Purpose This study aims to identify risk factors and changes in spino-pelvic parameters associated with Sacroiliac (SI) joint degeneration.
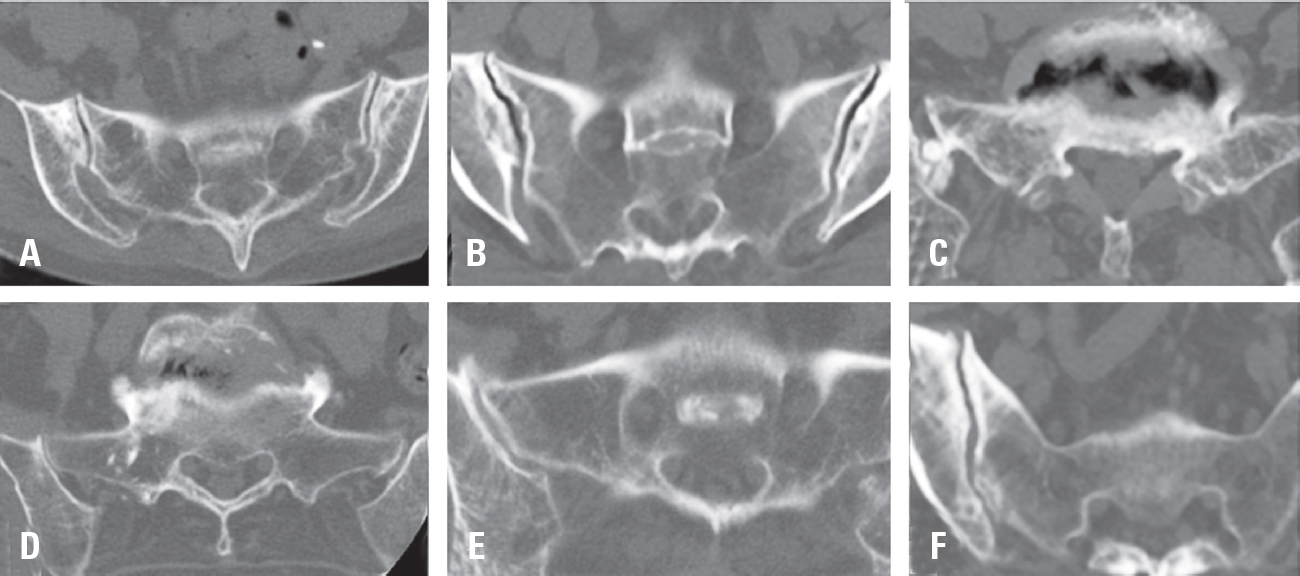
Materials and Methods This multicenter retrospective study included 472 patients who underwent fusion surgery at three hospitals between March 2021 and February 2024. SI joint degeneration was assessed using seven indicators: sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation, and subchondral cysts. CT scans were performed preoperatively and 6 months postoperatively. The patients were divided into two groups: those with progression of SI joint degeneration and those without. Standing whole spine lateral X-rays were used to measure a total of 10 spinopelvic parameters both preoperatively and at 6 months postoperatively. Statistical analysis was performed using two-sample t-tests and multivariable logistic regression.
Results Among the 472 patients, 135 (28.6%) showed progression of SI joint degeneration. When comparing the two groups, age (p=0.022), alcohol consumption (p=0.001), smoking (p<0.001), and S1 involvement (p=.04) were associated with SI joint degeneration. Regarding spino-pelvic parameters, patients with SI joint degeneration exhibited significant changes in thoracic kyphosis (p=0.017) and pelvic tilt (p=0.049).
Conclusions Sacrum fixation, smoking, alcohol consumption, and age can be significant risk factors for SIJ degeneration following lumbar fusion surgery.
