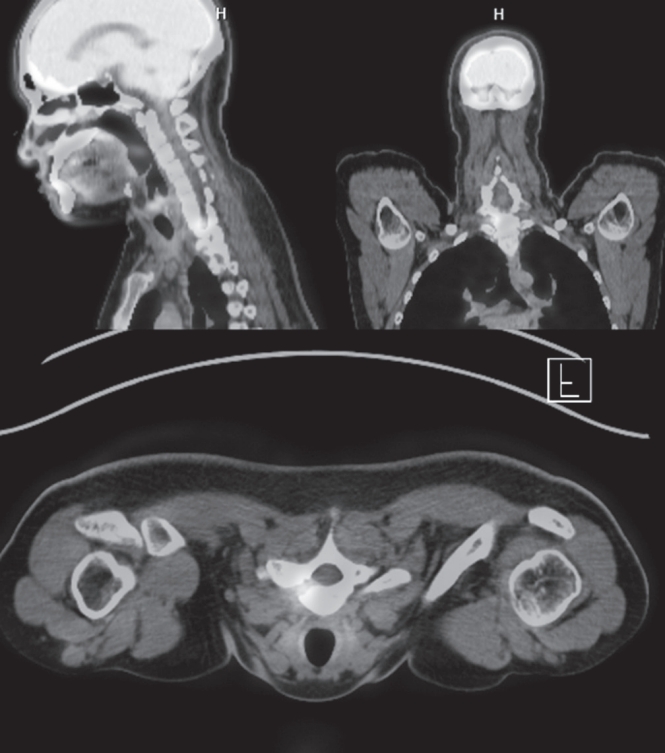
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Purpose To evaluate whether the contralateral radiating pain improved after unilateral decompression and minimally invasive transforaminal lumbar interbody fusion (TLIF) in the patients with bilateral radiating pain due to degenerative lumbar disease.
Materials and Methods Patients with the degenerative lumbar disease who underwent unilateral minimally invasive TLIF and were followed for more than 1 year were included. Clinically, low back pain and radiating pain on the dominant symptom side and the contralateral side were evaluated by the visual analogue score (VAS), and the Oswestry disability index (ODI) score was also evaluated.
Results ODI and VAS of low back pain and radiating pain were effectively reduced in a total of 57 cases. Thirty cases having bilateral radiating pain, among these patients, unilateral decompression was performed in 15 cases and bilateral decompression thru unilateral approach in 15 patients. In unilateral decompression group, radiating pain on the dominant symptom side, and radiating pain on the contralateral side were also improved at the final followup. In 15 cases who underwent bilateral decompression, radiating pain on the dominant symptom side and the contralateral side were improved at the final follow-up. There was no significant difference between the two groups in terms of preoperative ODI, VAS of low back and radiating pain.
Conclusions Minimally invasive TLIF via unilateral approach with or without contralateral decompression showed good clinical results in patients having unilateral or bilateral radiating pain. Minimally invasive TLIF could be an useful option even if there is bilateral radiating pain in degenerative lumbar disease.
Purpose Spinal fusion is useful method of treatment of degenerative lumbar diseases, and is divided into anterior and posterior surgery. Each approach has advangages and disadvantages. Recently, minimally invasive lateral lumbar interbody fusion (LLIF) supplemented disadvantages of anterior and posterior surgery is interested. We introduce LLIF and present about application and indication of LLIF.
Materials and Methods A 76-year-old female was diagnosed by degenerative disc disease on L2-3. A 66-year-old male was diagnosed by central spinal stenosis on L2-3-4-5. A 86-year-old female was diagnosed by foraminal stenosis on L3-4-5 and degenerative scoliosis. A 73-year-old male was diagnosed by spinal stenosis on L3-4-5 and spondylolisthesis. A 70-year-old male was diagnosed nonunion on L4-5. On past history, the patient was operated by fusion because of L2 burst fracture. A 75-year-old female was diagnosed by infective spondylodiscitis on L3-4.
Results Degenerative disc disease, severe central and foraminal spinal stenosis, degenerative scoliosis, spondylolisthesis and infective spondylodiscitis were application and indication of LLIF.
Conclusions LLIF merges the advantages and covers the disadvantages of anterior and posterior surgery. However, approach-related lumbar plexus injury and L5-S1 approach were remained obstacles.
Numerous improvements in minimally invasive spine surgery (MISS) have been made during the past decade.
