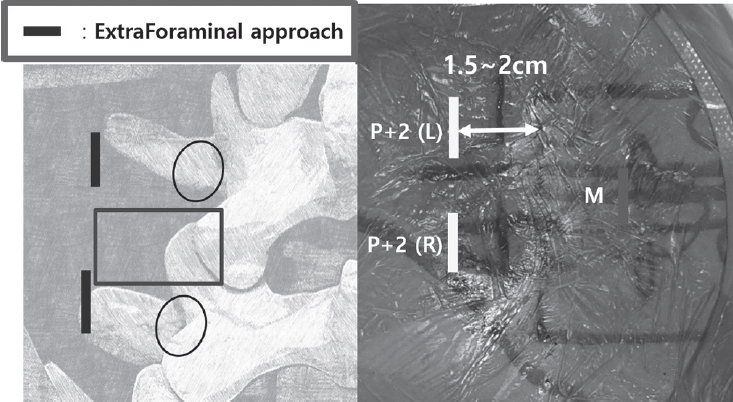
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
Tethered cord syndrome (TCS) is a condition in which the spinal cord becomes pathologically stretched due to various congenital or acquired etiologies, leading to progressive neurological symptoms. While surgical detethering is the gold standard for pediatric patients, adult-onset recurrent TCS presents a significant surgical challenge. Reoperation carries substantial risks—including spinal cord injury, cerebrospinal fluid leakage, and a high rate of retethering—often resulting in suboptimal long-term outcomes. Recently, spine-shortening osteotomy (SSO) has emerged as an alternative technique to reduce spinal cord tension without direct manipulation of the neural elements. Here, we report a case of recurrent adult TCS associated with a lipomyelomeningocele, which was exacerbated by post-traumatic kyphosis from an L1 compression fracture. The patient was successfully treated with SSO at the L1 level. This case highlights the utility of SSO as a safe and effective alternative to conventional revision detethering, particularly in complex cases involving spinal deformity.
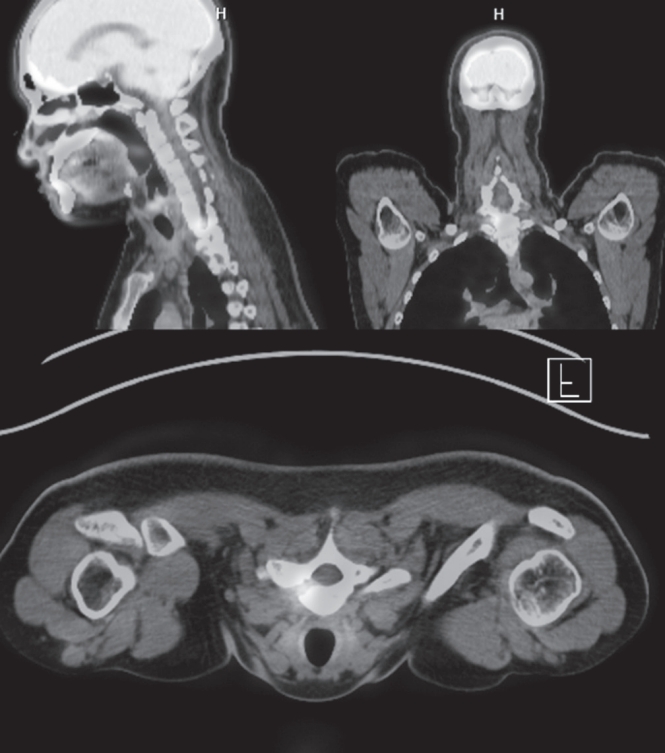
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Purpose This study aimed to compare the clinical effectiveness and potential benefits of ultrasound (US)-guided versus fluoroscopy (FL)-guided cervical retrolaminar block (RLB) in patients with cervical facet joint pain.
Materials and Methods A total of 27 patients aged 40 years or older who were diagnosed with cervical facet joint syndrome based on physical examination and imaging modalities were included. 12 patients of group I treated with US-guided RLB and 15 patients of group II treated with FL-guided RLB. The position of the needle and the distribution of contrast agent were confirmed using fluoroscopic images, and the changes in numeric rating scale (NRS) and neck disability index (NDI) before and 2 weeks after the procedure were compared in the two groups.
Results Radiologically, the target agreement of needle placement in group I was 75%. There was no difference in contrast medium spread between the two groups. Clinically, the mean NRS improved from 7.08±0.52 to 3.08±0.90 in group I (p=0.01) and from 7.20±0.56 to 3.33±0.72 in group II (p=0.01). The mean NDI decreased from 41.67±2.27 before the procedure to 20.83±2.33 after the procedure in group I (p=0.01), and from 40.87±2.61 before the procedure to 21.67±2.02 after the procedure in group II (p=0.01), with no difference between the two groups.
