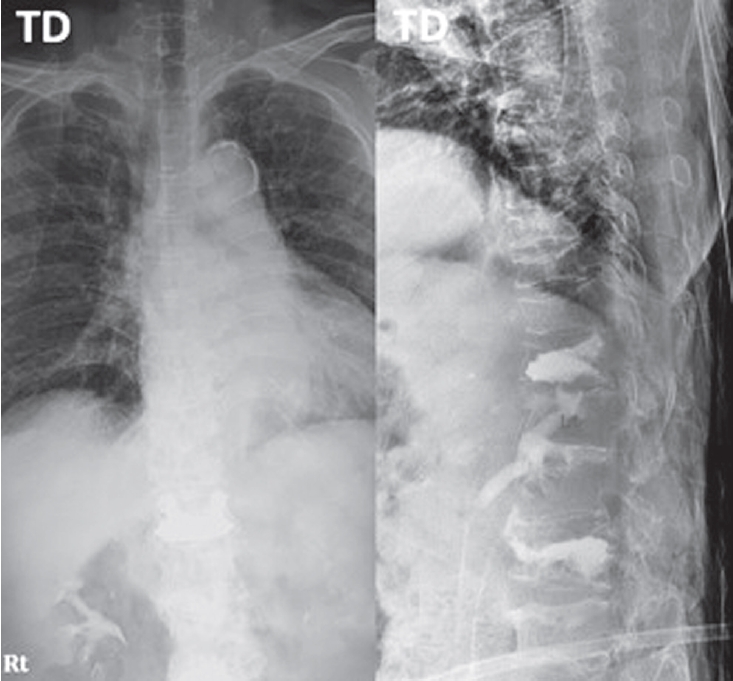
Methods An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
Purpose Metabolic syndrome is a multifactorial condition associated with increased risks of cardiovascular disease and type 2 diabetes. This study aims to evaluate whether combining AI-based abdominal CT metrics with traditional InBody analysis enhances the prediction of metabolic syndrome.
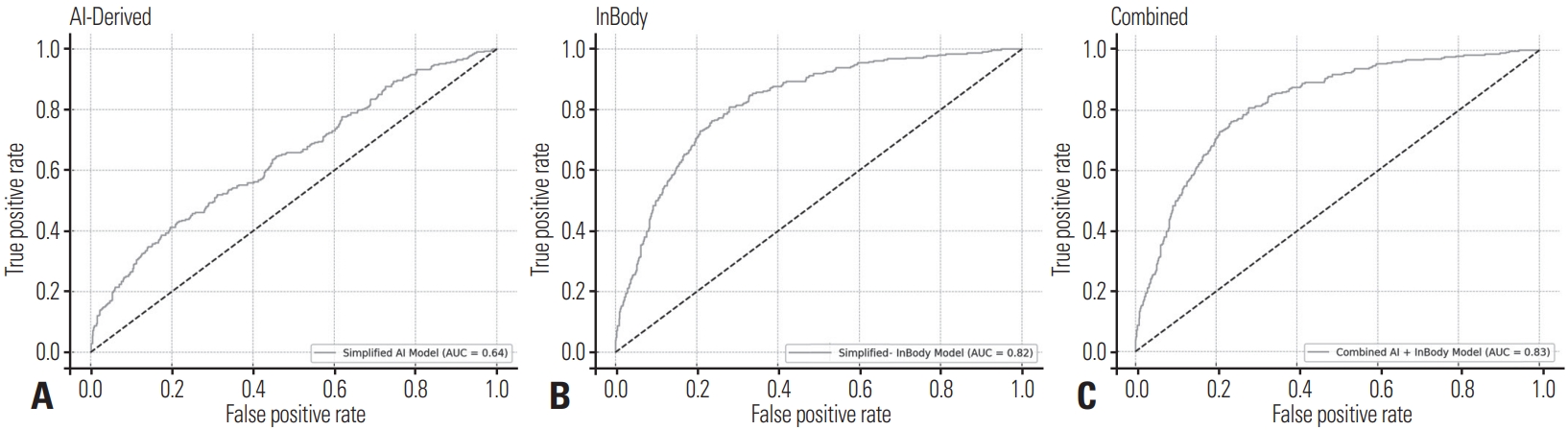
Materials and Methods This retrospective study included 977 adults who underwent both abdominal CT and InBody assessments. AI-derived measurements were obtained using a deep-learning V-Net model trained to segment seven body tissue types. InBody measurements included BMI, body fat percentage, fat mass, and waist-hip ratio. Metabolic syndrome was defined by NCEP-ATP III criteria. Logistic regression and ROC analyses were used to evaluate the predictive performance of AI-derived metrics, InBody metrics, and their combination.