Classic treatment methods have reserved surgical intervention for trauma patients with neurological compromises or instability. When used in thoracolumbar spine trauma management, MISS should achieve the similar results as classic treatment with less morbidity.(1) In the past decade, minimally invasive surgical (MIS) techniques for spine surgery have been increasingly used. The goal of minimally invasive surgery is to decrease surgical morbidity through decreased soft-tissue dissection providing similar structural stability as classic techniques. An increasing number of studies is reporting good clinical and radiographic outcomes with MIS techniques. However, the literature is lacking high-quality evidence comparing these newer techniques to classic treatments. In the future, development of techniques can expand the indications and treatment possibilities in spine trauma treatment. We reviewed the current literatures to clarify the indications of minimally invasive techniques with spinal trauma.
Objective This study aimed to describe the surgical technique in patients with cervical herniated disc treated with unilateral biportal endoscopic spinal surgery.
Materials and Methods Working and viewing portals were created in each unilateral paravertebral area at the target disc level. Under exploring by endoscopic view, effective decompression was possible via safe access to the medial foramen with minimal laminectomy and facetectomy. We evaluated 27 patients, and clinical outcome was analyzed using the visual analogue scale (VAS), Neck disability index (NDI), Macnab criteria, and motor function of involved upper extremity, all assessed before and 3, 6 months post procedure.
Results The VASs for axial neck pain and upper extremity pain decreased from 6.8 to 1.9 and 7.7 to 1.5, respectively, at 6 months post procedure. The NDIs were improved from 45.5 to 13.0 at 6 months post procedure. According to the Macnab criteria, an ‘Excellent’ , ‘Good’ , and ‘Fair’ result was obtained in 55.6%, 29.6%, and 14.8% subjects, respectively.
The motor power of involved upper extremity improved as an approximately one grade on average at 6 months post procedure; 3.9±0.8 to 4.8±0.4.
Conclusions Unilateral biportal endoscopic spinal cervical surgery can be an efficient and safe intervention in patients with cervical herniated disc.
Purpose To evaluate and analyze the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor between recurrence and non-recurrence group, and to assess the merits of minimally invasive spinal surgery.
Overview of Literature: No large registry study has so far investigated the clinical results of lumbar microdiscectomy using minimally invasive tubular retractor.
Methods From July 2003 to April 2011 we retrospectively studied a consecutive series of 156 patients who underwent lumbar microdiscectomy using minimally invasive tubular retractor. The following data were collected: clinical outcomes, operative time, intraoperative blood loss, recurrence, and complications. The clinical outcomes were measured using a visual analog scale (VAS) and assessed by the modified MacNab criteria.
Results Minimally invasive tubular microdiscectomy was performed in 156 patients. The clinical outcomes assessed by MacNab criteria were excellent in 63 patients (40%), good in 71 patients (45%). VAS scores of low-back pain decreased from a mean of 6.7 prior to surgery to 2.5 after surgery, and that of leg pain decreased from 7.2 to 2.1. The average operative time was 68 minutes (range, 25 to 180 minutes). The average blood loss was 42 mL (range, 0 to 500 mL). None of the patients needed blood replacement. One patient had wound infection problem but there was no dural tear case. Twenty-two patients had recurrence. Average time to recurrence was about 42 months. Seventeen cases recurred at the same level and five cases recurred at the adjacent level. Eleven cases in 22 patients with recurrence were contained disc type and the others were non-contained disc type. Eighteen cases in 22 patients with recurrence were paracentral disc herniation type and the others were far lateral type. Average body mass index (BMI) of recurrence cases was 24.7 (range, 17.5 to 31.3) and that of non-recurrence cases was 24.5 (range, 16.3 to 39.2).
Conclusions Lumbar microdiscectomy using tubular retractor can offer a useful modality for the treatment of lumbar herniated disc with the merits of minimally invasive spinal surgery. Further randomized, prospective investigations are needed to fully evaluate the impact of this technique.
Recently, favorable results of minimally invasive spinal surgery have been reported in comparison to the open decompression or fusion surgery. Biportal endoscopic spine surgery (BESS) has several benefits and Indications for BESS are nearly identical to those for general open spinal surgery. However, it remains a challenging procedure even for an experienced endoscopic surgeon. because it takes a a long operation time while early learning period. If the operation time is prolonged, the advantages of endoscopic surgery are reduced and the incidence of complications can be increased. Therefore, we will investigate the factors affecting the operation time and how to minimize it before and during operation.
Purpose of Study: Purpose of this study is to summarize the technique of UBE surgery in lumbar interbody fusion and review the clinical outcomes and complications of UBE surgery in lumbar interbody fusion.
