Purpose To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
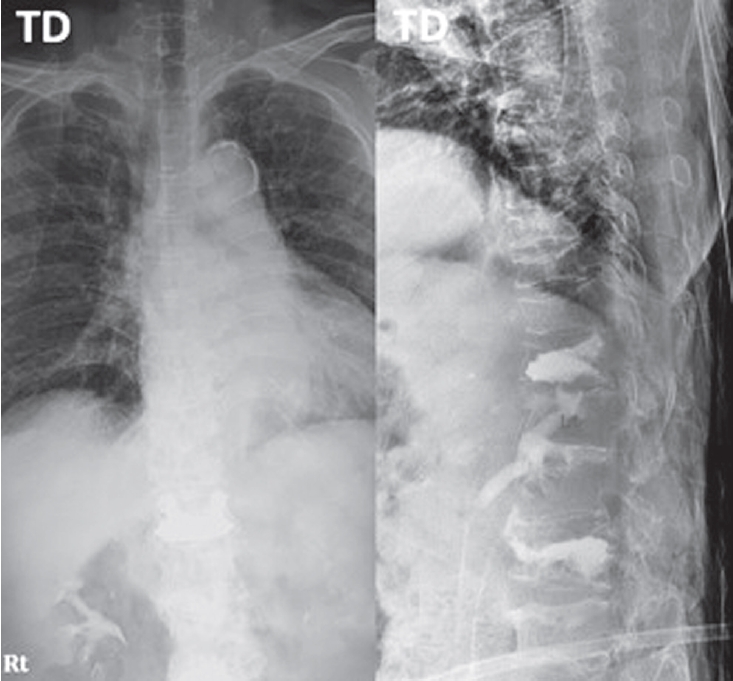
Methods An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
Purpose To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
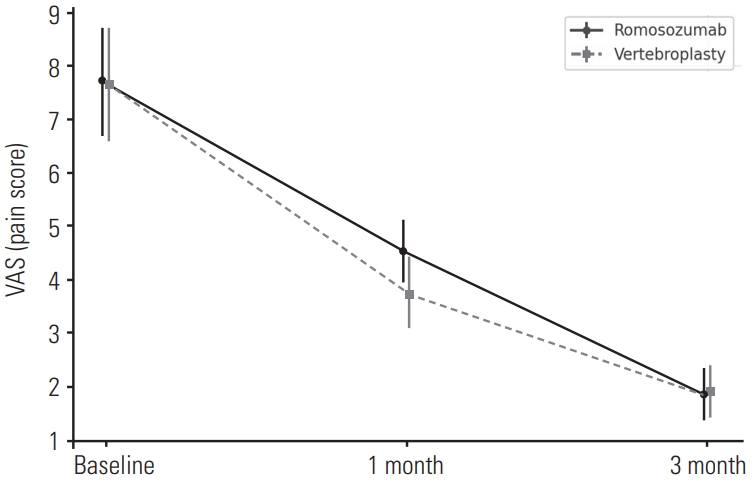
Material and Methods: This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.
Vertebral compression fracture is one of the most common osteoporotic fractures along with hip fractures. In some patients, pain was improved through conservative treatment including pharmaceuticals, bracing and physiotherapy. But it has been reported that conservative therapy is insufficient in many patients with vertebral compression fracture. Accordingly, interest in vertebroplasty has increased and many studies have been reported that vertebroplasty have therapeutic effects in acute vertebral compression fracture. On the other hand, some studies have been reported that the effect of vertebroplasty was not significant. So whether vertebroplasty is useful or not is still controversial. Therefore, in this review article, we will review open-label randomized controlled trials and blinded randomized controlled trials that provide high-level evidence and provide an opinion on which patients it is appropriate to perform vertebroplasty.
Introduction We describe the complications that can occur after percutaneous vertebroplasty using bone cement for osteoporosis vertebral compression fracture.
Main subject: The most common complication of percutaneous vertebroplasty is the leakage of bone cement.
Leakage of bone cement has been reported variously and could leak into the spinal or neural foramen, adjacent intervertebral disc and soft tissues around the spine, and venous systems. The most serious complications are neurologic symptoms due to spinal cord and nerve root compression and complications associated with death due to heart and pulmonary embolism. In addition, recompression fracture or adjacent vertebral compression fracture might occur and various treatment methods have been proposed.