Results Body fat percentage and waist-hip ratio from InBody analysis were strong predictors of metabolic syndrome (AUC 0.82). AI-derived visceral fat was also significantly associated with metabolic syndrome (AUC 0.61). Combining both AI and InBody metrics slightly improved predictive performance (AUC 0.83), indicating a complementary diagnostic value.
Conclusions While InBody metrics remain superior in predicting metabolic syndrome due to their close association with metabolic processes, AI-derived body composition metrics, particularly visceral fat, offer structural insights. The modest improvement in prediction when combined suggests the potential of an integrated diagnostic model in clinical practice.
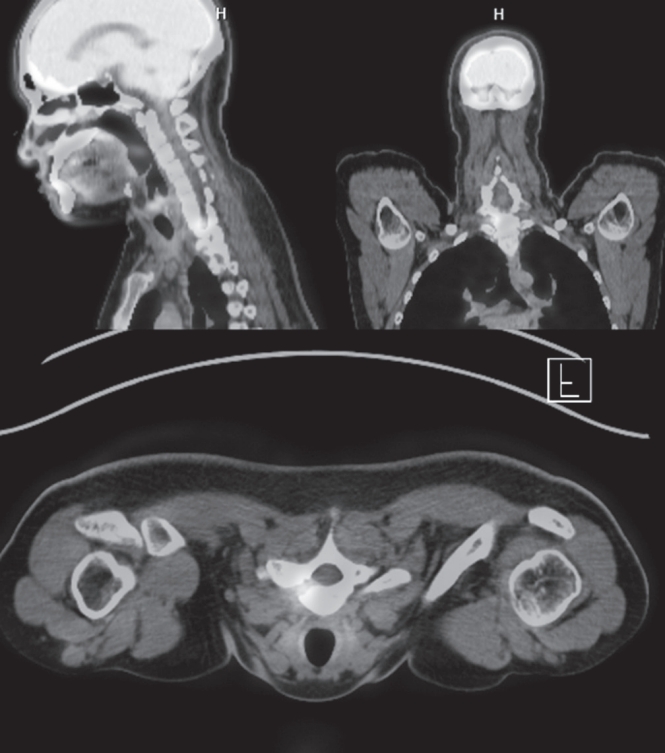
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Objective To investigate the association of quantitative paraspinal muscle measurements to the Oswestry disability index (ODI) in patients with lumbar spondylolisthesis.
Materials and Methods Ninety two patients (mean age, 61.6 years; male, mean age, 71.8 years ; female; mean body mass index [BMI], 24.9 kg/m2 ) who had undergone lumbar fusion due to spondylolisthesis with available selfcompleted postoperative ODI were included. The total cross-sectional area (CSA) and functional CSA (FCSA; i.e., area containing only lean muscle tissue) of the paraspinal muscle group (multifidus and erector spinae muscles) and the psoas muscles were measured at L2–L3, L3–L4, and L4–L5 disc levels each on preoperative magnetic resonance imaging (MRI) and the sum of areas at each level served as representative values for each muscle. The FCSA/total CSA ratio and the skeletal muscle index (SMI=muscle area [cm2 ]/patient height2 [m2 ]) were calculated.
Pearson’s correlation analyses were performed to evaluate the relationship between preoperative paraspinal muscle measurements and postoperative ODI.
Results Quantitative values of low paraspinal muscle showed significant correlation with high ODI values. As a result of this study, the preoperative paraspinal muscle was quantified in the group of patients undergoing spinal fusion.
Patients with low value in CSA and FCSA of paraspinal muscle could observe the tendency to transition to low clinical outcomes. Therefore, quantitative values of surrounding muscles are factors affecting clinical outcomes of patients undergoing spinal surgery Conclusion: Smaller muscle bulk (total CSA) of psoas muscles and lean muscle mass (FCSA) of paraspinal muscle group and psoas muscles combined on preoperative MRI were associated with significant postoperative disability based on ODI in patients with lumbar spondylolisthesis.
