
| Seung-Hwan Yoon | 3 Articles |
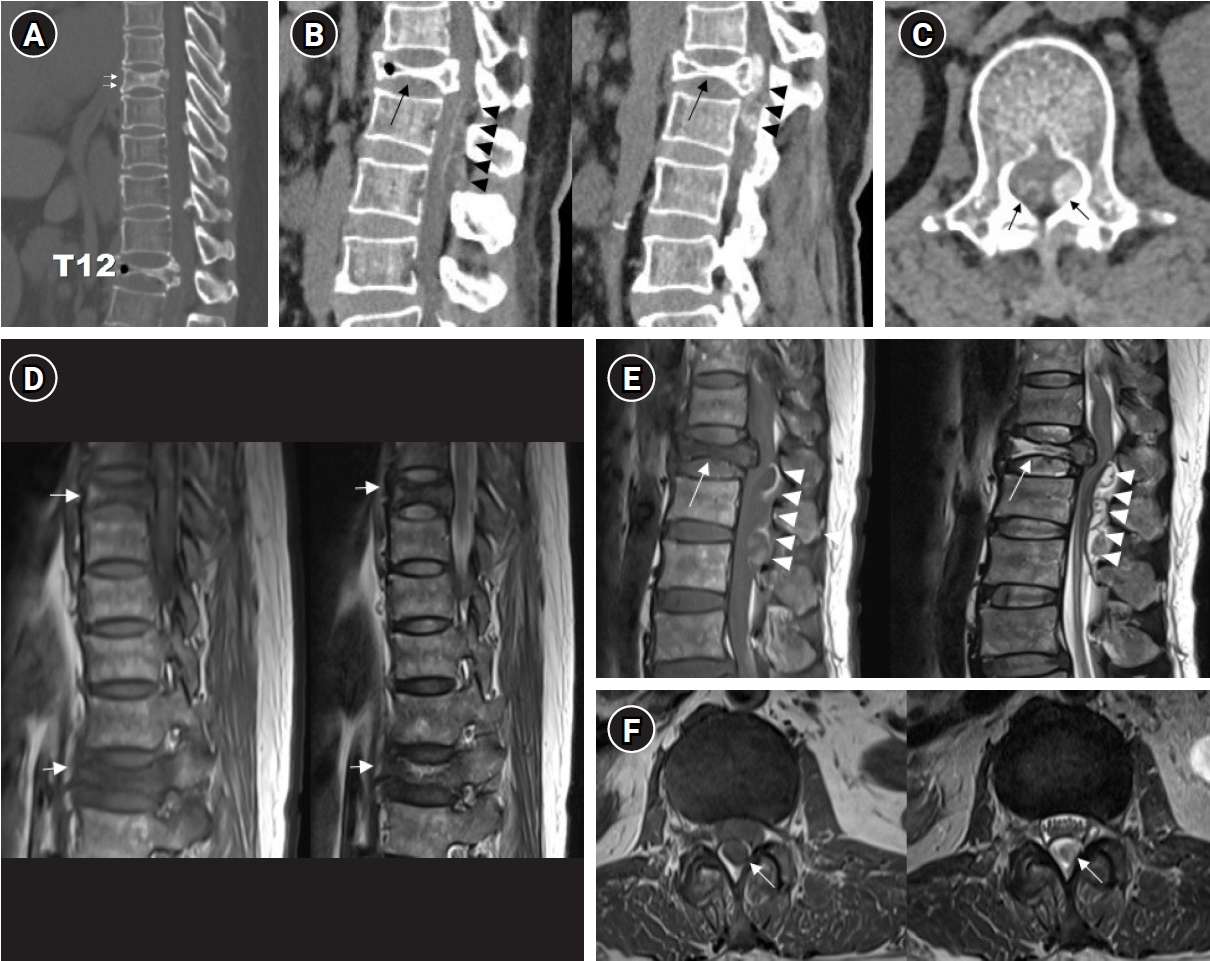
The incidence of compression fractures is increasing in aging populations. Differentiating pathological fracture types is complex and requires careful consideration during diagnosis. This case report describes the clinical course of a 54-year-old female patient presenting with progressive paraplegia after a back injury sustained while lifting a heavy object. Initial imaging revealed a burst fracture at T12 and severe spinal cord compression due to an epidural mass extending from T12 to L2. Clinical assessment raised suspicions of a hematologic malignancy or pathological fractures. Laminectomy and spinal fusion, along with mass removal, resulted in partial improvement in motor function and patient-reported pain levels. However, further evaluation and biopsy revealed chronic inflammation with fibrosis consistent with an unresolved hematoma. This case underscores the importance of a comprehensive differential diagnosis and multidisciplinary collaboration, integrating radiologic, surgical, and pathologic correlation, in the management of complex spinal pathologies.