Conclusions US-guided cervical RLB is an effective, radiation-free alternative to FL-guided RLB for managing cervical facet joint pain, offering comparable pain relief and functional improvement.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Purpose The biplanar whole body imaging system (EOS) is a new tool for measuring whole body sagittal alignment in a limited space. This tool may affect the sagittal balance of patients compared to conventional whole spine radiography (WSX). This study is to investigate the difference in sagittal alignment between WSX and EOS.
Materials and Methods We compared spinal and pelvic sagittal parameters in 80 patients who underwent EOS and WSX within one month between July 2018 and September 2019.The patients were divided based on sagittally balanced and imbalanced groups according to pelvic tilt (PT) >20˚, pelvic incidence-lumbar lordosis >10°, C7-sagittal vertical axis (SVA) > 50 mm in WSX.
Results In sagitally imbalanced group, for WSX versus EOS, the pelvic parameters demonstrated compensation in EOS with smaller PT (27.4±11.6° vs. 24.9±10.9°, p=0.003), greater sacral slope (SS), and patients tended to stand more upright with smaller C7-SVA (58.4±17 mm vs. 48.9±57.3 mm, p=0.003), T1-pelvic angle (TPA), T5-T12, and T2-T12.
However, in sagitally balanced group, these differences were less pronounced only with smaller PT (10.8±6.9° vs.
9.4±4.7°, p=0.04), TPA and T2-T12 angle, but SS and C7-SVA were similar (p>0.05).
Conclusions EOS shows a negative SVA shift and lesser pelvic tilt than WSX especially in patients with sagittal imbalance. When making a surgical plan, surgeon should consider these differences between EOS and WSX.
Background Percutaneous-short segment screw fixation (SSSF) without bone fusion has proven to be a safe and effective modality for thoracolumbar spine fractures (TLSFs). When fracture consolidation is confirmed, pedicle screws are no longer essential, but clear indications for screw removal following fracture consolidation have not been established.
Methods In total, we enrolled 31 patients with TLSFs who underwent screw removal following treatment using percutaneous-SSSF without fusion. Plain radiographs, taken at different intervals, measured local kyphosis using Cobb’ angle (CA), vertebra body height (VBH), and the segmental motion angle (SMA). A visual analogue scale (VAS) and the Oswestry disability index (ODI) were applied pre-screw removal and at the last follow-up.
Results The overall mean CA deteriorated by 1.58º (p<0.05) and the overall mean VBH decreased by 0.52 mm (p=0.001). SMA preservation was achieved in 18 patients (58.1%) and kyphotic recurrence occurred in 4 patients (12.9%). SMA preservation was statistically significant in patients who underwent screw removal within 12 months following the primary operation (p=0.002). Kyphotic recurrence occurred in patients with a CA ≥20º at injury (p<0.001) with a median interval of 16.5 months after screw removal. No patients reported worsening pain or an increased ODI score after screw removal.
Conclusion Screw removal within 12 months can be recommended for restoration of SMA with improvement in clinical outcomes. Although, TLSFs with CA ≥20º at the time of injury can help to predict kyphotic recurrence after screw removal, the clinical outcomes are less relevant.
Purpose Minimally invasive technique in spinal surgery have evolved including cortical bone trajectory (CBT) screw technique which is s new lumbar pedicle screw path, as an alternative fixation technique for lumbar spine.
Theoretical advantage is that it provides enhanced screw torque and has biomechanical characteristics, also it minimizes approach-related damages. Midline lumbar fusion (MIDLF) has appeared with CBT screw technique.
Many studies of CBT screw reported the effectiveness of MIDLF. We adopted this technique for lumbar degenerative spondylolisthesis and evaluated early radiological outcomes.
Materials and Methods From May 2014 to March 2015, 17 patients (mean age 65.6±7.5 years; 4 males, 13 females) underwent MIDLF procedures for the treatment of single level lumbar spondylolisthesis. Average follow-up period was 8.8±2.7 months. Initial and last follow-up X-ray and computed tomography (CT) were evaluated for screw malposition, detection of peri-screw halo, loosening of the construct, or signs of spinal instability.
Results The average bone mineral density (BMD) was -1.9±0.8. Eleven patients were fused at L4-5, 5 were at L3-4, and 1 was at L2-3. Five CBT screws were converted into pedicle screws due to intraoperative misposition of screws, so total 63 CBT screws were evaluated for peri-screw halo and malposition. There were no findings of screw pull-out or breakage in all screws. Four out of 63 (6.3%) screws were judged as peri-screw halo, and 20 (41.2%) screws were judged as malposition (1 medial; 2 superior; 17 lateral pedicle violation). But, there were no screw related nerve root injury. In all cases, interbody bony mass were identified. Four out of 17 (23.6%) patients were detected more than 2 degrees motions on flexion-extension lateral X-rays at final follow-up, and 1 out of these 4 patients was identified loss of reduction. There was no operation related complication.
