Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Corresponding author: Jin-Sung Park, M.D., Ph.D. Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea TEL: +82-2-3410-1583, FAX: +82-2-3410-0061, E-mail: jinsungosspine@gmail.com, jinsungosspine.park@samsung.com
*These authors contributed equally to this work.
• Received: May 15, 2026 • Revised: June 5, 2026 • Accepted: June 9, 2026
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dysplastic spondylolisthesis is a developmental subtype characterized by congenital lumbosacral abnormalities and progressive instability. Primary presentation with cauda equina syndrome (CES) has rarely been reported. We report a rare case of CES associated with high-grade dysplastic spondylolisthesis in a patient with concurrent giant ovarian teratomas, which contributed to delayed diagnosis and treatment because of overlapping pelvic symptoms. The patient presented with progressive urinary dysfunction, saddle anesthesia, and lower-extremity symptoms. Radiographic evaluation demonstrated high-grade L5–S1 dysplastic spondylolisthesis with severe canal compromise and lumbosacral deformity. Surgical treatment involved neural decompression and controlled deformity correction with sacral dome osteotomy and interbody fusion performed under provisional stabilization. Postoperatively, the patient demonstrated meaningful neurological recovery with improvement of urinary symptoms and restoration of lumbosacral alignment. This case highlights that CES can occur as an initial manifestation of dysplastic spondylolisthesis and underscores the importance of early spinal evaluation and timely surgical treatment with appropriate reduction techniques to prevent further neurological deterioration in patients with persistent neurological symptoms.
Dysplastic spondylolisthesis is a developmental subtype characterized by congenital abnormalities of the lumbosacral junction, including facet joint dysplasia, sacral dome deformity, and posterior element deficiency, resulting in inherent instability and progressive anterior translation of L5 on S1.1-3) It predominantly affects pediatric and adolescent patients and has a higher propensity for progression to high-grade slippage.1,2) Dysplastic spondylolisthesis is also commonly associated with lumbosacral kyphosis and abnormal spinopelvic alignment, which may further contribute to deformity progression and biomechanical instability.4) Neurological manifestations in dysplastic spondylolisthesis are typically gradual and most commonly present as radiculopathy related to foraminal narrowing or nerve root stretching1. In contrast, primary presentation with cauda equina syndrome (CES) is exceedingly rare in dysplastic spondylolisthesis. Most previously reported cases have occurred in the postoperative setting following in situ fusion or reduction procedures.5,6)
The optimal surgical management of high-grade dysplastic spondylolisthesis remains controversial, particularly regarding the degree of reduction and the risk of neurological complications.1,7) Recent studies have emphasized the role of sacral dome osteotomy and careful deformity correction techniques in facilitating safe reduction while minimizing neural tension.7,8)
Herein, we report a rare case of CES associated with dysplastic spondylolisthesis in a patient with concurrent giant ovarian teratomas, in whom overlapping pelvic pathology contributed to delayed spinal diagnosis and surgical treatment. This case highlights that CES can occur as an initial manifestation of dysplastic spondylolisthesis and underscores the importance of maintaining suspicion for spinal pathology in patients with persistent neurogenic symptoms despite treatment of concomitant pelvic disease.
Case Report
A 19-year-old female presented to the emergency department with a 6-month history of urinary incontinence. The symptoms worsened during the preceding month. Neurological examination revealed sensory deficits in the bilateral S1–3 dermatomes, with approximately 30%–40% decreased sensation. Motor function of both lower extremities was intact without definite weakness. Initial abdominal-pelvic computed tomography demonstrated large bilateral mature cystic ovarian teratomas measuring approximately 14 cm in diameter (Fig. 1). Initially, the urinary symptoms were presumed to be secondary to compression by the large pelvic masses and the patient underwent bilateral ovarian cystectomy for bilateral mature cystic ovarian teratomas on the day of admission. However, the urinary symptoms persisted postoperatively. Because symptoms failed to improve after gynecologic surgery, orthopedic consultation was obtained. Standing radiographs and computed tomography (CT) demonstrated high-grade dysplastic spondylolisthesis at L5–S1 (Meyerding grade III) with a preoperative slip percentage of 55%. Magnetic resonance imaging demonstrated severe central canal stenosis and bilateral L5 nerve root compression (Figs. 2, 3). Characteristic radiographic features, including vertically oriented facet joints, sacral dome deformity, and elongation of the L5 pars interarticularis, were identified on CT (Fig. 4). CES secondary to dysplastic spondylolisthesis was considered the most likely diagnosis.
