Romosozumab Following Long-Term Bisphosphonate Use for Severe Osteoporotic Vertebral Collapse (Vertebra Plana): Potential Facilitation of Vertebral Fracture Healing
Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea
Corresponding author: Jae-Won Shin, M.D., Ph.D. Department of Orthopedic Surgery, Yonsei University College of Medicine, 50-1, Yonsei-ro Seodaemun-gu, Seoul, Korea TEL: +82-2-2228-2181, FAX: +82-2-363-1139 E-mail: jaewuni@yuhs.ac
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
Methods
An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results
During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions
Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
장기간 비스포스포네이트 치료를 받아온 고령의 중증 골다공증 환자에서 로모소주맙으로 치료를 전환한 후, 척추 골절 치유 및 임상적 경과를 평가하고 전환 치료의 임상적 시사점을 제시하고자 한다.
대상 및 방법
골다공증성 골절 병력이 있고 장기간 정주 비스포스포네이트 치료를 받아온 85세 여성 환자가 급성 요추 제2번 압박 골절로 내원하였다. 보존적 치료로 체간 석고 고정을 시행하였으며, 골형성 촉진 치료가 필요하다고 판단하여 로모소주맙으로 치료를 전환하였다. 흉요추부 단순 방사선 촬영은 수상 시점 및 수상 후 1, 3, 7, 12, 18개월에 시행하였고, 컴퓨터단층촬영은 초기 및 수상 후 7개월, 12개월에 시행하여 골절 치유 과정을 평가하였다. 골밀도 검사는 수상 후 18개월 시점부터 시행하였으며 이후 매년 추적 관찰하였다. 통증 및 보행 능력에 대한 기능적 평가는 총 30개월간 추적 관찰하였다.
결과
로모소주맙 치료 기간 동안 요추 제2번의 심한 척추체 평면형(vertebral plana) 골다공증성 압박골절에서 골내 골충전의 진행과 함께 소주골 연속성이 점진적으로 회복되는 방사선학적 호전을 보였으며, 추가적인 척추체 높이 소실은 관찰되지 않았다. 추적 컴퓨터단층촬영에서 이전에 공동화되었던 척추체의 골성 치유가 확인되어 단순 안정화가 아닌 구조적 회복이 이루어졌음을 시사하였다. 임상적으로 통증 및 보행 능력은 점진적으로 호전되었다. 로모소주맙 6개월 치료 종료 후 데노수맙으로 유지 치료를 전환하였으며, 요추 골밀도 T-score는 -1.7에서 -0.9로 개선되었고 대퇴부 골밀도 또한 증가하였다. 추적 관찰 기간 동안 추가적인 취약성 골절은 발생하지 않았다.
결론
장기간 비스포스포네이트 치료 후 로모소주맙으로 치료를 전환한 결과, 고령의 중증 골다공증 환자에서 골밀도 개선과 함께 척추체 골내 골충전 및 구조적 회복이 관찰되었고 추가적인 붕괴 없이 안정적인 임상 경과를 보였다. 로모소주맙은 중증 골다공증 환자에서 선택적으로 고려될 수 있는 골형성 촉진 치료 옵션이 될 수 있으며, 이후 데노수맙 유지 치료는 장기적인 골격 보호에 기여할 수 있을 것으로 판단된다.
Osteoporotic vertebral compression fractures (OVCFs) are a major health burden in the elderly population, frequently resulting from systemic skeletal fragility associated with osteoporosis.1) Severe forms of OVCF, including vertebra plana–type collapse, can lead not only to persistent pain and disability but also to progressive kyphotic deformity, impaired pulmonary function, and, in some cases, catastrophic neurologic compromise.2) These fractures are strongly associated with underlying severe osteoporosis, defined as a BMD T-score ≤ –3.0 or the presence of one or more fragility vertebral fractures, placing patients at substantial risk for subsequent fractures and structural deterioration.3,4)
Pharmacologic treatment for osteoporosis is broadly categorized into antiresorptive and anabolic agents. Bisphosphonates remain a widely used first-line antiresorptive therapy due to their proven fracture-prevention efficacy.5,6) However, long-term bisphosphonate exposure may suppress bone turnover to the extent that microdamage repair and fracture healing become impaired, potentially exacerbating structural instability in patients with severe vertebral collapse.7) When patients on antiresorptive therapy sustain new fragility fractures or continue to demonstrate skeletal deterioration, guidelines typically recommend initiating anabolic treatment, most commonly teriparatide.3,8)
Teriparatide has demonstrated robust anabolic effects and potential benefits in fracture healing, yet its use is limited by daily injections, contraindications in certain metabolic conditions, and an early transitional decline in BMD when switching from bisphosphonates.9) This early phase is clinically significant because rapid bone recovery is essential to prevent recurrent vertebral collapse after an acute fracture. Thus, alternative anabolic options may be necessary for patients who require prompt skeletal reinforcement following long-term antiresorptive therapy.