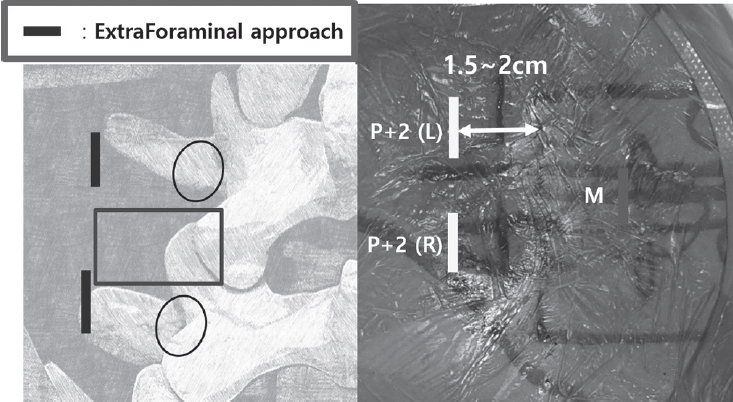
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
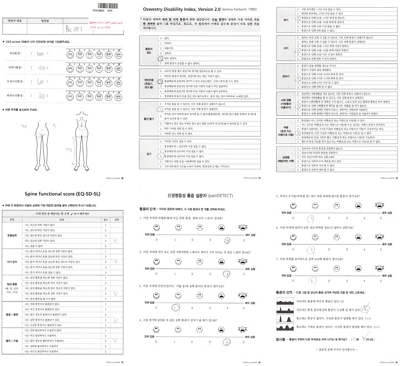
Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
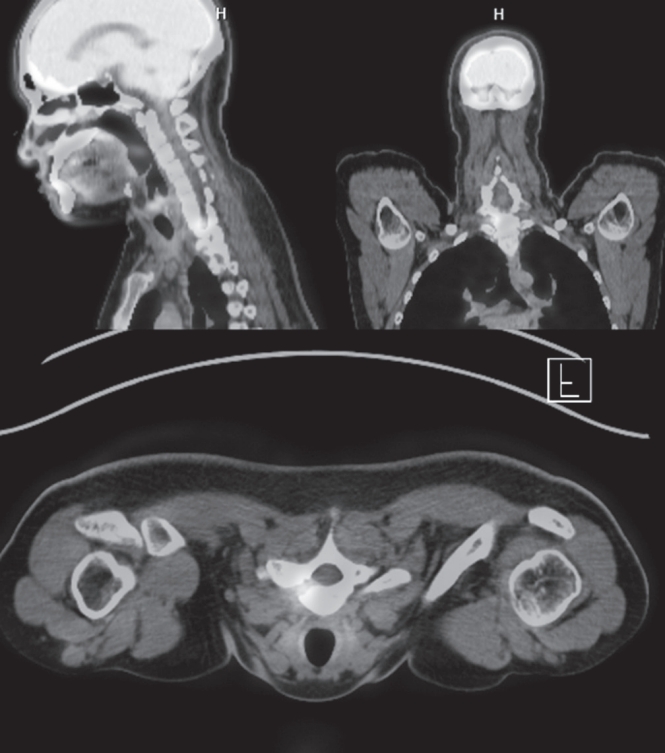
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
Purpose Thoracolumbar vertebral compression fractures (VCFs) are a leading cause of kyphosis and related biomechanical complications, often resulting in chronic back pain and reduced function. Balloon kyphoplasty has been widely used as a minimally invasive intervention to provide pain relief and restore vertebral height. The SpineJack system is a relatively novel technique that introduces mechanical distraction, offering potentially enhanced vertebral restoration. This study aims to compare these two effective treatments for thoracolumbar fractures.
Materials and Methods This study analyzed 30 patients with thoracolumbar VCFs surgically treated, using the Spine-Jack system (n=10) or balloon kyphoplasty (n=20). Back pain was evaluated as VAS pain score and functional disability was assessed with Oswestry Disability Index (ODI) preoperatively and immediately postoperatively.
Radiological outcomes were measured on plain lateral X-rays, including vertebral height restoration, segmental kyphosis angle, and sagittal vertical axis (SVA). Complications, such as cement leakage and adjacent vertebrae fractures, were recorded. Continuous variables – with t-tests and categorical variables- with chi-square tests, were analyzed. P-value less than 0.05 was considered statistically significant.