Materials and Methods Medical databases were searched for the key words of unilateral biportal endoscopic surgery and lumbar spinal stenosis using PubMed from 2005 to the present.
Conclusion UBE spinal surgery is a new technique that can be a feasible alternative and an effective treatment modality for spinal degenerative diseases and can achieve the necessary surgical skills for experienced microscopic surgeons, which is still expanding the indications for lumbar spinal surgery.
Background Owing to its new introduction, there are few documents on pit-falls of biportal endoscopic spine surgery (BESS) clinically. The authors reported etiologies in need of early exploration after BESS for lumbar degenerative diseases and strategies to overcome them.
Methods BESS were performed for lumbar spine diseases (LSDs) by two spine surgeons from December 2013 to March 2016. Postoperative MRI was checked for all cases and following-up MRIs in the case in need of revision surgery within six months after the first surgery due to pain intolerable, sustained or recurred. The complicated cases were reviewed and classified as radiographic and operative findings to reveal the main reasons for early explorations.
Results The 562 cases (M:295, F:267, Age 58.5±14.1 yrs, 20~88 yrs) included lumbar disc herniation (LDH) (255 cases), extraforaminal disc herniation (22 cases), spinal stenosis (218 cases), degenerative spondylolisthesis (27 cases), revision surgery after recurred disc herniation or restenosis after open surgery (24 cases), juxtafacet cyst (11 cases), adjacent segment stenosis with fusion surgery (3 cases), and spondylolytic spondylolisthesis (2 cases). Early explorations were needed in 43 cases (7.7%) at 26.1±31.5 days after the initial operations. Causative etiologies were listed as recurred LDH (12 cases, 27.9%), remnant stenosis (7 cases, 16.3%), remained ruptured disc fragment (6 cases, 14.0%), root edema (5 cases, 11.6%), synovitis (4 cases, 9.3%), hematoma (3 cases, 7.0%), dura tear (2 cases, 4.7%), recurred stenosis (2 cases. 4.7%), wrong level (1 case, 2.3%) and postoperative fungal infection (1 case, 2.3%).
Thirty-one cases (72.1%) were revised within 4 weeks and most conditions (40 cases, 93.0%) were improved after early exploration using BESS. Two cases of dura tear were conversed to open repair. One case of fungal infection was suspected to related with the patient’s medical illness including long-term steroid use for chronic lung disease with pulmonary fibrosis and Diabetes mellitus.
Conclusions Preoperative planning should be prepared carefully to decrease early exploration. It was helpful to comparing MRIs immediately postoperative and early following-up to find the reasons. Don’t hesitate to explore the operated site again using BESS, because most etiologies are supposed to be controlled by early exploration without need of converting to open surgery except in the case of dura tear in need of dural repair.
Minimally invasive TLIF has been reported to be a useful treatment option for the patients with various degenerative lumbar diseases. Many studies have reported the favorable clinical results of MIS TLIF. However it remains technically demanding, leading to higher complication rates and longer operative times during the early period of the learning curve. It showed some potential complications due to small working space and visual field. In this study, authors tried to find out various possible complications and some tips avoiding these complications through the review of various articles and authors’ clinical experiences. In many studies, the general complication fusion rates of MIS TLIF have been reported to be similar to that of open fusion. The technical difficulty of the procedure, combined with inadequate training, is evident in initial studies of MIS TLIF. A difficult learning curve of MIS TLIF demands that surgeons have sufficient preclinical training, and education is obtained before the application of MIS TLIF in clinical practice.
The minimally invasive technique to correct deformity in scoliosis is not a familiar concept among spine surgeons but is interesting, as this innovative surgery, if it proves successful, will have the advantages of the minimally invasive technique in the final outcomes and will be the future of scoliosis surgery. We operated on 18 adolescent idiopathic scoliosis (AIS) patients using a newly designed technique which utilizes two or three 1-inch midline incisions to insert pedicle screws with a rod, facet fusion and de-rotation maneuver to correct the deformity. Post-operative complications were minimal and the results of the deformity corrections were comparable to the open scoliosis surgery in the follow up. The advantages of minimally invasive surgery observed in all cases include cosmetically fainter scars, reduced blood loss, shorter hospital stay, early mobilization and minimal need of analgesics for pain.
Even though many challenges were faced in executing this procedure, the goal of inventing this novel approach was accomplished. We feel this technique is a good alternative to open surgery in certain curve types of AIS but large scale studies are needed in the future to recommend its routine use.
We reviewed literatures relating to minimally invasive lateral lumbar interbody fusion for the treatment of adult degenerative spinal deformity. Most of literatures were retrospective case series with a small numbers of patients.