The patient subsequently underwent L5–S1 posterior lumbar interbody fusion with neural decompression. Direct decompression alone was considered hazardous because further slippage during surgery could worsen neural compression. Therefore, temporary fixation using reduction pedicle screws and bilateral rod fixation was performed before decompression to stabilize the lumbosacral segment and prevent further slippage during surgery. After provisional stabilization, decompression was carefully performed. Intraoperatively, marked dural tension was observed. Because reduction alone was insufficient to relieve neural tension and restore spinopelvic alignment, sacral dome osteotomy was additionally performed. After sacral dome osteotomy, the set screws were partially loosened, and further reduction was gradually performed using a unilateral blunt dilator. Bilateral interbody cages were then inserted sequentially on each side during the reduction maneuver. Postoperative radiographs demonstrated improvement in lumbosacral alignment, including correction of the Spinal Deformity Study Group lumbosacral angle and slip angle (Fig. 5). Urinary symptoms and sensory deficits gradually improved without postoperative neurologic deterioration. Radiographic alignment and instrumentation were well maintained at the 3-month and 1-year follow-up evaluations, with sustained clinical improvement.
Discussion
Dysplastic spondylolisthesis has a higher propensity for progression to high-grade slippage and is frequently associated with lumbosacral kyphosis and biomechanical instability.1,4) Neurological manifestations of dysplastic spondylolisthesis are typically gradual and most commonly present as radiculopathy, whereas CES is rare and has been reported predominantly in the postoperative setting rather than as a primary presentation.5,6) In the present case, concurrent giant ovarian teratomas further complicated the diagnostic process because the patient’s progressive urinary dysfunction and saddle anesthesia initially overlapped with symptoms potentially attributable to pelvic pathology. Previous reports have described CES following in situ fusion or reduction procedures in high-grade spondylolisthesis, suggesting vulnerability of the neural elements to mechanical stress and stretch injury.5,6) In contrast, the present case presented with CES as the primary presentation without prior surgical intervention, indicating that dysplastic spondylolisthesis itself may cause critical neural compression in the setting of progressive deformity and instability.
The mechanisms underlying CES in this setting likely involve central canal compromise from anterior translation and dynamic neural tension related to lumbosacral kyphosis and abnormal sacral morphology.4,9) These considerations are supported by prior reports of CES following in situ fusion or reduction procedures in high-grade spondylolisthesis, highlighting the vulnerability of the cauda equina to mechanical stress and stretch.6) Interestingly, despite a delay in surgical treatment, the patient demonstrated meaningful recovery of cauda equina symptoms following decompression and reduction. This observation may suggest that neural compromise was influenced not only by static canal narrowing, but also by dynamic or positional mechanical compression related to instability at the lumbosacral junction.
Surgical management of high-grade dysplastic spondylolisthesis has evolved from traditional in situ fusion toward deformity correction and reduction techniques with increasing emphasis on restoration of sagittal alignment.9-11) Hoel et al.9) and Polly et al.11) emphasized that high-grade dysplastic spondylolisthesis should be regarded as a sagittal deformity driven by lumbosacral kyphosis and spinopelvic imbalance, with restoration of lumbosacral lordosis and pelvic alignment representing the principal surgical goal. Although in situ fusion was historically favored to minimize neural traction, reduction and deformity correction techniques are increasingly performed to restore sagittal alignment.10,11) Concerns regarding neural stretch injury remain. However, recent studies have demonstrated favorable clinical and radiological outcomes following partial or complete reduction.12,13) Min et al.8) and Faldini et al.7) emphasized that sacral dome osteotomy facilitates reduction by shortening the posterior column and minimizing neural tension during deformity correction. In addition, Ye et al.13) reported favorable clinical and radiographic outcomes after complete reduction and posterior L5–S1 fusion in pediatric high-grade dysplastic spondylolisthesis. This concept is consistent with our surgical strategy, in which sacral dome osteotomy allowed safe reduction while effectively addressing neural compression. Similarly, Tatsumura et al.14) and Takeda et al.15) also reported satisfactory radiographic and clinical outcomes after posterior lumbar interbody fusion with reduction (Table 1).
Despite these favorable outcomes, reduction in high-grade spondylolisthesis carries a theoretical risk of nerve root stretch injury, particularly involving the L5 nerve root and the cauda equina. In this context, sacral dome osteotomy has been proposed as a valuable adjunct to facilitate safe reduction by shortening the posterior column and reducing tension on neural elements. Previous studies have suggested that resection of the sacral dome can decrease neural stretch over the posterosuperior sacral margin and thereby reduce the risk of neurological complications during deformity correction.7,8) Although intraoperative neurophysiologic monitoring may serve as a useful adjunct during reduction procedures for high-grade dysplastic spondylolisthesis, its interpretation may be limited in patients with established CES because baseline neurophysiologic signals can already be affected by pre-existing neural dysfunction. In the present case, temporary stabilization with reduction pedicle screws and a bilateral rod was performed prior to decompression in order to prevent further slip progression and facilitate controlled reduction with sacral dome osteotomy and interbody fusion while minimizing neural tension. This strategy allowed decompression and sacral dome osteotomy to be performed under provisional stability before definitive reduction and fusion, which may be advantageous in dysplastic spondylolisthesis with coexisting canal compromise and lumbosacral instability. Progressive urinary dysfunction, particularly involuntary urinary leakage without urinary urge or subtle cauda equina symptoms should prompt early spinal evaluation and surgical consideration. Surgical strategies emphasizing provisional stabilization prior to decompression, followed by controlled reduction with sacral dome osteotomy and interbody fusion with further reduction, may help minimize neurological deterioration while achieving safe neural decompression and lumbosacral stabilization.