Results Both the Spine-Jack system and balloon kyphoplasty were effective in reducing back pain and improving patients’ function, with significant improvements in VAS and ODI scores. However, the Spine-Jack system demonstrated superior vertebral height restoration (85% vs. 72%, p=0.03) and segmental kyphosis angle correction (12° vs. 9°, p=0.032) when compared to balloon kyphoplasty. Complication rates were all low and comparable between the two groups.
Conclusions Although the Spine-Jack system and balloon kyphoplasty are all effective for thoracolumbar VCFs, the Spine-Jack system offered superior radiological outcomes in selected cases. Further studies may explore their complementary roles in managing thoracolumbar VCFs.
Objective Postoperative urinary retention (POUR) is a common complication following lumbar spine surgery, significantly affecting functional recovery and Enhanced Recovery After Surgery (ERAS) protocols. POUR can lead to bladder overdistension, infections, prolonged hospital stays, and long-term detrusor dysfunction. Postoperative delirium (POD) can impair cognitive function and mobility, potentially triggering or exacerbating POUR. This study aims to investigate whether POD serves as an independent risk factor for POUR and to analyze other contributing factors to provide clinical management strategies.
Materials and Methods A retrospective cohort study was conducted involving 420 patients who underwent lumbar spine surgery at a single tertiary medical institution between March 2021 and February 2024. POUR was defined as a post-void residual (PVR) bladder volume ≥300 mL measured via bladder ultrasound or requiring catheter reinsertion due to urinary retention. POD was diagnosed within 72 hours postoperatively using the Confusion Assessment Method (CAM) and was classified into three subtypes: hyperactive, hypoactive, and mixed. Multivariate logistic regression analysis was employed to identify the relationship between POD and POUR, with sensitivity and specificity assessed through Receiver Operating Characteristic (ROC) curve analysis.
Results Among 420 lumbar spine surgery patients, 44 (10.5%) experienced POD. Of these, 16 (36.4%) were classified as hyperactive, 20 (45.5%) as hypoactive, and 8 (18.2%) as mixed type. POUR occurred in 28 of the POD patients (63.6%) compared to 71 of 376 patients without POD (18.9%), demonstrating a statistically significant difference (p<0.001). The analysis of POUR incidence by POD subtype revealed rates of 62.5% (10/16) for hyperactive POD, 60.0% (12/20) for hypoactive POD, and 75.0% (6/8) for mixed POD. Patients with mixed POD showed the highest POUR incidence, with a significant difference compared to hyperactive and hypoactive POD (p<0.05). Multivariate logistic regression analysis identified POD as an independent risk factor for POUR, increasing the likelihood by approximately 3.7 times (Odds Ratio, OR: 3.71; 95% Confidence Interval, CI: 1.95–7.06; p<0.001). Among POD subtypes, mixed POD presented the strongest association with POUR, increasing the risk by 4.8 times (OR: 4.84; 95% CI: 2.10–11.15; p<0.001). Hyperactive and hypoactive POD were also significant risk factors, increasing POUR risk by 3.0 times (OR: 3.04; 95% CI: 1.45–6.35; p=0.003) and 3.5 times (OR: 3.48; 95% CI: 1.69–7.19; p=0.001), respectively.
Conclusions This study confirms that postoperative delirium (POD) is an independent risk factor for postoperative urinary retention (POUR) in lumbar spine surgery. The occurrence and subtype of POD significantly influence POUR incidence, with mixed POD presenting the highest risk. These findings highlight the importance of early diagnosis and prevention of POD as a strategy to effectively reduce POUR. A multidisciplinary approach integrating POD and POUR management could optimize postoperative outcomes and improve patient recovery.
Objective The purpose of this study is to investigate the radiological risk factors and differences in spinopelvic parameters for radiologic degenerative changes in the sacroiliac joint after lumbar or lumbosacral fusion surgery.