Romosozumab, a monoclonal antibody that increases bone formation while simultaneously reducing bone resorption, has emerged as another treatment option in severe osteoporosis.10) Although its fracture-prevention efficacy and rapid BMD gains are well established, romosozumab has not been proven to enhance fracture healing, and current evidence is limited mainly to preclinical animal models. Nevertheless, in cases of severe vertebral collapse where early anabolic response is desired and teriparatide use is impractical, romosozumab may offer a reasonable therapeutic alternative. Here, we report a case of severe osteoporosis with multiple vertebral compression fractures in a patient receiving long-term bisphosphonate therapy who sustained a new vertebral fragility fracture and was subsequently switched to romosozumab. We describe the corresponding clinical and radiologic outcomes, including notable vertebral bone fill-in during follow-up.
Case
An 85-year-old woman presented with acute back pain after falling on an escalator. Neurological examination showed no motor or sensory deficits and no bowel or bladder dysfunction. Her medical history included vertebroplasty for T12 and L3 compression fractures and a right subtrochanteric femoral fracture treated with plate fixation. After the femoral fracture surgery, she had received intravenous bisphosphonate therapy at 3-month intervals for two years. Initial radiographs revealed multiple chronic vertebral compression fractures, and computed tomography identified a new L2 compression fracture (Fig. 1).
Baseline BMD confirmed severe osteoporosis, showing a T-score of approximately –3.0. Given her advanced age, compromised bone quality, and multilevel vertebral collapse, conservative management was selected. A body cast was applied for two months, and romosozumab was initiated as an anabolic option following prior bisphosphonate therapy.
At the two-month follow-up, radiographs demonstrated no further collapse of the L2 vertebra, and her body cast was exchanged for a thoracolumbosacral orthosis (TLSO). Back pain progressively improved. By three months, radiographs showed early signs of fracture consolidation accompanied by improved ambulation and increased walking distance (Fig. 2).
At six months, she was able to ambulate with a walker. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab for long-term maintenance. One-year follow-up CT demonstrated complete consolidation of the L2 fracture with substantial intravertebral bone fill-in (Fig. 3).
At 18 months, BMD had improved from –1.7 to –0.9 in the lumbar spine and –3.5 in the femur. By 30 months, femoral BMD further improved to –3.0, and no additional fragility fractures occurred during the follow-up period.
Discussion
This case demonstrates the clinical and radiologic course of an elderly patient with severe osteoporosis and vertebra plana–type vertebral collapse who sustained a new fragility fracture despite long-term bisphosphonate therapy. After the injury, conservative treatment combined with a transition to romosozumab resulted in progressive intravertebral bone fill-in and complete consolidation of the L2 fracture without further collapse. Functional improvements paralleled radiographic recovery, and subsequent maintenance therapy with denosumab supported continued skeletal stabilization throughout follow-up.
The choice of anabolic therapy is particularly important in patients previously treated with bisphosphonates, as the metabolic environment created by long-term anti-resorptive therapy may influence early treatment responses.6) Several clinical studies have shown that switching from bisphosphonates to teriparatide can lead to an initial increase in bone resorption and a transient decrease in BMD during the early phase of therapy, a period during which patients remain at increased risk for additional fractures.8) This early imbalance between bone formation and resorption may delay early structural recovery and represents a meaningful limitation when teriparatide is used immediately after a new vertebral fracture.8)
Romosozumab offers a mechanistically distinct anabolic option, characterized by rapid increases in bone mass and simultaneous suppression of bone resorption. Preclinical studies in animal models have suggested that sclerostin inhibition may enhance callus formation and improve biomechanical strength, although such findings have not been confirmed in human fracture-healing trials.11,12) Thus, romosozumab cannot be considered a fracture-healing agent. Nonetheless, the dramatic consolidation and intravertebral bone fill-in observed in this case suggest that romosozumab may help stabilize skeletal metabolism following a fragility fracture, particularly in patients who require early anabolic support after long-term bisphosphonate therapy.9)
This report has several limitations. As a single case, causality between romosozumab and fracture consolidation cannot be established, and the observed radiologic improvement may reflect the natural healing process or the mechanical support provided by bracing. Bone turnover markers were not measured, limiting insight into the metabolic response to therapy. Additionally, romosozumab was used in a patient without cardiovascular risk factors, and its generalizability to broader populations requires caution. Further clinical studies are needed to clarify the optimal sequence of anabolic and anti-resorptive agents after longterm bisphosphonate use and to determine whether romosozumab provides meaningful advantages during the early post-fracture period.