Although limited by the nature of a single case report, this case demonstrates that cauda equina syndrome, although exceedingly rare, can occur as an initial manifestation of dysplastic spondylolisthesis. This finding underscores the importance of early recognition and timely spinal evaluation in patients with progressive neurogenic symptoms. Carefully planned surgical strategies incorporating neural decompression, provisional stabilization, controlled reduction, and lumbosacral reconstruction may provide meaningful neurological recovery even in delayed presentations.
Jin-Sung Park, a contributing editor of the Journal of Advanced Spine Surgery, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Funding
None.
Acknowledgments
None.
Fig. 1.
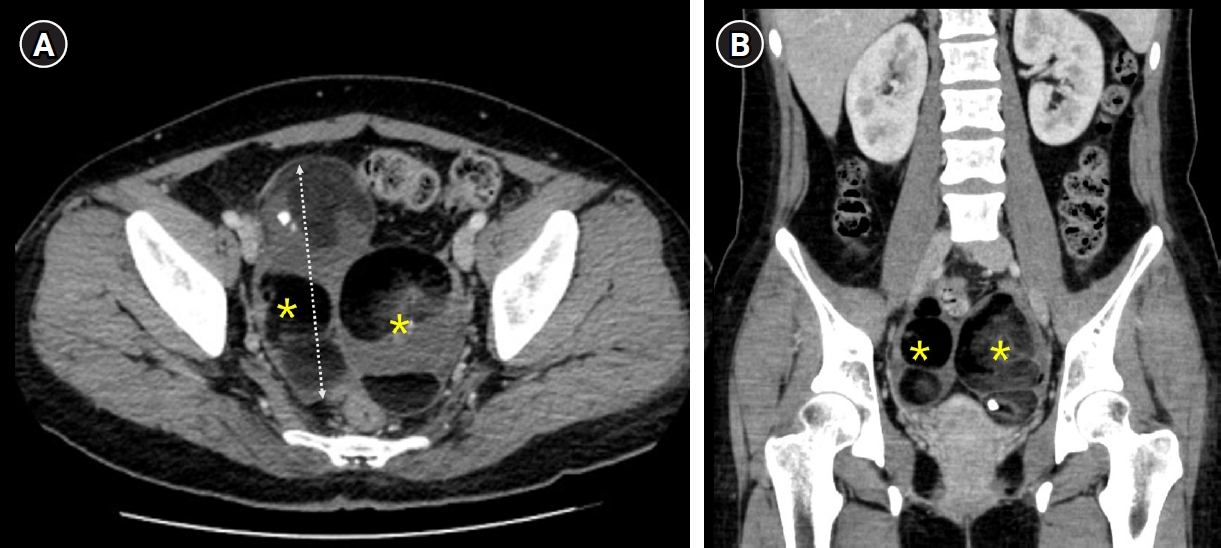
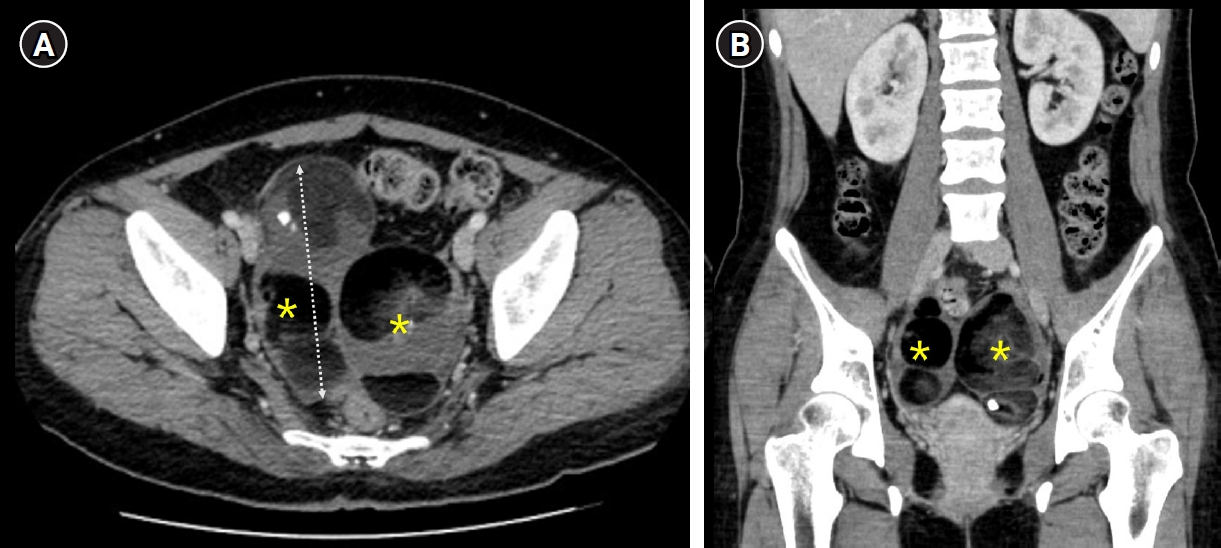
Abdominal-pelvic computed tomography demonstrating bilateral mature cystic teratomas occupying the pelvic cavity. (A) Axial computed tomography (CT) image showing bilateral cystic masses (asterisks) with internal heterogeneous components, measuring approximately 14 cm in diameter (dashed line). (B) Coronal CT image demonstrating bilateral pelvic masses (asterisks) causing mass effect within the pelvic cavity.