Materials and Methods From 2019 to 2020, 116 patients diagnosed with lumbar and sacral degenerative diseases who underwent lumbar or lumbar sacral fusion were included. The degenerative changes of the sacroiliac joint were measured by CT performed before and 6 months after surgery, and divided into two groups according to the presence or absence of radiographic degeneration. Evaluation factors for radiographic degeneration include sclerotic changes, erosion, osteophyte formation, intra-articular bone formation, joint space narrowing, intra-articular gas formation and subchondral cysts were evaluated. Spinopelvic radiologic parameters and surgery-related parameters including lumbar lordosis, sacral slope, pelvic incidence, global tilts, and T1PA between the two groups were analyzed using Student's t-tests and chi-square tests to determine the difference between continuous and non-continuous variables between groups. Logistic regression analysis was used for the analysis of risk factors for degeneration for SI joints after lumbar or lumbosacral fusion surgery.
Results There was no statistically significant difference between the demographic data and surgery-related data between the group with and without sacroiliac joint degenerative changes. There was also no statistical difference in the rate of degenerative changes in the sacroiliac joint according to the presence or absence of S1 in the fusion segment. (degeneration group vs non-degeneration group; 45.5% vs 39.8%, p: 0.574) There were statistically significant differences between the two groups in lumbar lordosis (LL), pelvic angle of incidence (PI), and PI-LL. (LL; 27.2±12.0 vs. 39.8±11.3, PI; 51.3±12.0 vs. 57.2±12.6. and PI-LL; 24.1±17.0 vs 17.4±13.9, p: <0.001, 0.023, and 0.030) As risk factors for radiographic degenerative changes in the sacroiliac joint, lumbar lordosis (LL), pelvic incidence (PI), sacral inclination (SS), and sagittal vertical axis (SVA) were statistically significant factors. (lumbar lordosis Odd ratio: 0.851, 95% CI: 0.791-0.917, p-value <0.001)
Conclusions Lumbar lordosis and pelvic incidence are related as risk factors for radiographic degenerative changes in the sacroiliac joint after surgery in patients with lumbar spinal fusion.
Oblique lumbar interbody fusion (OLIF) is one of surgical techniques for patients with spondylolisthesis, but an insertion of cage at an ideal location (anterior 1/3 of disc space) is challenging for patient with high grade spondylolisthesis, because vertebra are not aligned. Recently, a technique of simultaneous insertion of pedicle screw and rod system from the back of patient and insertion of cage via retroperitoneal route from the front of patient is possible by using spinal navigation system (OLIF-360). The author present a case and surgical technique of simultaneous re-alignment of high-grade spondylolisthesis at L4-5 and insertion of interbody cage by using OLIF-360. An intervertebral cage was inserted at the ideal location after re-alignment of spondylolisthesis with OLIF-360. Postoperative images showed re-aligned vertebra and successful decompression. The specific utilization of OLIF-360 has not been underscored yet.
Objective This study aimed to describe the surgical technique in patients with cervical herniated disc treated with unilateral biportal endoscopic spinal surgery.
Materials and Methods Working and viewing portals were created in each unilateral paravertebral area at the target disc level. Under exploring by endoscopic view, effective decompression was possible via safe access to the medial foramen with minimal laminectomy and facetectomy. We evaluated 27 patients, and clinical outcome was analyzed using the visual analogue scale (VAS), Neck disability index (NDI), Macnab criteria, and motor function of involved upper extremity, all assessed before and 3, 6 months post procedure.
Results The VASs for axial neck pain and upper extremity pain decreased from 6.8 to 1.9 and 7.7 to 1.5, respectively, at 6 months post procedure. The NDIs were improved from 45.5 to 13.0 at 6 months post procedure. According to the Macnab criteria, an ‘Excellent’ , ‘Good’ , and ‘Fair’ result was obtained in 55.6%, 29.6%, and 14.8% subjects, respectively.
The motor power of involved upper extremity improved as an approximately one grade on average at 6 months post procedure; 3.9±0.8 to 4.8±0.4.
Conclusions Unilateral biportal endoscopic spinal cervical surgery can be an efficient and safe intervention in patients with cervical herniated disc.