A prospective multicenter study was published in two separate papers. This procedure was effective in treating the coronal deformity. On the other hand, restoring the sagittal plane remains an issue. Pseudarthrosis was problematic, especially in the cases without use of the human recombinant bone morphogenetic protein-2 (rhBMP-2) and bilateral pedicle screw fixation. Temporary sensory deficits and transient leg weakness was the most common complication after lateral lumbar interbody fusion. Careful patient selection is important for the application of lateral minimally invasive techniques for adult degenerative scoliosis.
Extreme lateral interbody fusion (XLIF) and direct lateral interbody fusion (DLIF) are novel minimally invasive transpsoas approaches to the lumbar spine for performing fusions. Advantages of DLIF include easier technique, faster recovery, minimal complication, high fusion rate, and possibility of achieving better alignment. Many previous reports have evaluated outcomes of DLIF. The authors described surgical procedure of DLIF and reviewed clinical outcomes, radiological outcomes, and complications from various literatures. In conclusion, the DLIF seems to be a valuable minimally invasive surgical tool for the fusion in patients with various diseases, including degenerative disc disease, instability, stenosis, scoliosis, tumor, infection, and adjacent segment degeneration.
Purpose A surgical treatment has been preferred in patients with unstable lumbar spine fracture-dislocation with incomplete paraplegia as it does not cause further nerve injury by regenerating and maintaining the shape of the spinal canal via the accurate reduction of fracture, and prevents additional complications by preventing neurovascular injury that secondarily occurs.1) However, the surgical treatment may be delayed or even impossible in patients with hemodynamic unstable state caused by an emergent concurrent injury. Accordingly, Stage operation was conducted on patients with unstable lumbar spine fracture-dislocation with incomplete paraplegia who had a difficulty in undergo immediate reduction and decompression due to hemodynamic unstable state caused by other concurrent injuries.
Methods Postural reduction and minimal invasive percutaneous pedicle screw fixation L1-4 were conducted as a first stage operation, and L2-3 partial laminectomy, discectomy, and posterior fusion were then conducted as a second stage operation by applying the concept of stage operation in the department of spinal surgery.
Results The first stage operation had a blood loss of 150cc and an operation time of 58 min. Compared to motor grade 3 shown in preoperative status, motor grade 4 was shown in L3 level or lower in a postoperative physical examination. The second stage operation was conducted two weeks later. It had an operation time of 90 min and a blood loss of 500cc. no neurologic change was further found.
Conclusion Stage operation was conducted on patients with hemodynamic unstable state. Postural reduction and minimal invasive percutaneous pedicle screw fixation were conducted as a first stage operation to achieve the immediate reduction and stability of fracture and dislocation and the improvement of neurologic deficits.
Subsequently, decompression or fusion was conducted as a second stage operation under stable systemic status for through and accurate operation.
Purpose The purpose of this study is to decrease the frequency of the perioperative complication and improve the clinical outcomes of multilevel lumbar degenerative disease by multilevel minimally invasive transforaminal lumbar interbody fusion.
Materials and Methods 317 patients(Minimally invasive transforaminal lumbar interbody fusion : 161, Conventional open surgery : 156) were followed up for more than 1 year. The age of each patient, the amount of intraoperative blood loss, the postoperative drainage, the transfusion requirement, surgery time, using of Intensive care unit, ambulation day, admission day and perioperative complications were investigated and analyzed.
Results Minimally invasive transforaminal lumbar interbody fusion was found to have a less blood loss, less using of Intensive care unit. And as the levels of union increase, disparities were increased(p<0.05).
But, surgery time of Minimally invasive transforaminal lumbar interbody fusion was longer, and as the levels of union increase, disparities were increased(p<0.05).
Conclusions Multilevel Minimally invasive transforaminal lumbar interbody fusion can be the better way, If surgery time of Multilevel Minimally invasive transforaminal lumbar interbody fusion can be reduced.
Protecting cranially located facet joints during pedicle screw placement is one of the modifiable factors that could prevent possible adjacent level problems related with spinal fusion procedure. Placing pedicle screws percutaneously appears to be more challenging in the technical aspect than performing with traditional open technique because of its limited selecting entry point for screw placement. The authors have reported surprisingly higher incidence and risk factors of cranial facet joint violations by percutaneously placed pedicle screws. The purpose of this literature was to illustrate the surgical technique focusing on the tips to avoid cranial facet joint violation during percutaneous placement of pedicle screws.

 First
First Prev
Prev