Fig. 2.
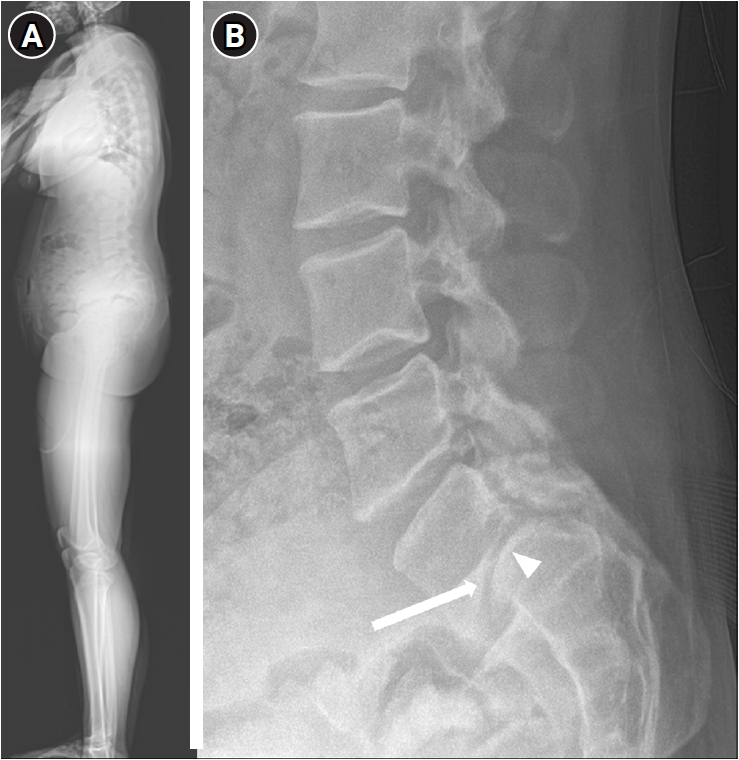
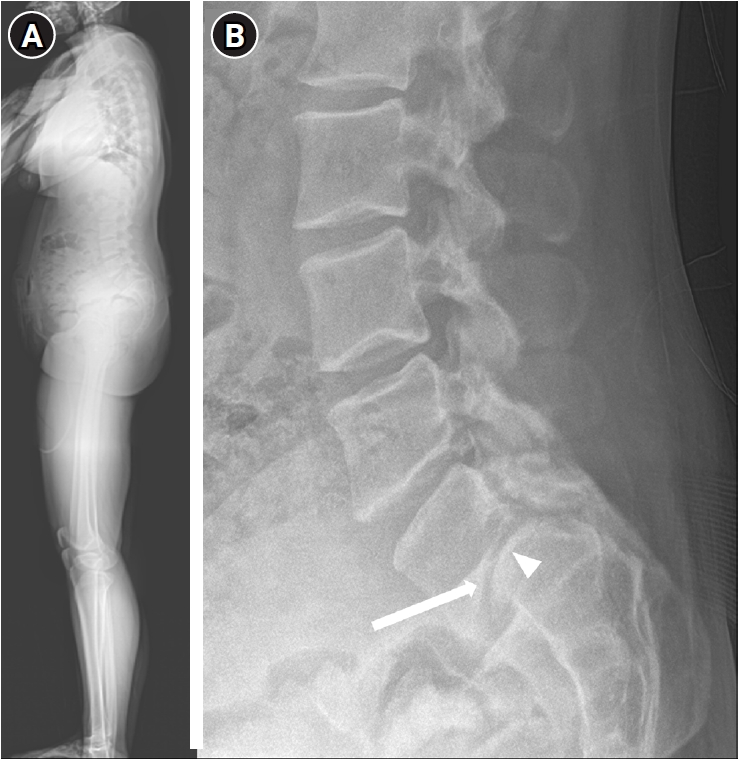
Whole-spine standing lateral radiograph and simple lateral radiograph demonstrating dysplastic spondylolisthesis at the L5–S1 level. (A) Whole-spine standing lateral radiograph showing a stooped sagittal posture, resulting in a characteristic appearance associated with high-grade L5–S1 dysplastic spondylolisthesis. (B) Simple lateral lumbar radiograph demonstrating high-grade anterior slippage of L5 on S1 (arrow) and sacral dome deformity (arrowhead).