Objectives The primary surgical goals when treating a spinal metastasis are usually pain relief and preservation of ambulatory function. Minimally invasive techniques have become popular, being associated with less morbidity and mortality than conventional open surgeries.
Materials and Methods Between April 2012 and September 2016, 15 consecutive patients underwent percutaneous pedicle screw fixation (PPSF) to treat spinal metastases. We retrospectively analyzed prospectively collected data, including visual analog scale (VAS) pain scores, Frankel scale scores, and complications.
Results Fifteen patients (8 males, 7 females; mean age 61 years) underwent surgery under general anesthesia. PPSF was performed on all patients, and two with poor bone quality underwent cement augmentation of the manipulated vertebra(e) just prior to pedicle screw insertion. Seven patients underwent fixation plus distraction (indirect decompression via ligamentotaxis) and two laminectomies (direct decompression) of the spinal cord. Two patients developed screw pullout requiring revision surgery. One patient died 7 days after surgery from liver cirrhosis and sepsis. All patients reported that pain was reduced after surgery. After surgery, 12 patients regained ambulatory capacity. Nine patients died during follow-up; the mean overall survival time was 14.1 months.
Conclusions PPSF is a safe and minimally invasive palliative surgery option for patients with spinal metastases.
Recently, favorable results of minimally invasive spinal surgery have been reported in comparison to the open decompression or fusion surgery. Biportal endoscopic spine surgery (BESS) has several benefits and Indications for BESS are nearly identical to those for general open spinal surgery. However, it remains a challenging procedure even for an experienced endoscopic surgeon. because it takes a a long operation time while early learning period. If the operation time is prolonged, the advantages of endoscopic surgery are reduced and the incidence of complications can be increased. Therefore, we will investigate the factors affecting the operation time and how to minimize it before and during operation.
Background Context: There are few reports of changes in global sagittal alignment and corresponding factors like hand grip strength (HGS) and muscle performance tests to detect changes in global sagittal alignment after surgery for lumbar spinal stenosis (LSS).
Purpose The purpose of the study was to determine whether HGS can be a useful predictive marker of global sagittal alignment changes after decompression with fusion surgery for LSS.
Study Design: This is a retrospective observational study.
Patient Sample: Patients who underwent spine surgery for LSS were included in the present study.
Outcome Measures: Radiological spinopelvic parameters including sagittal vertical axis (SVA), lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), global tilt (GT), and T1 pelvic angle (T1PA) were assessed. Clinical outcomes parameters like Oswestry Disability Index (ODI), Euro-QOL (EQ-5D), visual analog scale (VAS) scores for back or leg pain were assessed. To assess muscle performance, three functional mobility tests (6-meter walk test, timed up and go test, sit-to-stand test) and HGS were checked.
Materials and Methods A total 91 consecutive patients who underwent spine fusion surgery for LSS were included. 1 year after posterior decompression and fusion surgery, the patients were further classified into four groups according to preoperative and postoperative SVA. We analyzed radiological parameters like SVA, LL, PT, PI, GT, and T1PA. The ODI, the EQ-5D and VAS scores for back or leg pain were recorded as clinical outcomes assessment. To assess muscle performance, SMT, TUGT, STS, and HGS were checked.
Results HGS was significantly correlated with age, postoperative SVA, ODI, EQ-5D and muscle performance test. HGS was related with change of preoperative sagittal alignment 1yr after surgery. Using a receiver operating characteristic (ROC) curve to determine the cutoff values of HGS as predictors of postoperative balanced sagittal alignment according to SVA, cutoff value of HGS demonstrated 19.5 kg with a sensitivity of 82.1% and specificity of 66.7%.
Conclusion Patients with non-balanced sagittal alignment in LSS demonstrated decreased muscle function and muscle strength. If the muscle strength was weak in the group in which the sagittal balance was maintained preoperatively, it could be converted to non-balanced sagittal alignment. Thus, preoperative HGS may be a good predictor of postoperative SVA change.
Purpose of Study: Purpose of this study is to summarize the technique of UBE surgery in lumbar interbody fusion and review the clinical outcomes and complications of UBE surgery in lumbar interbody fusion.