Conclusion The complications that can occur after percutaneous vertebroplasty have been reported variously, including neurologic deficits due to the leakage of bone cement and lung and heart embolism. In addition, there is a possibility of recompression fracture or adjacent compression fracture. Therefore, you should be careful about percutaneous vertebroplasty. Finally, patients with many risk factors regarding complications of vertebroplasty would need close observation and follow-up.
Purpose To evaluate long term efficacy of percutaneous balloon kyphoplasty for osteoporotic compressive vertebral fracture.
Materials and Methods Percutaneous balloon kyphoplasty was performed to 52 vertebral bodies, for 42 patients with compression fracture from March 2003 to October 2007. During observation, 32 patients (39 vertebral bodies) were followed over 5 years except 8 patients (19.0%) who have expired. Pre operational, post operational and final observational radiologic evaluation (vertebral height, compression ratio, kyphotic angle) and clinic evaluation(VAS score) were checked. And correlation with bone cement leakage, fracture of adjacent vertebral body, gender, age, bone mineral density and medication was analyzed.
Result Average age was 71.3 years old and average observation period was 74.3 months. Average interval from injury to operation was 24.1 days. Vertebral compression ratio recovered 29.7% to 17.4% (12.3%), kyphotic angle improved 11.6 degree to 9.0 degree (2.6 degree) and there was no significant change until final observation. VAS score got better 7.60 to 3.57 (4.03) after operation. Bone cement leakage occurred in 5 cases (12.8%) and fracture of adjacent vertebral body occurred in 10 cases (25.6%), there was no correlation between two groups (p=1.000). Fracture of adjacent vertebral body showed meaningful correlation with bone mineral density only.
Conclusion Percutaneous balloon kyphoplasty relieve the pain after compression fracture of vertebral body and is safe and efficient procedure to correct sagittal deformity. After 5 year follow up, the effect of procedure was maintained clinically. Bone cement leakage did not increase risk of fracture of adjacent vertebral body which occurred frequently in low bone mineral density.
Purpose Osteoporosis is an age-related systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone contents, with a consequent increase in bone fragility. In severe osteoporosis progressive collapse of multiple vertebrae is and unsolved problem. Medical treatment appears to be too slow to prevent the course. Recently, there are some reports on the results of the percutaneous vertebroplasty (VP) in treating the multi-level osteoporotic vertebral compression fractures (VCFs). we reviewed painful multi-level osteoporotic VCFs treated by percutaneous VP and assess the efficacy and safety of multiple percutaneous cement VP in the treatment of multi-level osteoporotic VCFs.
Materials and Methods From January 2008 to August 2010, the clinical cases and radiographic records were reviewed retrospectively for 28 patients treated for the multi-level painful osteoporotic VCFs by percutaneous cement VP.
Initially radiography and MRI of the spine were performed. Spine radiographs were repeated at post-operation, 1,3 months and final follow-up. The patient’s outcomes of demographic, clinical, radiologic and procedural data were analyzed and assessed using self-report and physiological measures. A t-test was used for means of VAS, anterior vertebral height and kyphotic angle. Statistical analysis was performed with the SPSS(Version 15.0.1, Chicago, Illinois). The p-values of < 0.001 were deemed significant.
Results The back pain recorded using the VAS improved significantly in all cases, from 7.7±1.0(6-10), points preoperatively to 2.0±0.7(1-3) points postoperatively (p<0.001) and then 2.8±0.8(1-4) points at the follow-up (p<0.001).
The anterior heights increased from 17.40±4.98 to 21.02±5.36 after VP procedures (p<0.001) and finally 19.49±5.28 (p<0.001). The kyphotic angle was 12.58º preoperatively and improved to 4.39º postoperatively, but kyphotic deformities became worse in 12.80º.
Conclusion The vertebroplasty for patients with multiple osteoporotic vertebral compression fractures may improve pain and can be effective for preventing adjacent fractures, restoration of vertebral height and maintenance of sagittal alignment. Patients with multiple osteoporotic compression fractures have many comorbidity, the surgeon should be conscious to all procedure.

 First
First Prev
Prev