Fig. 3.
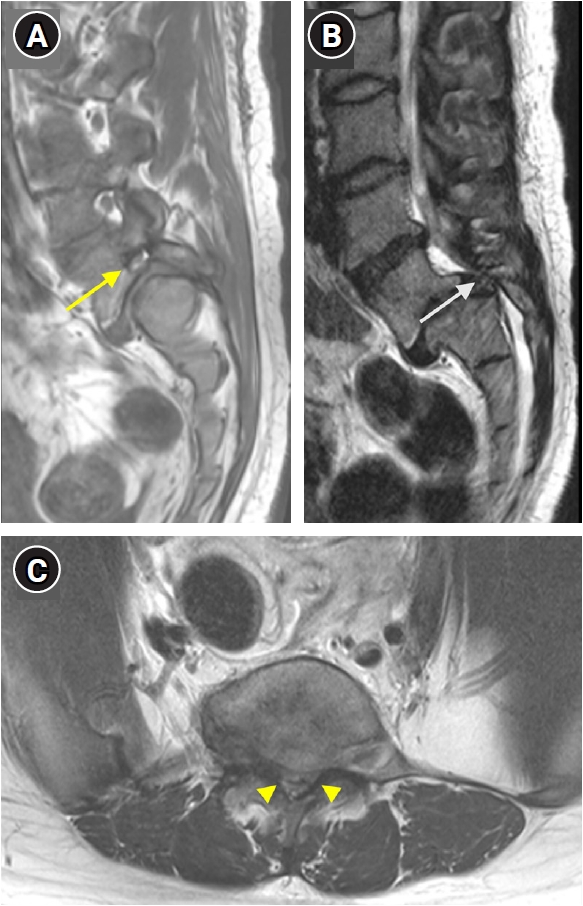
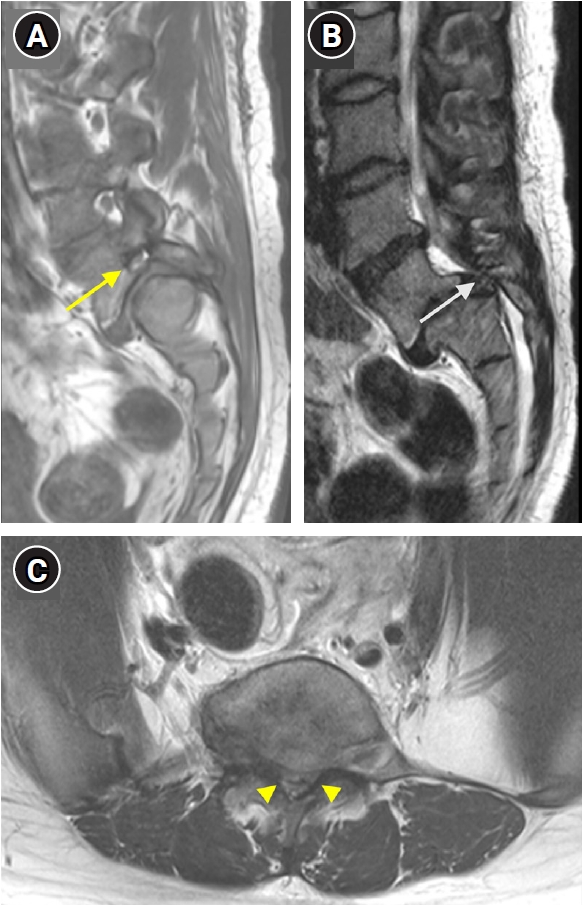
Lumbar spine magnetic resonance imaging demonstrating severe central canal stenosis and foraminal stenosis associated with dysplastic spondylolisthesis at the L5–S1 level. (A) Sagittal T1-weighted magnetic resonance image demonstrating high-grade L5–S1 dysplastic spondylolisthesis with severe foraminal stenosis (yellow arrow). (B) Sagittal T2-weighted magnetic resonance image showing severe central canal stenosis at the L5–S1 level (white arrow). (C) Axial T2-weighted magnetic resonance image demonstrating severe central canal stenosis (yellow arrowheads).