Materials and Methods Medical databases were searched for the key words of unilateral biportal endoscopic surgery and lumbar spinal stenosis using PubMed from 2005 to the present.
Conclusion UBE spinal surgery is a new technique that can be a feasible alternative and an effective treatment modality for spinal degenerative diseases and can achieve the necessary surgical skills for experienced microscopic surgeons, which is still expanding the indications for lumbar spinal surgery.
Objectives We report the new minimally invasive technique and its clinical results of oblique lumbar interbody fusion (OLIF) combined with central decompression using biportal endoscopic spinal surgery (BESS).
Summary of Literature Review: The OLIF procedure is one of the minimally invasive spine surgeries and is being frequently attempted recently to treat lumbar degenerative disease. It has been reported that it effectively decompresses foraminal stenotic lesions indirectly by inserting a large cage anteriorly, which reduces spondylolisthesis and widens the disc space. However, OLIF has limited effect for severe central canal stenosis, since it cannot achieve direct decompression. Therefore, authors report a new minimally invasive technique of OLIF combined with direct central decompression using BESS for severe central stenosis along with its clinical results as a pilot study.
Materials and Methods For patients who were candidate for fusion surgery due to spondylolisthesis (more than one segment) or foraminal stenosis, authors performed OLIF and central decompression using BESS simultaneously, when the patients had concomitant severe central canal stenosis. From June to December, 2017, 8 patients (16 levels) were enrolled, the operative time, blood loss, complications and clinical results have been evaluated. The clinical results were analyzed by Visual analog scale (VAS) scores, Oswestry disability index (ODI) and Roland Morris Disability Questionnaire (RMDQ) of preoperative, 1month, 3month postoperative and final follow-up.
Results Mean operative time and blood loss were 238.4 minutes and 173.3ml, respectively. In all cases, there were no operative complications, and mean follow-up period was 7.1 months. The mean back VAS, lower extremity VAS, ODI, and RMDQ at the final follow-up were improved from 5.4±2.4 to 2.0±0.9, 7.0±1.1 to 1.6±1.7, 64.2±11.8 to 44.2±10.6, and from 17.5±4.2 to 12.9±4.0.
Conclusion A new combination technique of OLIF and BESS for direct decompression can be regarded as effective alternative procedure to treat the foraminal and central stenotic lesions of lumbar degenerative disease.
The foramen of L5-S1 can develop several degenerative diseases such as extraforaminal lumbar disc herniation, foraminal stenosis with disc height collapse, degenerative or spondylolytic spondylolisthesis, and far-out syndrome.
The floating technique in biportal endoscopic spine surgery (BESS) keeps a certain distance between instruments and spinal structures. 1) This key point makes the floating technique different from conventional endoscopic surgery, which uses the Kambin’s safe triangle as a work zone. The floating view can enable the surgeon to see the structures panoramically, under high magnification: consequently, fine discrimination of their margin and safe manipulation of neural structures can be guaranteed. A certain gap between the floating scope and lesion can permit various instruments, generally used in open spine surgery, to be inserted from the sides with fewer limitations. Extraforaminal or foraminal lesions under the lamina can be reached by avoiding the iliac crest, and total facetectomy, which has the potential of iatrogenic instability, is not required to explore the foraminal structures. However, the floating view can be obstructed by small bleeds from laminectomized bone and/or surrounding vessels. This present article describes the technique and provides tips on how to perform BESS with floating technique safely and successfully for various lesions at the L5-S1 foramen.
The minimally invasive technique to correct deformity in scoliosis is not a familiar concept among spine surgeons but is interesting, as this innovative surgery, if it proves successful, will have the advantages of the minimally invasive technique in the final outcomes and will be the future of scoliosis surgery. We operated on 18 adolescent idiopathic scoliosis (AIS) patients using a newly designed technique which utilizes two or three 1-inch midline incisions to insert pedicle screws with a rod, facet fusion and de-rotation maneuver to correct the deformity. Post-operative complications were minimal and the results of the deformity corrections were comparable to the open scoliosis surgery in the follow up. The advantages of minimally invasive surgery observed in all cases include cosmetically fainter scars, reduced blood loss, shorter hospital stay, early mobilization and minimal need of analgesics for pain.
