Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
Purpose To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
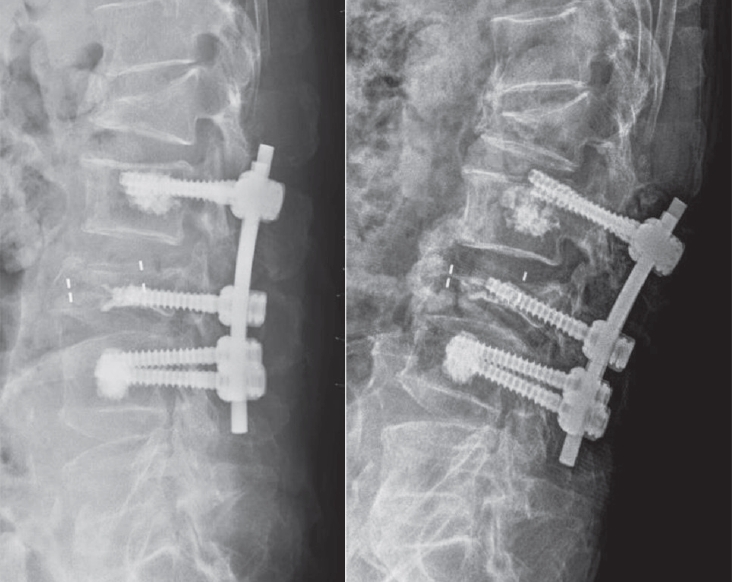
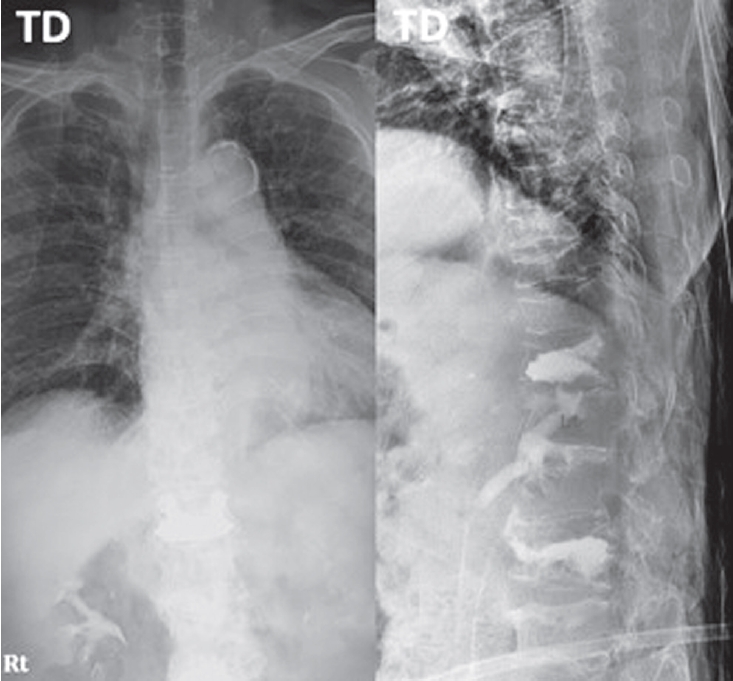
Methods An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
Purpose To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
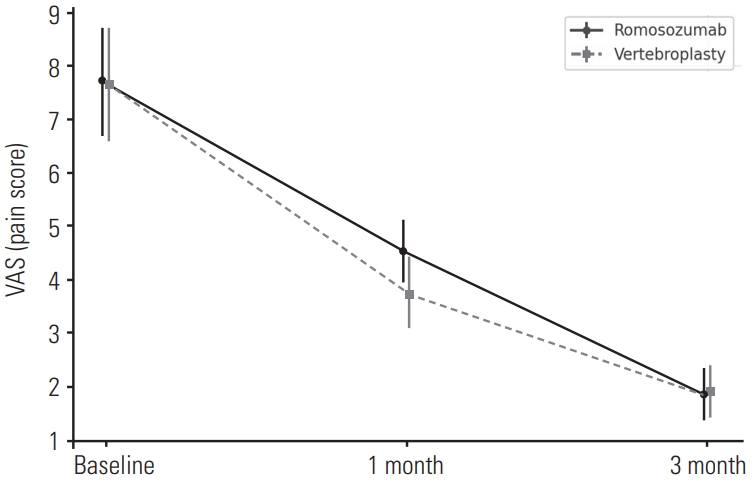
Material and Methods: This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.

 First
First Prev
Prev