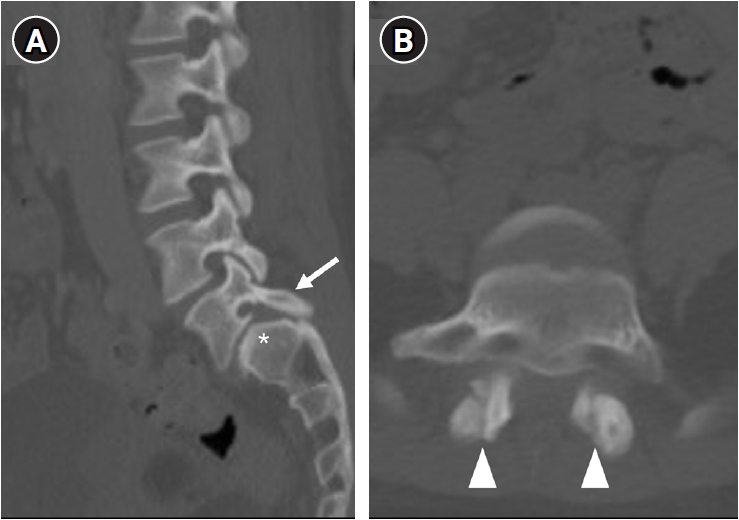
Fig. 4.
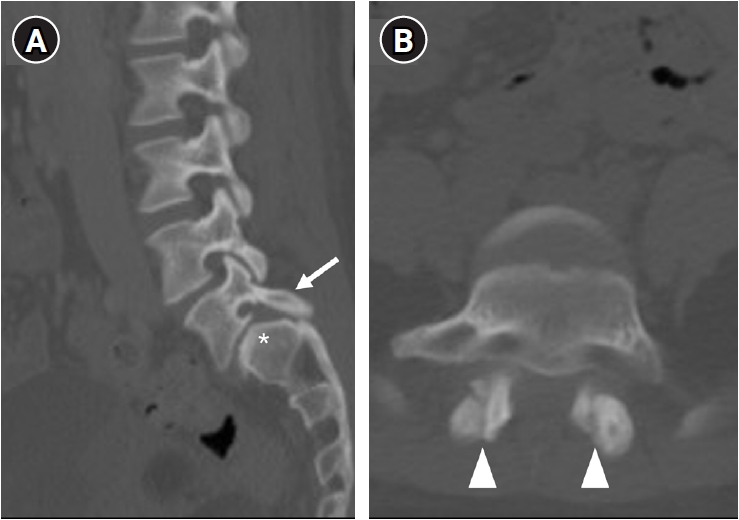
Computed tomography demonstrating characteristic dysplastic features at the L5–S1 level. (A) Sagittal computed tomography (CT) image demonstrating elongation of the L5 pars interarticularis (arrow) and sacral dome deficiency (asterisk). (B) Axial CT image demonstrating vertically oriented L5–S1 facet joints (arrowheads).
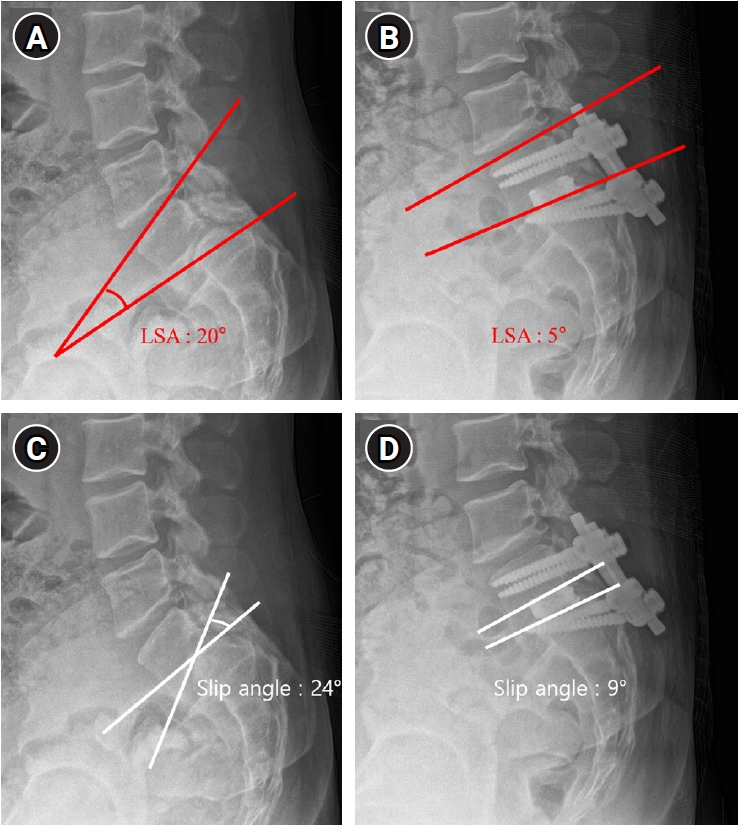
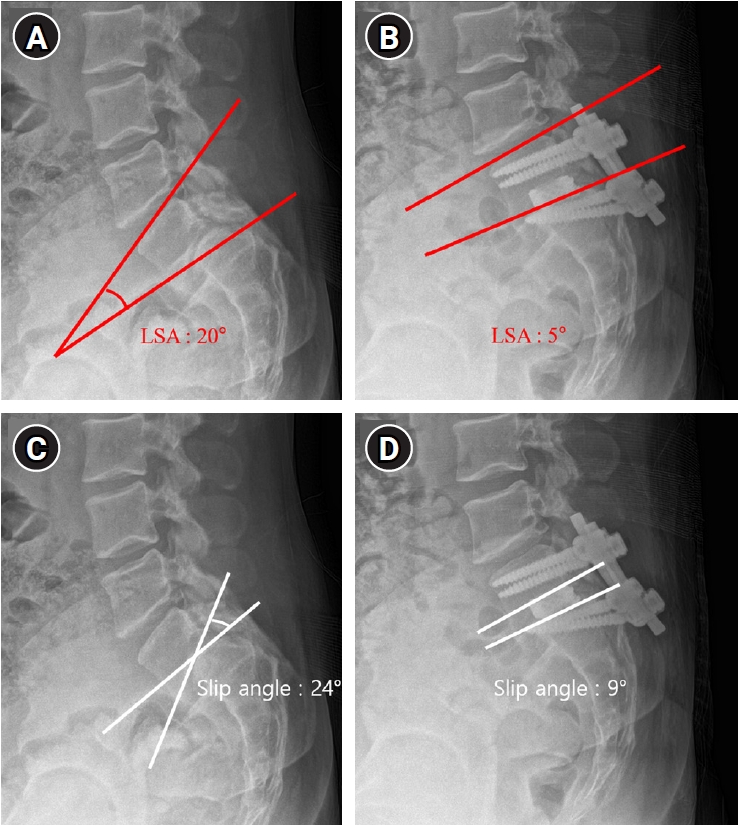
Fig. 5.
Preoperative and postoperative lateral radiographs demonstrating changes in lumbosacral alignment following surgical correction. (A, B) Measurement of the Spinal Deformity Study Group (SDSG) lumbosacral angle (LSA) on preoperative and postoperative radiographs, respectively. The SDSG LSA, measured between the superior endplate of L5 and the superior endplate of S1, improved from 20° preoperatively to 5° postoperatively (red lines). (C, D) Measurement of slip angle on preoperative and postoperative radiographs, respectively. The slip angle, measured between the inferior endplate of L5 and the superior endplate of S1, improved from 24° preoperatively to 9° postoperatively (white lines).
Table 1.
Representative studies of reduction strategies for high-grade dysplastic spondylolisthesis
1. Lamartina C, Zavatsky JM, Petruzzi M, Specchia N. Novel concepts in the evaluation and treatment of high-dysplastic spondylolisthesis. Eur Spine J 2009;18 Suppl 1:133-42.