Even though many challenges were faced in executing this procedure, the goal of inventing this novel approach was accomplished. We feel this technique is a good alternative to open surgery in certain curve types of AIS but large scale studies are needed in the future to recommend its routine use.
Purpose The purpose of this study was to determine the early failure rate of percutaneous epidural neuroplasty (PEN) that led to subsequent decompressive lumbar surgery. We also assessed the limits of spinal pain management by using the current PEN technique.
Materials and Methods We classified 1763 cases according to their diagnoses and radiological findings. Patients who underwent subsequent open surgery when PEN failed to improve or aggravated their symptoms were included.
Results All 37 patients underwent open decompressive surgery within 3 months after PEN. There were 18 in the intracanalicular focal herniation category, 11 in intracanalicular broad based herniation category, and 8 in foraminal category; the early failure rates were 1.7%, 1.9%, and 5.6%, respectively. There was no significant statistical difference between the intracanalicular categories with regard to failure rate, but the foraminal category had a higher rate of failure than that of intracanalicular categories (p<0.05). Moreover, there were 11 cases in intracanalicular categories that experienced deterioration or new symptoms due to posterior longitudinal ligament rupture or fragment migration. Among these, there were 9 cases (82%) with preexisting intracanalicular migrating fragments.
Conclusion PEN with targeted drug delivery may be an effective treatment for low back pain and/or radiculopathy.
However, its early failure rate is at least 2.1%, and the presence of intracanalicular migrating fragments or symptomatic foraminal lesions are predictors of poor outcome. Patients must be carefully selected on the basis of thorough radiologic reviews to improve the rate of satisfactory PEN outcomes.
Purpose of study: The purpose of this study is to understand the biomechanics of interspinous devices in lumbar spinal surgery and to review the effectiveness of the devices for lumbar spinal stenosis through recent related articles.
Materials and Methods Medical databases were searched for the key words of interspinous device and lumbar spinal stenosis using PubMed from 2010 to the present.
Results Several studies have shown sustained symptomatic improvements after interspinous device insertion.
However, most of the prospective, randomized, double-blinded studies have shown that it is not superior to conventional laminectomy from a statistical perspective. Furthermore, interspinous device insertion has been shown to have a higher reoperation rate and to be less cost effective.
Conclusions A large prospective cohort study with a longer follow-up period comparing decompressive surgery alone versus interspinous device insertion for the treatment of lumbar spinal stenosis is needed to conclusively determine whether the interspinous device is beneficial.
Purpose The purpose of the study was to investigate the effect of obesity on the accuracy of percutaneous pedicle screw placement.
Materials and Methods We performed a retrospective analysis on the first 89 patients undergoing minimally invasive lumbar fusion with percutaneous pedicle screw placements for the treatment of degenerative lumbar spinal disorder.
Based on patient’s body mass index (BMI), patients were divided into 3 groups: group 1 – normal weight (BMI<25, 38 patients, 157 screws); group 2 – overweight (25≤BMI<30, 29 patients, 124 screws); group 3 – obese (BMI≥30, 22 patients, 89 screws). Using postoperative computed tomography (CT) scans, the position of placed screws to the pedicle or anterior body perforation was evaluated using the following grading method: Grade A, completely in the range without pedicle cortex violation; Grade B, pedicle wall violation<2 mm; Grade C, pedicle wall violation 2 to 4 mm; and Grade D, pedicle wall violation>4 mm.
Results Among the 370 pedicle screws, 308 screws (83%) were perfectly placed within the pedicle. Among the 62 misplaced screws, 45 screws were grade B pedicle breaches (73%, 45/62), and 45 screws were misplaced in lateral direction (73%, 45/62). 36 screws (10%) perforated the anterior vertebral cortex. Twenty eight screws were misplaced in overweight group, 12 screws in obese group, and 22 screws in normal weight group. With the number of screws available, subgroup analysis did not reveal a significant difference in the grade (p=0.10) or the direction (p=0.97) of pedicle breaches among groups.