Conclusion There is no doubt that MIDLF with CBT screw is the minimally invasive method. Many numbers of screw malposition identified in our series were thought to be due to our earlier experience of trying free hands technique.
We recommend the use of intraoperative fluoroscopy, which achieve accuracy. Although MIDLF with CBT has theoretical strengths, we must evaluate further long-term clinical follow-up and measure outcome.
Background Oblique and anterior lumbar interbody fusion have been widely performed in the lumbar spinal disease but we cannot get a direct decompression effect with these procedure.
Objective: The purpose of this study is to report clinical and imaging outcomes of microscope assisted direct decompression combined with oblique lumbar interbody fusion (OLIF) or anterior lumbar interbody fusion (ALIF).
Methods Twelve patients who received microscope assisted direct decompression during OLIF or ALIF for lumbar spinal stenosis were enrolled. The OLIF was performed for the lesion upper than the L4-5 or in the case of multisegmental disease. The ALIF was performed for the lesion at the L5-S1. After anterior-approaching surgery, percutaneous fixation of pedicle screw was performed and we did not perform an additional decompression posteriorly in all cases. For the clinical outcomes, we evaluated short form 36 (SF-36), Oswestry disability index (ODI) score and visual analog scale (VAS) pain score. For the imaging outcomes, we obtained postoperative lumbar magnetic resonance imaging (MRI).
Results The OLIF was performed for 9 patients and the ALIF was performed for 3 patients. In the clinical outcomes, SF-36 was improved from 25.40 to 69.83 and ODI score was also improved from 69.83 to 16.50. VAS pain score of back was improved from 4.3 to 1.6 and VAS pain score of leg was improved from 7.5 to 2.2. In the imaging outcomes, all patients had severe stenosis before surgery. After surgery the severity of the stenosis was reduced to mild state in 9 cases and moderate state in 3 cases postoperatively.
Conclusions We could obtain the good clinical outcomes and effective decompression through microscope assisted direct decompression during OLIF or ALIF.
Oblique lumbar interbody fusion (OLIF) is one of surgical techniques for patients with spondylolisthesis, but an insertion of cage at an ideal location (anterior 1/3 of disc space) is challenging for patient with high grade spondylolisthesis, because vertebra are not aligned. Recently, a technique of simultaneous insertion of pedicle screw and rod system from the back of patient and insertion of cage via retroperitoneal route from the front of patient is possible by using spinal navigation system (OLIF-360). The author present a case and surgical technique of simultaneous re-alignment of high-grade spondylolisthesis at L4-5 and insertion of interbody cage by using OLIF-360. An intervertebral cage was inserted at the ideal location after re-alignment of spondylolisthesis with OLIF-360. Postoperative images showed re-aligned vertebra and successful decompression. The specific utilization of OLIF-360 has not been underscored yet.
Lumbar fusion surgery for lumbar degenerative diseases has increased in the past several decades and many techniques for fusion surgery have been introduced. Recently lateral lumbar interbody fusion with minimally invasive technique was introduced and accepted as a useful method for various lumbar degenerative disease. It can produce good correction for sagittal and coronal imbalance with relatively decreased morbidity. The advantage of lateral lumbar interbody fusion is that it can avoid injury to the abdominal large vessels and neural structures which is more common during posterior approaches. However various complications had been reported. Complications related with lateral lumbar interbody fusion include neurologic complications including thigh pain and numbness, vascular complications including arterial injury, cage related complication such as cage subsidence and vertebral body fractures. Therefore special care should be taken to avoid possible complications in lateral lumbar interbody fusion surgery.
Among the complex causes of chronic low back pain, suboptimal injury of ligament in the lumbosacral spine is common. Injured ligaments can become a primary pain source and raise secondary pain with referred pain pattern.
Due to the low blood supply to the ligaments, ligaments are notoriously poor healer. In order to compensate the poor healing of ligament, prolotherapy has been introduced and used for more 60 years. To date, no definite recommendations have not been made based on literature available. However, if conventional treatment modalities have failed in patient with chronic back pain in lumbosacral spine, prolotherapy targeted on ligaments around lumbosacral spine should be considered in appropriate patients.
The foramen of L5-S1 can develop several degenerative diseases such as extraforaminal lumbar disc herniation, foraminal stenosis with disc height collapse, degenerative or spondylolytic spondylolisthesis, and far-out syndrome.
The floating technique in biportal endoscopic spine surgery (BESS) keeps a certain distance between instruments and spinal structures. 1) This key point makes the floating technique different from conventional endoscopic surgery, which uses the Kambin’s safe triangle as a work zone. The floating view can enable the surgeon to see the structures panoramically, under high magnification: consequently, fine discrimination of their margin and safe manipulation of neural structures can be guaranteed. A certain gap between the floating scope and lesion can permit various instruments, generally used in open spine surgery, to be inserted from the sides with fewer limitations. Extraforaminal or foraminal lesions under the lamina can be reached by avoiding the iliac crest, and total facetectomy, which has the potential of iatrogenic instability, is not required to explore the foraminal structures. However, the floating view can be obstructed by small bleeds from laminectomized bone and/or surrounding vessels. This present article describes the technique and provides tips on how to perform BESS with floating technique safely and successfully for various lesions at the L5-S1 foramen.