Conclusions
Switching from long-term bisphosphonate therapy to romosozumab was followed by fracture consolidation, preserved vertebral height, and improved BMD in this elderly patient with severe osteoporosis. Although not proven to enhance fracture healing, romosozumab may be a reasonable option when early metabolic stabilization is needed or when teriparatide is unsuitable.
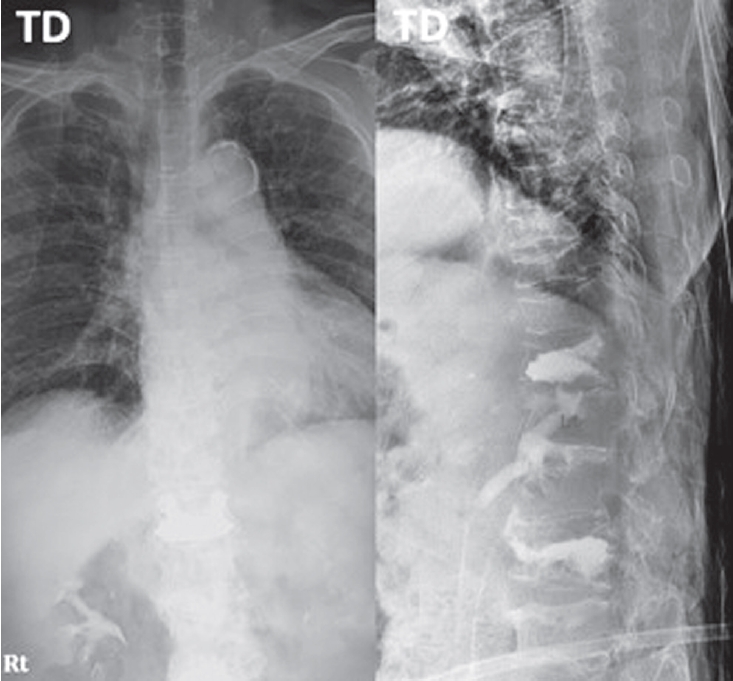
Fig. 1.
Initial lumbar spine anteroposterior and lateral radiographs demonstrating an acute L2 compression fracture and multiple chronic compression fractures and prior vertebroplasty at T12, L3.
Fig. 2.
Serial follow-up radiographs showing progressive healing of the L2 compression fracture with increasing vertebral body consolidation.
Fig. 3.
Follow-up computed tomography demonstrating interval consolidation of L2 vertebral fracture.
References
1. Khoo B, Gonzalvo A, Kweh BTS. Spinal orthoses in osteoporotic vertebral fractures of the elderly. J Spine Surg 2023;9(3):224-8.
2. Suzuki N, Ogikubo O, Hansson T. Previous vertebral compression fractures add to the deterioration of disability and quality of life after an acute compression fracture. Eur Spine J 2010;19(4):567-74.
3. Camacho PM, Petak SM, Binkley N, et al. American Association of Clinical Endocrinologists and American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis— 2016. Endocr Pract 2016;22(Suppl 4):S1-S42.
4. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 2014;25(10):2359-81.
5. Qaseem A, Forciea MA, McLean RM, et al. Treatment of low bone density or osteoporosis to prevent fractures: A clinical practice guideline update from the American College of Physicians. Ann Intern Med 2017;166(11):818-39.
6. Watts NB, Adler RA, Bilezikian JP, et al. Osteoporosis in men: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2012;97(6):1802-22.
7. Komatsubara S, Mori S, Mashiba T, et al. Suppressed bone turnover by long-term bisphosphonate treatment accumulates microdamage but maintains intrinsic material properties in cortical bone of dog rib. J Bone Miner Res 2004;19(6):999-1005.
8. Curtis EM, Moon RJ, Harvey NC, Cooper C. The impact of switching osteoporosis therapies: current evidence and clinical implications. Aging Clin Exp Res 2022;34(4):695-714.
Romosozumab Following Long-Term Bisphosphonate Use for Severe Osteoporotic Vertebral Collapse (Vertebra Plana): Potential Facilitation of Vertebral Fracture Healing
Fig. 1. Initial lumbar spine anteroposterior and lateral radiographs demonstrating an acute L2 compression fracture and multiple chronic compression fractures and prior vertebroplasty at T12, L3.
Fig. 2. Serial follow-up radiographs showing progressive healing of the L2 compression fracture with increasing vertebral body consolidation.
Romosozumab Following Long-Term Bisphosphonate Use for Severe Osteoporotic Vertebral Collapse (Vertebra Plana): Potential Facilitation of Vertebral Fracture Healing