5. Alzakri AA. Cauda equina syndrome a rare early surgical complication in a pediatric patient with dysplastic high-grade lumbosacral spondylolisthesis: a case report. J Musculoskelet Surg Res 2022;6:283-7.
6. Maurice HD, Morley TR. Cauda equina lesions following fusion in situ and decompressive laminectomy for severe spondylolisthesis: four case reports. Spine (Phila Pa 1976) 1989;14:214-6.
7. Faldini C, Barile F, Ialuna M, et al. High-grade dysplastic spondylolisthesis: surgical technique and case series. Musculoskelet Surg 2023;107:323-31.
8. Min K, Liebscher T, Rothenfluh D. Sacral dome resection and single-stage posterior reduction in the treatment of high-grade high dysplastic spondylolisthesis in adolescents and young adults. Eur Spine J 2012;21 Suppl 6:S785-91.
9. Hoel RJ, Brenner RM, Polly DW Jr. The challenge of creating lordosis in high-grade dysplastic spondylolisthesis. Neurosurg Clin N Am 2018;29:375-87.
10. Elias E, Daoud A, Elias C, Chiu RG, Sanchez JM, Nasser Z. Historical evolution, management, and outcome of surgical treatment for high-grade spondylolisthesis: a systematic review. J Neurosurg Spine 2025;42:784-96.
12. Stulik J, Geri G, Barna M, Klezl Z. High-grade high-dysplastic lumbosacral spondylolisthesis in children treated with complete reduction and single-level circumferential fusion: a prospective case series. Brain Spine 2022;2:100871.
13. Ye X, Guo D, Zhao Y, et al. Posterior L5-S1 fusion with complete reduction for pediatric high-grade dysplastic spondylolisthesis: a multicenter retrospective case series with exploratory analysis of residual sagittal imbalance. BMC Musculoskelet Disord 2026;27:314.