A 77-year-old female suffering from severe degenerative scoliosis, spinal stenosis and lumbar disc herniation underwent Direct lateral lumbar interbody fusion (DLIF) at L2-4. On the 3rd postoperative day, she complained of severe back pain without any trauma history. Simple radiograph revealed L3 vertebral fracture and cage subsidence.
Pain was subsided after conservative treatment including TLSO and medication. Radiographic union was achieved at fractured vertebra after 3 months. Solid fusion was observed at operated level after 6 months. Patient has visited our clinic without any pain. DLIF is one of novel minimally invasive spine procedures available today. It is designed to maximize benefits and minimize risks of other traditional techniques such as anterior approach and posterior approach. However, there can be some risk of cage subsidence and vertebral fracture after DLIF. Therefore, care should be taken to avoid cage subsidence during the operation.
Objective To compare the pull-out strength of polyaxial general screws and rescue screws when inserted into the lateral mass through cadaveric biomechanical experiment
Materials and Methods Twenty three segments of the human cervical spine (from C3 to C7) were prepared. Two biomechanical studies were progressed. In the first experiment (13 segments), each segment was instrumented with 3.5×12 mm polyaxial screws on both sides. In one side, the inserted screw was removed and then the rescue screw was inserted to the same screw hole. In the second experiment (10 segments), all segments were instrumented with 3.5×12 mm polyaxial screws on both sides and all screws were removed. In one side, removed same screw was reinserted and in the other side, the rescue screw was inserted without change of the screw trajectory. All specimens were fixed to the specially designed frame with the cement. Universal Material Test Machine (Mini Bionix 858) was used to assess the pull-out strength of the screws. All data were compared with non-parametric paired test (Wilcoxon’s signed rank test).
Results There was no crack or fracture around the screw hole. No significant difference was noted between the original screws (not reinserted) and the rescue screws in the first experiment (p=0.753). There is no significant difference between the same screw reinsertion and the conversion to the rescue screw (p=0.646).
Conclusions The overall results of this study showed the conversion to the rescue screw with the same screw trajectory could offer no biomechanical advantage over reinsertion of the same screw. In case of secure screw hole after removal of the screw, the reinsertion of the same screw could be recommended.
Minimally invasive TLIF has been reported to be a useful treatment option for the patients with various degenerative lumbar diseases. Many studies have reported the favorable clinical results of MIS TLIF. However it remains technically demanding, leading to higher complication rates and longer operative times during the early period of the learning curve. It showed some potential complications due to small working space and visual field. In this study, authors tried to find out various possible complications and some tips avoiding these complications through the review of various articles and authors’ clinical experiences. In many studies, the general complication fusion rates of MIS TLIF have been reported to be similar to that of open fusion. The technical difficulty of the procedure, combined with inadequate training, is evident in initial studies of MIS TLIF. A difficult learning curve of MIS TLIF demands that surgeons have sufficient preclinical training, and education is obtained before the application of MIS TLIF in clinical practice.
The minimally invasive technique to correct deformity in scoliosis is not a familiar concept among spine surgeons but is interesting, as this innovative surgery, if it proves successful, will have the advantages of the minimally invasive technique in the final outcomes and will be the future of scoliosis surgery. We operated on 18 adolescent idiopathic scoliosis (AIS) patients using a newly designed technique which utilizes two or three 1-inch midline incisions to insert pedicle screws with a rod, facet fusion and de-rotation maneuver to correct the deformity. Post-operative complications were minimal and the results of the deformity corrections were comparable to the open scoliosis surgery in the follow up. The advantages of minimally invasive surgery observed in all cases include cosmetically fainter scars, reduced blood loss, shorter hospital stay, early mobilization and minimal need of analgesics for pain.
Even though many challenges were faced in executing this procedure, the goal of inventing this novel approach was accomplished. We feel this technique is a good alternative to open surgery in certain curve types of AIS but large scale studies are needed in the future to recommend its routine use.
Purpose Recently, there is concern for spinal sagittal alignment associated with back pain. Nowadays many women wear high heels or high-heeled shoes for their beauty. We study change of spinal sagittal alignment when women are wearing high heels.
Materials and Methods We raised 15 female adult volunteers to accept our study. They do not have past history, operation history and especially back pain. We applied X-rays for anteroposterior and lateral whole spine radiography when women were bare foot (Group I). In addition, we applied each X-rays when women were wearing 5 cm high heels (Group II) and 12 cm high heels (Group III). We estimate the spinal sagittal alignment distinguishing pelvic index from spinal index. We use ANOVA test of SPSS v18.0 statistically.