Purpose To evaluate and analyze the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor between recurrence and non-recurrence group, and to assess the merits of minimally invasive spinal surgery.
Overview of Literature: No large registry study has so far investigated the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor.
Methods From July 2003 to April 2011 we retrospectively studied a consecutive series of 156 patients who underwent lumbar microdiscectomy using minimally invasive tubular retractor. The following data were collected: clinical outcomes, operative time, intraoperative blood loss, recurrence, and complications. The clinical outcomes were measured using a visual analog scale (VAS) and assessed by the modified MacNab criteria.
Results Minimally invasive tubular microdiscectomy was performed in 156 patients. The clinical outcomes assessed by MacNab criteria were excellent in 63 patients (40%), good in 71 patients (45%). VAS scores of low-back pain decreased from a mean of 6.7 prior to surgery to 2.5 after surgery, and that of leg pain decreased from 7.2 to 2.1. The average operative time was 68 minutes (range, 25 to 180 minutes). The average blood loss was 42 mL (range, 0 to 500 mL). None of the patients needed blood replacement. One patient had wound infection problem but there was no dural tear case. Twenty-two patients had recurrence. Average time to recurrence was about 42 months. Seventeen cases recurred at the same level and five cases recurred at the adjacent level. Eleven cases in 22 patients with recurrence were contained disc type and the others were non-contained disc type. Eighteen cases in 22 patients with recurrence were paracentral disc herniation type and the others were far lateral type. Average body mass index (BMI) of recurrence cases was 24.7 (range, 17.5 to 31.3) and that of non-recurrence cases was 24.5 (range, 16.3 to 39.2).
Conclusions Lumbar microdiscectomy using tubular retractor can offer a useful modality for the treatment of lumbar herniated disc with the merits of minimally invasive spinal surgery. Further randomized, prospective investigations are needed to fully evaluate the impact of this technique.
Background Context: There are few reports of changes in global sagittal alignment and corresponding factors like hand grip strength (HGS) and muscle performance tests to detect changes in global sagittal alignment after surgery for lumbar spinal stenosis (LSS).
Purpose The purpose of the study was to determine whether HGS can be a useful predictive marker of global sagittal alignment changes after decompression with fusion surgery for LSS.
Study Design: This is a retrospective observational study.
Patient Sample: Patients who underwent spine surgery for LSS were included in the present study.
Outcome Measures: Radiological spinopelvic parameters including sagittal vertical axis (SVA), lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), global tilt (GT), and T1 pelvic angle (T1PA) were assessed. Clinical outcomes parameters like Oswestry Disability Index (ODI), Euro-QOL (EQ-5D), visual analog scale (VAS) scores for back or leg pain were assessed. To assess muscle performance, three functional mobility tests (6-meter walk test, timed up and go test, sit-to-stand test) and HGS were checked.
Materials and Methods A total 91 consecutive patients who underwent spine fusion surgery for LSS were included. 1 year after posterior decompression and fusion surgery, the patients were further classified into four groups according to preoperative and postoperative SVA. We analyzed radiological parameters like SVA, LL, PT, PI, GT, and T1PA. The ODI, the EQ-5D and VAS scores for back or leg pain were recorded as clinical outcomes assessment. To assess muscle performance, SMT, TUGT, STS, and HGS were checked.
Results HGS was significantly correlated with age, postoperative SVA, ODI, EQ-5D and muscle performance test. HGS was related with change of preoperative sagittal alignment 1yr after surgery. Using a receiver operating characteristic (ROC) curve to determine the cutoff values of HGS as predictors of postoperative balanced sagittal alignment according to SVA, cutoff value of HGS demonstrated 19.5 kg with a sensitivity of 82.1% and specificity of 66.7%.
Conclusion Patients with non-balanced sagittal alignment in LSS demonstrated decreased muscle function and muscle strength. If the muscle strength was weak in the group in which the sagittal balance was maintained preoperatively, it could be converted to non-balanced sagittal alignment. Thus, preoperative HGS may be a good predictor of postoperative SVA change.

 First
First Prev
Prev