Purpose
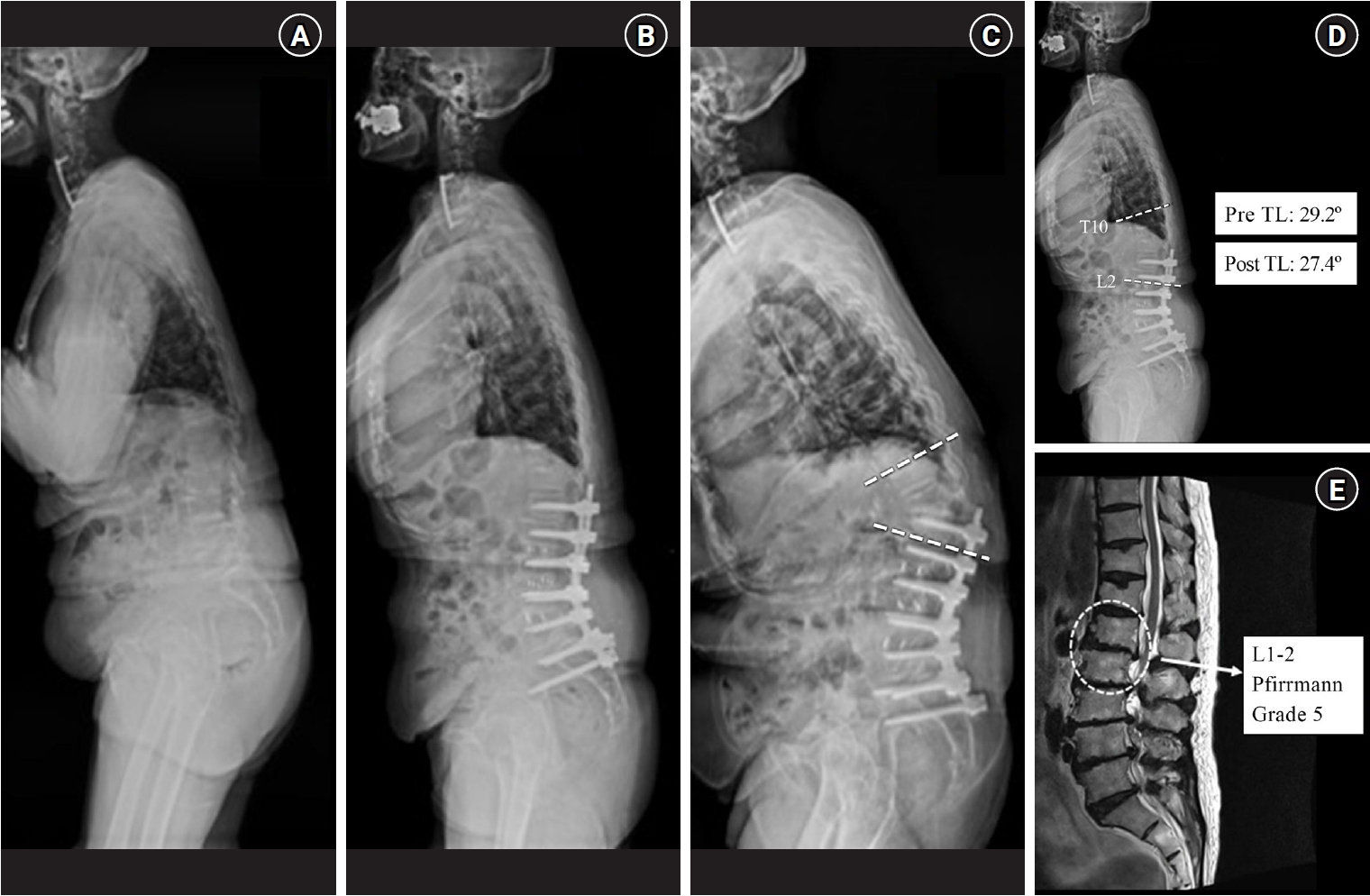
This retrospective study investigated the distinct clinical and radiographic drivers of early- versus late-onset proximal junctional kyphosis (PJK) following multilevel thoracolumbar (TL) fusion. Methods After applying the exclusion criteria (spinal infection, neuromuscular disease, age <50 years), the analysis included 136 patients who underwent ≥4-level TL fusion and were followed up for a minimum of 2 years. PJK was classified as early (≤6 months) or late (>6 months) onset. Patient-related factors, surgical variables, sagittal spinopelvic parameters, and preoperative magnetic resonance imaging findings were analyzed using multivariate logistic regression to identify independent predictors of early PJK. Results Among 24 patients (17.6%) who developed PJK, the early and late-onset groups included 13 and 11 patients, respectively. The early PJK group exhibited significantly greater preoperative and postoperative TL angles compared with the late group (preoperative: 23.03±13.83° vs. 9.67±9.67°, p=0.024; postoperative: 