Conclusion Our data suggest that obesity does not affect the accuracy of percutaneous pedicle screw placement. We do not hesitate or deny the surgery because of patient’s heavy body habitus, which seems to be a apparent benefit of minimally invasive spinal surgery.
Summary of Background Data Recently, minimal invasive spine surgery has been used and spine surgeons are prone to the radiation exposures.
Objectives: To determine the radiologic hazard to the spine surgeon.
Methods We searched the PUBMED, MEDLINE with Mesh term from MIS, radiation exposure.
Results We reviewed the radiation exposure in different disease and surgery. There exist significant dose of radiation exposures in MIS Discectomy, MIS or open pedicle screw fixation, and kyphoplasty.
Conclusion Surgeons should aware of the radiation exposure of the spine surgery and should do efforts on minimize it.
Neurological complications related to spinal surgery are not common, but can result in catastrophic clinical failures.
The ultimate goal during the operation should be to try to reduce and prevent a severe neurologic complication by careful preoperative planning and attention to trivial details related to the patients and their pathologies. It is very critical and important to understand the potential neurological complications that can occur during the operation and to manage them if they should happen. In our review article, general principles associated with various neurologic complications are reviewed and discussed.
Purpose The purpose of this study is to decrease the frequency of the perioperative complication and improve the clinical outcomes of multilevel lumbar degenerative disease by multilevel minimally invasive transforaminal lumbar interbody fusion.
Materials and Methods 317 patients(Minimally invasive transforaminal lumbar interbody fusion : 161, Conventional open surgery : 156) were followed up for more than 1 year. The age of each patient, the amount of intraoperative blood loss, the postoperative drainage, the transfusion requirement, surgery time, using of Intensive care unit, ambulation day, admission day and perioperative complications were investigated and analyzed.
Results Minimally invasive transforaminal lumbar interbody fusion was found to have a less blood loss, less using of Intensive care unit. And as the levels of union increase, disparities were increased(p<0.05).
But, surgery time of Minimally invasive transforaminal lumbar interbody fusion was longer, and as the levels of union increase, disparities were increased(p<0.05).
Conclusions Multilevel Minimally invasive transforaminal lumbar interbody fusion can be the better way, If surgery time of Multilevel Minimally invasive transforaminal lumbar interbody fusion can be reduced.
Discectomy or fusion have been a gold standard of the treatment for discogenic back pain. Since mid 1950s, spine surgeons have introduced the concept of arthroplasty for the management of low back pain. The current technologies are total disc replacement (TDR), posterior dynamic stabilization (PDS), interspinous process. Although many studies have reported their efficacy and safety, there are still lacking high-quality evidence. It is also not proven that these technologies are superior to spinal fusion in preventing the adjacent segment disease.
Second generation TDR is newly developed technology. The current TDR could allow the motion of flexionextension and lateral bending, but it did not have the capacity to bear the axial compressive force. Second generation TDR placed the shock-absorption materials that can endure the compressive force. The current TDR was performed through the anterior approach, which is invasive and necessitates the removal of anterior longitudinal ligament. To
overcome these disadvantages, TDR through lateral approach was developed. Various type of nucleus replacement technologies have been introduced with theoretical advantages over TDR such as less invasiveness, stable segmental motion and preservation of disc height. However, some of them had critical problems such as the migration and subsidence of implanted prosthesis. Total facet replacement arthroplasty was developed to overcome both the
adjacent segment disease after fusion and the instability after posterior decompression. Because most of reports about total facet replacement arthroplasty are based on the results from the animal or cadaveric study, the long-term human trial is required.
New technologies regarding motion preservation spinal surgery have been introduced, shifting paradigm in spinal care. Even though various attempts have been made in the field of spine surgery, the fact is that all of these attempts do not succeed due to paucity of better clinical outcomes. Thus, well designed long-term studies are required to prove their safety and efficacy, showing “superiority”, not just “no inferiority” to the traditional treatments.

 First
First Prev
Prev