Results The average age of women was 29.3(23-41) years old, and mean BMI (Body Mass Index) was 18.7(16.2-24.5) kg/m 2 . When volunteers were bare foot, the average pelvic incidence (PI) was 49.3 degree, pelvic tilt (PT) was 10.8 degree, and sacral slope (SS) was 37.9 degree. The each average of lumbar lordosis (LL), thoracic kyphosis (TK), T12 slope, and sagittal vertical line on middle point of C7 (C7 SVA) and T12 (T12 SVA) was 55.5 degree, 28.5 degree, 19.3 degree, -1.2 cm, and -3.8 cm. When women were wearing 5 Cm high heels, the average was each 49.2 degree, 18.9 degree, 35.4 degree, 54.9 degree, 29.1 degree, 20.5 degree, -2.0 cm, -2.5 cm. When women were wearing 12 cm high heels, the average was each 49.9 degree, 18.2 degree, 31.2 degree, 52.6 degree, 30.8 degree, 22.8 degree, -4.1 Cm, -4.1 cm. Compared with each group, sacral slope (SS) and vertical line on middle point of C7 was statistically significant in group III (p<0.05). There was no statistically correlation between group I and group II.
Conclusion Spinal sagittal alignment can be changed if adult women wear high heels excessively. For maintaining of normal spinal sagittal alignment, We conclude adult women wearing high heels for a long time pay attention to change of their spinal sagittal alignment.
Purpose Pull-out of pedicle screw in posterior pedicle fixation for thoracic and lumbar burst fractures causes delayed rehabilitation, persistant pain, and imblance of sagittal plane. In this study we try to analyse the factors that cause the pull-out of pedicle screw.
Materials and Methods From March 01, 2006 to December 31, 2009, we assorted into two group; Group I for pullout pedicle, Group II for control. Plane lateral x-ray view film of thoracolumbar spine was taken on preoperation, postoperation, the first time when screw was pulled out and last follow up. we measure inserted angle for the upper endplate of screw, convergency angle and change of body height loss and kyphotic angle. We analysed corelation between these measuring values and pedicle screw pull-out by Mann-Whitney test and T-test.
Results Pull-out of pedicle screw was found at mean 5weeks among nine cases. For inserted pedicle screws, which place in upper and lower vertebral body of fractured one, Value of inserted angle for upper end plate and convergency angle was found non-significant(p>0.05, Mann-Whitney test). Restoration of height loss and kyphotic angle of fractured vertebral body was statically significant(p<0.05, T-test).
Conclusion In posterior pedicle fixation for thoracic and lumbar burst fractures, sufficient restoration of height loss and kyphotic angle is important factor for prevention of screw pull-out than inserted angle for upper end plate and convergency angle at a short period of time. Therefore we think that sufficient anterior fixation of vertebral body and restoration of kyphotic angle have a decisive effect on prognosis of patients.
Purpose To analyze the risk of a fall in patients with cervical spondylotic myelopathy (CSM) and its clinical significance.
Materials and methods 40 patients with CSM who visited to our hospital From May 2014 to April 2015 were enrolled in this study. After confirmation of CSM based on MRI and Physical examination, patients were divided into three groups according to m-JOA score (Group A; severe; score <8, Group B; moderate; score 8-12, Group C; mild score >13). All patients enrolled in this study performed 4 functional assessment test including Alternative-Step Test (AST), Six-MeterWalk Test (SMT), Sit-to-Stand test (STS), and Timed Up and Go test (TUGT) to assess the risk of a falls (ROF).
Results There were statistical significance between m-JOA score and ROF except for SMT. Average time (seconds) for STST was 26.12±5.60, 20.99±5.92 and 15.37±3.41 in group A, B, C, respectively (p=0.001), Although average time(s) for AST was 16.81±3.83, 14.39±4.05 and 12.37±3.95 in group A, B, C with no statistical significance (p=0.106), there was a significance between the value of Group A and C (p=0.047). Average time(s) for TUGT was 31.86±17.05, 15.09±4.59,18.04±9.32 in group A, B, C, respectively, showed statistical significance (p=0.000).
Conclusion According to its severity of myelopathy, it took more time to carry out each ROF assessment tests. Among 4 functional assessment tests of ROF, STST showed the most highest correlation with mJOA socre. Careful attention of ROF will be needed in patients with myelopathy.
Background Cervical kyphosis is frequently observed in the patients without axial neck pain and sigmoid curvatures are parts of the variety of cervical kyphosis.
Purpose This study was designed to investigate the characteristics of the static and dynamic alignment of the cervical spine with sigmoid configurations.