19.6±6.95° vs. 6.95±6.35°, p<0.001). The Pfirrmann grade of the L1–2 intervertebral disc was significantly higher in the early PJK group (3.92±0.95 vs. 2.81±0.60, p=0.006). No surgical variables differed significantly between the groups. Multivariate analysis confirmed greater postoperative TL angle and more advanced L1–2 disc degeneration as independent predictors of early PJK. Conclusion Early-onset PJK following multilevel TL fusion is primarily driven by regional biomechanical vulnerabilities, specifically residual postoperative TL kyphosis and advanced adjacent L1–2 disc degeneration, rather than by surgical variables. Meticulous evaluation of regional TL alignment and adjacent disc health during surgical planning is critical for risk stratification and prevention of early junctional failure.
Objective
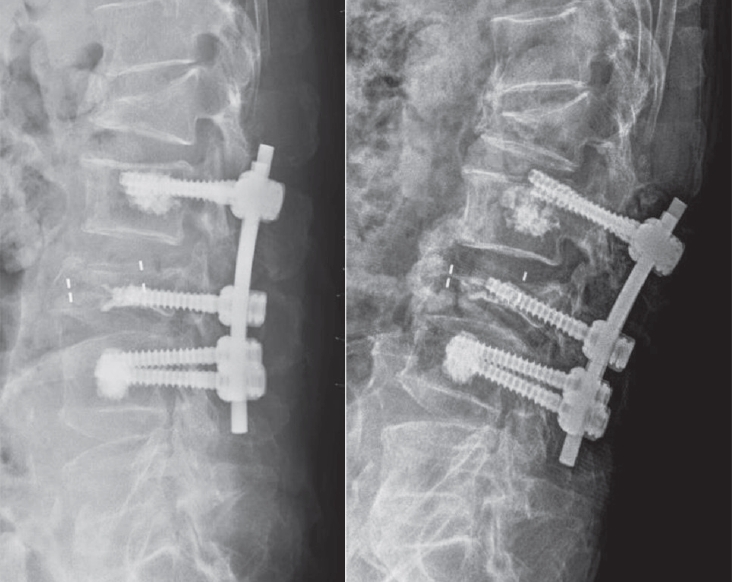
This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws. Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation. Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048). Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
|
|