14. Takeda K, Suzuki S, Ozaki M, et al. Influence of slippage reduction and correction of lumbosacral kyphosis by single-level posterior lumbar interbody fusion on spinal alignment in patients with dysplastic spondylolisthesis. Spine Deform 2024;12:1761-72.
15. Tatsumura M, Funayama T, Eto F, Nagashima K, Takeuchi Y, Yamazaki M. Posterior lumbar interbody fusion for dysplastic lumbar spondylolisthesis with high-grade slippage in two adolescent siblings: two case reports. J Med Case Rep 2022;16:331.
16. Martiniani M, Lamartina C, Specchia N. "In situ" fusion or reduction in high-grade high dysplastic developmental spondylolisthesis (HDSS). Eur Spine J 2012;21 Suppl 1:S134-40.
17. Bouyer B, Bachy M, Courvoisier A, Dromzee E, Mary P, Vialle R. High-grade lumbosacral spondylolisthesis reduction and fusion in children using transsacral rod fixation. Childs Nerv Syst 2014;30:505-13.
18. Tian W, Han XG, Liu B, et al. Posterior reduction and monosegmental fusion with intraoperative three-dimensional navigation system in the treatment of high-grade developmental spondylolisthesis. Chin Med J (Engl) 2015;128:865-70.
19. Thomas D, Bachy M, Courvoisier A, Dubory A, Bouloussa H, Vialle R. Progressive restoration of spinal sagittal balance after surgical correction of lumbosacral spondylolisthesis before skeletal maturity. J Neurosurg Spine 2015;22:294-300.
20. Hadgaonkar S, Nagpal S, Bhute AR, Sancheti P. Navigation-assisted reduction and fusion for 3 cases of high-grade pediatric dysplastic spondylolisthesis: a technical note. Surg Neurol Int 2025;16:381.
Delayed Surgical Management of Initial Cauda Equina Syndrome Due to Concurrent Giant Ovarian Teratomas: A Case Report and Literature Review
Fig. 1. Abdominal-pelvic computed tomography demonstrating bilateral mature cystic teratomas occupying the pelvic cavity. (A) Axial computed tomography (CT) image showing bilateral cystic masses (asterisks) with internal heterogeneous components, measuring approximately 14 cm in diameter (dashed line). (B) Coronal CT image demonstrating bilateral pelvic masses (asterisks) causing mass effect within the pelvic cavity.
Fig. 2. Whole-spine standing lateral radiograph and simple lateral radiograph demonstrating dysplastic spondylolisthesis at the L5–S1 level. (A) Whole-spine standing lateral radiograph showing a stooped sagittal posture, resulting in a characteristic appearance associated with high-grade L5–S1 dysplastic spondylolisthesis. (B) Simple lateral lumbar radiograph demonstrating high-grade anterior slippage of L5 on S1 (arrow) and sacral dome deformity (arrowhead).
Fig. 3. Lumbar spine magnetic resonance imaging demonstrating severe central canal stenosis and foraminal stenosis associated with dysplastic spondylolisthesis at the L5–S1 level. (A) Sagittal T1-weighted magnetic resonance image demonstrating high-grade L5–S1 dysplastic spondylolisthesis with severe foraminal stenosis (yellow arrow). (B) Sagittal T2-weighted magnetic resonance image showing severe central canal stenosis at the L5–S1 level (white arrow). (C) Axial T2-weighted magnetic resonance image demonstrating severe central canal stenosis (yellow arrowheads).
Fig. 4. Computed tomography demonstrating characteristic dysplastic features at the L5–S1 level. (A) Sagittal computed tomography (CT) image demonstrating elongation of the L5 pars interarticularis (arrow) and sacral dome deficiency (asterisk). (B) Axial CT image demonstrating vertically oriented L5–S1 facet joints (arrowheads).
Fig. 5. Preoperative and postoperative lateral radiographs demonstrating changes in lumbosacral alignment following surgical correction. (A, B) Measurement of the Spinal Deformity Study Group (SDSG) lumbosacral angle (LSA) on preoperative and postoperative radiographs, respectively. The SDSG LSA, measured between the superior endplate of L5 and the superior endplate of S1, improved from 20° preoperatively to 5° postoperatively (red lines). (C, D) Measurement of slip angle on preoperative and postoperative radiographs, respectively. The slip angle, measured between the inferior endplate of L5 and the superior endplate of S1, improved from 24° preoperatively to 9° postoperatively (white lines).
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Delayed Surgical Management of Initial Cauda Equina Syndrome Due to Concurrent Giant Ovarian Teratomas: A Case Report and Literature Review

 , Jae-Won Hur, M.D.*
, Jae-Won Hur, M.D.*