Methods Figty patients without changes of the cervical curvatures after subsidence of axial neck pain were enrolled in this study. Based on the alignment of cervical spine on lateral radiographs, cervical alignments were classified:
kyphotic (K), kypho-lordotic (KL), lordo-kyphotic (LK), and Lordotic (L) group. The sagittal alignment angles and each segmental angle were measured using the Harrison method on neutral, flexion, and extension-lateral radiographs.
Results The mean ratio of segmental ROM to C2-7 ROM revealed a similar pattern across the cervical levels without statistical difference between the groups. In the KL and LK group, the linear graphs for the mean ratio of segmental angles to C2-7 angles in flexion and extension showed a mirror image with respect to the C4-5 level. The lordotic components of both curves demonstrated larger ratio of segmental angles in flexion than the kyphotic components.
The kyphotic components of both curves demonstrated larger ratio of segmental angles in extension than the lordotic components.
Conclusions The lordotic and kyphotic components regardless of the type of sigmoid curvatures seem to adhere to constant dynamic behavior during flexion and extension. Therefore, the KL and LK cervical alignments may have the opposite dynamic behaviors in the high and low cervical levels.
Purpose To evaluate the method of inserting cortical bone trajectory pedicle screws (cortical screws) and potential complications when performing lumbar fusion.
Methods Lumbar fusion with cortical screw fixation in the hard cortical bone of the pars interarticularis of vertebrae was introduced to replace conventional pedicle screws. We review the literature on the biomechanics of cortical screw insertion and on the clinical outcomes.
Results In vitro biomechanical testing has shown that cortical screws have greater pullout strength than traditional pedicle screws due to the strong bone–screw interface in cortical bone. Cortical screws have the advantages of requiring minimal muscle dissection and shortening the surgery. However, early screw loosening and loss of reduction have been reported.
Conclusions When inserting cortical screws, the entry point and trajectory of the screws are important and a meticulous surgical technique is needed to prevent potential screw-related complications.
Purpose Total en bloc spondylectomy (TES) is one of curative surgical methods used for solitary spinal tumors, if indicated. However, TES is a complex technique and prudent preparation is mandatory. However, elective TES is not always possible for patients with neurological and mechanical spinal instability. In such situations, percutaneous pedicle screw fixation, with the purpose of stabilizing the spine and gaining time before TES, may be used.
Methods The first patient was a 29-year-old female who visited the emergency room (ER) due to progressive paraparesis (motor grade III/V) and back pain. Magnetic resonance imaging (MRI) showed compression of the spinal cord by a tumor and a collapsed L1 body. The second patient was a 23-year-old female who came to the ER with severe back pain. MRI revealed compression of the spinal cord by a collapsed T11 vertebral body and a tumor.
In both cases, neurological and mechanical instabilities were caused by a primary vertebral tumor. For both patients, TES was an optimal surgical technique, but TES was not possible on an emergency basis.
Results In both patients, percutaneous pedicle screw fixation, distraction, and biopsy were performed on an emergency basis. Subsequently, weakness and/or pain improved in both patients. Elective TES operations were successfully performed 3 weeks or 1 month later.
Conclusions If TES is indicated, but preparation time is insufficient, tentative spinal stabilization with a percutaneous technique may be utilized before TES. However, considering the need for additional surgery, skin incision, and cost, this surgical strategy should be selectively applied.
Purpose To compare the difference of cervical alignment between cervical lateral radiograph and whole-spine lateral radiograph by the effects of radiographic position and to assess the effect of the shoulder flexed position to cervical lordotic curvature and head position.
Materials and Methods We retrospectively evaluated 43 asymptomatic adult patients who were taken horizontal gazing standing cervical and whole-spine lateral radiograph simultaneously from Sep. 2008 to Dec. 2009. Cervical lateral radiograph was taken with the arms extended and hand gently clasped on both side and whole-spine lateral radiograph was taken in the position that subject were relaxed standing with fists-on-clavicles position. Cervical sagittal alignment were analyzed the following parameters. (1) Gore angle (GA, C2-7 angle); (2) Cobb angle (CA, C2-7 angle); (3) translation distance (TD, distance of C2 compared with vertical line through the posterior-inferior body of C7); (4) McGregor angle (MA, angle between McGregor line and horizontal line).
Results The mean of GA and CA in cervical radiograph were -12.64° and -9.96°, whereas -7.12° and -4.98° in wholespine radiograph. The mean TD and MA were in cervical radiograph were 16.95mm and 7.15°, whereas, 14.97mm and 6.54° respectively in whole-spine radiograph.
Conclusion Our study showed the significant differences of cervical alignment and head position between standing cervical lateral and whole-spine lateral radiograph. The radiographic posture of whole-spine lateral radiograph with horizontal gazing and fists-on-clavicles position make cervical alignment and head position less lordotic and posterior translation compared to cervical radiograph.
We reviewed literatures relating to minimally invasive lateral lumbar interbody fusion for the treatment of adult degenerative spinal deformity. Most of literatures were retrospective case series with a small numbers of patients.
A prospective multicenter study was published in two separate papers. This procedure was effective in treating the coronal deformity. On the other hand, restoring the sagittal plane remains an issue. Pseudarthrosis was problematic, especially in the cases without use of the human recombinant bone morphogenetic protein-2 (rhBMP-2) and bilateral pedicle screw fixation. Temporary sensory deficits and transient leg weakness was the most common complication after lateral lumbar interbody fusion. Careful patient selection is important for the application of lateral minimally invasive techniques for adult degenerative scoliosis.
Intraoperative blood loss volume increases due to soft tissue injury or excessive traction generated by extensive approach including posterior fusion or posterior lumbar interbody fusion, leading to the occurrence of complication and delay in postoperative recovery, On the other hand, MI-TLIF minimizes injuries in soft tissue and surrounding muscle by approaching between multifidus muscles and longissimus dorsi after separating them, and reaching intervertebral disc from lateral vertebral foramen. The advantages of this surgical procedure are minimization of muscle or soft tissue injuries incurred by lateral approach, reduction of surgically related muscle damage, and decrease of postoperative blood loss. However, The size of cages are limited by transforaminal approach in MI-TLIF, eventually it could be difficult to maintain the correction of deformity(disc height, segmental and lumbar lordosis).
Recently, DLIF(Direct lateral interbody fusion) is developed to improve the disadvantages of TLIF. DLIF allows to insert larger cage than TLIF, as a result larger cage have a advantage to maintain correction of disc height and lordosis because it can support both apophyseal rings of endplates.
However, Transpsoas approach is essential for DLIF, so we need to understand the anatomy lumbosacral plexus in psoas, because nerve injury during the transpsoas approach is the most common and potentially the most devastating complication of the DLIF procedure. And many authors reported that various frequency of nerve injury according to surgeon’s skill. Therefore, surgeon’s skill and accurate understanding about the procedure are important factors to prevent the complications of DLIF.
Purpose The purpose of the study was to investigate the effect of obesity on the accuracy of percutaneous pedicle screw placement.
Materials and Methods We performed a retrospective analysis on the first 89 patients undergoing minimally invasive lumbar fusion with percutaneous pedicle screw placements for the treatment of degenerative lumbar spinal disorder.
Based on patient’s body mass index (BMI), patients were divided into 3 groups: group 1 – normal weight (BMI<25, 38 patients, 157 screws); group 2 – overweight (25≤BMI<30, 29 patients, 124 screws); group 3 – obese (BMI≥30, 22 patients, 89 screws). Using postoperative computed tomography (CT) scans, the position of placed screws to the pedicle or anterior body perforation was evaluated using the following grading method: Grade A, completely in the range without pedicle cortex violation; Grade B, pedicle wall violation<2 mm; Grade C, pedicle wall violation 2 to 4 mm; and Grade D, pedicle wall violation>4 mm.
Results Among the 370 pedicle screws, 308 screws (83%) were perfectly placed within the pedicle. Among the 62 misplaced screws, 45 screws were grade B pedicle breaches (73%, 45/62), and 45 screws were misplaced in lateral direction (73%, 45/62). 36 screws (10%) perforated the anterior vertebral cortex. Twenty eight screws were misplaced in overweight group, 12 screws in obese group, and 22 screws in normal weight group. With the number of screws available, subgroup analysis did not reveal a significant difference in the grade (p=0.10) or the direction (p=0.97) of pedicle breaches among groups.
Conclusion Our data suggest that obesity does not affect the accuracy of percutaneous pedicle screw placement. We do not hesitate or deny the surgery because of patient’s heavy body habitus, which seems to be a apparent benefit of minimally invasive spinal surgery.
Objective Peridural fibrosis may cause failed back syndrome and the presence of fibrosis renders reoperations risky.
Therefore, preventing the adhesion of scar tissue to the dura and nerve root is one of the issues in spinal surgery.
Thus, the purpose of this study is to evaluate and compare the efficacy and the safety between two anti-adhesive agents, BNCH-202 (Korea BNC Inc, Daegu, Korea) and Guardix-SOL (Hanmi, Seoul, Korea).
Methods Sixty eight patients were enrolled in this study. To evaluate and compare the efficacy in preventing epidural adhesion formation and the safety in human laminotomy models, the two barriers tested were either BNCH-202 or Guardix-SOL (gel/film combination). Clinical evaluation was performed at 0, 6 and 12 weeks to assess pain and functional outcome. The patients were also assessed radiographically with postoperative magnetic resonance imaging (MRI) to evaluate the presence of perinueral scar and adhesion.
Results There was no statistically significant difference between two biologic barriers in terms of the safety issue, clinical and radiological efficacy. There were no significant differences between the BNCH-202 group and the control group on the preoperative ODI and VAS scores. In general, the ODI and VAS scores decreased in both groups at all the time points. At the 6 week and 12 week time point, the VAS scores for back pain/ leg pain and the ODI scores in both groups were lower than the preoperative score in each group (P<0.01). And at the 12-week time point, the peridural scar scores were assessed in both groups. The mean value of the peridural scar score in BNCH-202 group was not inferior to the mean value of that in Guardix-SOL group.
Conclusion The results demonstrated that BNCH-202 gel is as effective as Guardix-SOL in reducing posterior dural adhesions in the spine with no apparent safety issues. It can improve patients’ postoperative clinical outcome.
Summary of Background Data Recently, minimal invasive spine surgery has been used and spine surgeons are prone to the radiation exposures.
Objectives: To determine the radiologic hazard to the spine surgeon.
Methods We searched the PUBMED, MEDLINE with Mesh term from MIS, radiation exposure.
Results We reviewed the radiation exposure in different disease and surgery. There exist significant dose of radiation exposures in MIS Discectomy, MIS or open pedicle screw fixation, and kyphoplasty.
Conclusion Surgeons should aware of the radiation exposure of the spine surgery and should do efforts on minimize it.
Introduction Recently, minimally invasive lateral approach for the lumbar spine is revived and getting popularity under the name of XLIF or DLIF by modification of mini-open method using sequential tubular dilator and special expandable retractor system.
Purpose s: The purposes of this study were to introduce the mini-open lateral approach for the anterior lumbar interbody fusion (ALIF), and to investigate the advantages, technical pitfalls and complications & to provide basic knowledge on XLIF or DLIF
Materials and Methods Seventy-four patients who underwent surgery by the mini-open lateral approach from September 2000 to April 2008 with various disease entities were included. Blood loss, operation time, incision size, postoperative time to mobilization, length of hospital stay, technical problems and complications were analyzed.
Results With this approach, we can reach form T12 to L5 subdiaphragmatically. The blood loss and operation time of patients who underwent simple ALIF were 61.2 ml and 86 minutes for one level, 107 ml and 106 minutes for two levels, 250 ml and 142.8 minutes for three levels, and 400 ml and 190 minutes for four levels of fusion, respectively.
The incision sizes were on average 4.5cm for one level, 6.3 cm for two levels, 8.5 cm for three levels and 10.0 cm for four levels of fusion. The complications were retroperitoneal hematoma in two cases, pneumonia in one case and transient lumbosacral plexus palsy in three cases.
Conclusion The mini-open lateral approach is simpler & safer than XLIF or DLIF with very short learning curve. Trial of mini-open lateral approach would be helpful before trial of XLIF or DLIF. However, special attention is required to complications such as transient lumbosacral plexus palsy.
A 45 year-old male was brought to our hospital with severe back pain and motor, sensory impairment in both lower extremities. He had no underlying diseases including coagulapathy. Motor weakness below both hip joint and decreased sensory below T12 dermatome, voiding dysfunction were examined. The MRI showed a spinal subdural hematoma at the thoracolumbar region, which was extremely rare. Medical treatment was applied without surgical interventions. After two weeks, motor weakness, sensory impairment, and voiding dysfunction were improved. And he returned to his daily activities. We present this case and literature reviews because traumatic spinal subdural hematoma is an extremely rare disease and the condition was treated successfully in conservative manner.
Discectomy or fusion have been a gold standard of the treatment for discogenic back pain. Since mid 1950s, spine surgeons have introduced the concept of arthroplasty for the management of low back pain. The current technologies are total disc replacement (TDR), posterior dynamic stabilization (PDS), interspinous process. Although many studies have reported their efficacy and safety, there are still lacking high-quality evidence. It is also not proven that these technologies are superior to spinal fusion in preventing the adjacent segment disease.
Second generation TDR is newly developed technology. The current TDR could allow the motion of flexionextension and lateral bending, but it did not have the capacity to bear the axial compressive force. Second generation TDR placed the shock-absorption materials that can endure the compressive force. The current TDR was performed through the anterior approach, which is invasive and necessitates the removal of anterior longitudinal ligament. To
overcome these disadvantages, TDR through lateral approach was developed. Various type of nucleus replacement technologies have been introduced with theoretical advantages over TDR such as less invasiveness, stable segmental motion and preservation of disc height. However, some of them had critical problems such as the migration and subsidence of implanted prosthesis. Total facet replacement arthroplasty was developed to overcome both the
adjacent segment disease after fusion and the instability after posterior decompression. Because most of reports about total facet replacement arthroplasty are based on the results from the animal or cadaveric study, the long-term human trial is required.
New technologies regarding motion preservation spinal surgery have been introduced, shifting paradigm in spinal care. Even though various attempts have been made in the field of spine surgery, the fact is that all of these attempts do not succeed due to paucity of better clinical outcomes. Thus, well designed long-term studies are required to prove their safety and efficacy, showing “superiority”, not just “no inferiority” to the traditional treatments.

 First
First Prev
Prev

