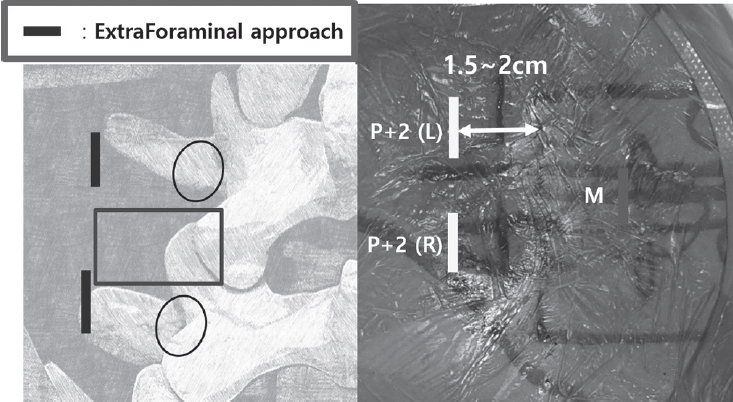
Purpose Revision lumbar surgery following posterior decompression is technically challenging because epidural adhesions and altered anatomy increase the risk of complications during posterior re-entry. Surgical approaches that avoid the previously operated corridor may reduce these risks. Biportal endoscopic lumbar interbody fusion using an extraforaminal approach allows direct neural decompression and interbody fusion through a new surgical corridor, which may be advantageous in revision settings. However, clinical evidence regarding this technique in revision surgery remains limited. To evaluate the clinical and radiological outcomes of biportal endoscopic revision extraforaminal lumbar interbody fusion (BE-REFLIF) performed at lumbar segments previously treated with central decompression.
Materials and Methods This study is Single-center retrospective case series.We retrospectively reviewed 20 consecutive patients who underwent single-level BE-REFLIF as revision surgery after prior central decompression between September 2017 and June 2024. Clinical outcomes were assessed using the visual analogue scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the EuroQol-5D (EQ-5D). Radiological outcomes included disc height, segmental alignment, lumbar lordosis, fusion status, and cage subsidence. Perioperative data and postoperative complications were also analyzed.
Results Significant improvements were observed in all clinical outcome measures during follow-up. Mean VAS scores for back and leg pain and ODI decreased significantly over time (p < 0.001). Radiological analysis demonstrated significant restoration of disc height, improvement in segmental alignment, and maintenance of lumbar lordosis. Solid fusion was achieved in 85% of patients at the final follow-up, and cage subsidence occurred in 25% of cases without the need for reoperation. Perioperative complications included dural tears in 10% of patients, epidural hematoma in 5%, and surgical site infection in 5%, with no instrumentation-related failures.
Conclusions Biportal endoscopic revision extraforaminal lumbar interbody fusion demonstrated favorable clinical and radiological outcomes in patients undergoing revision surgery after previous central decompression. By utilizing an extraforaminal corridor that avoids scarred posterior tissues, BE-REFLIF allows effective direct decompression and interbody fusion with an acceptable complication profile. This technique may represent a viable and less invasive option for selected patients requiring revision lumbar fusion.
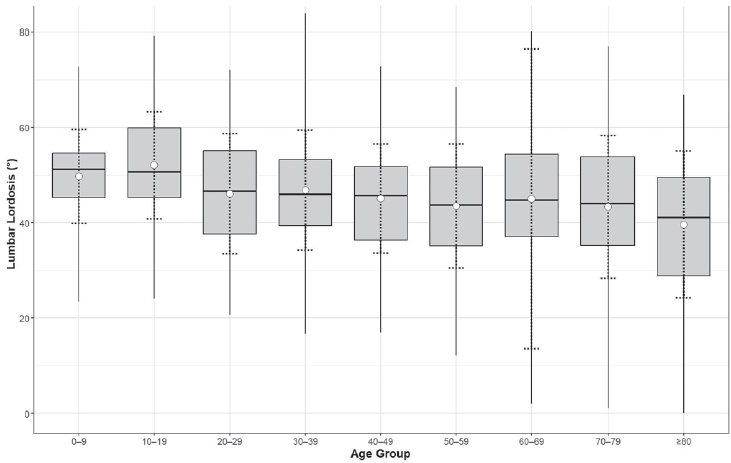
Purpose To evaluate the association between lumbar lordosis and age using an AI-based automated measurement model applied to a large dataset of standing lateral spinal radiographs.
Materials and Methods This retrospective study analyzed 904 high-quality radiographs selected from 2,397 images acquired between 2019 and 2021. Lumbar lordosis was defined as the angle between the superior endplates of L1 and S1 and automatically measured using a validated deep learning model. Subjects were categorized into nine age groups. One-way ANOVA compared lumbar lordosis across age groups, and Pearson correlation assessed the relationship between age and lumbar lordosis.
Results Lumbar lordosis ranged from 0° to 84° (mean 45.9°±13.4°). The highest mean value was in the 10–19-year group (52.1°), and the lowest in the ≥80-year group (39.6°). Minimum values decreased to 0° in individuals aged ≥60 years. No significant differences were found across age groups (p=0.561). A weak but significant negative correlation was observed between age and lumbar lordosis (r=–0.247, p<0.0001).
Conclusions AI-based automated measurement enabled efficient large-scale analysis and revealed a wide distribution of lumbar lordosis with a gradual age-related decline. These findings highlight the value of AI in spinal alignment assessment.
Purpose This study evaluates the performance of Claude and GPT LLM Vision APIs for automated clinical questionnaire processing in spine surgery by comparing accuracy, efficiency, reproducibility, and cost-effectiveness.
Methods Clinical questionnaires from 56 patients (336 total pages) were processed using a Python 3.12-based system incorporating PDF preprocessing, image enhancement via OpenCV, and direct LLM Vision analysis. Both models were evaluated on 26 questionnaire items (1,456 data points) using accuracy comparison, processing time measurement, token utilization analysis, and intra-class correlation coefficient (ICC) assessment through three independent iterations.
Results GPT achieved 98.83% accuracy (1,439/1,456) compared to Claude's 97.94% (1,426/1,456). Both models processed questionnaires in 27 seconds per set, representing 68% time reduction versus manual entry (85 seconds). GPT demonstrated 59% cost advantage ($0.023 vs. $0.056 per questionnaire), while Claude showed superior reproducibility (ICC 0.98 vs. 0.96). GPT achieved 100% accuracy across 21 items versus Claude's 17 items. Error analysis identified predominantly handwriting recognition (52%) and image quality issues (28%), with 89% of errors successfully flagged for review.
Conclusions Both models achieve clinical-grade performance exceeding 90% accuracy. GPT demonstrates superior accuracy and cost-effectiveness, while Claude provides better reproducibility. Model selection should be guided by institutional priorities regarding accuracy, reproducibility, and operational scale.
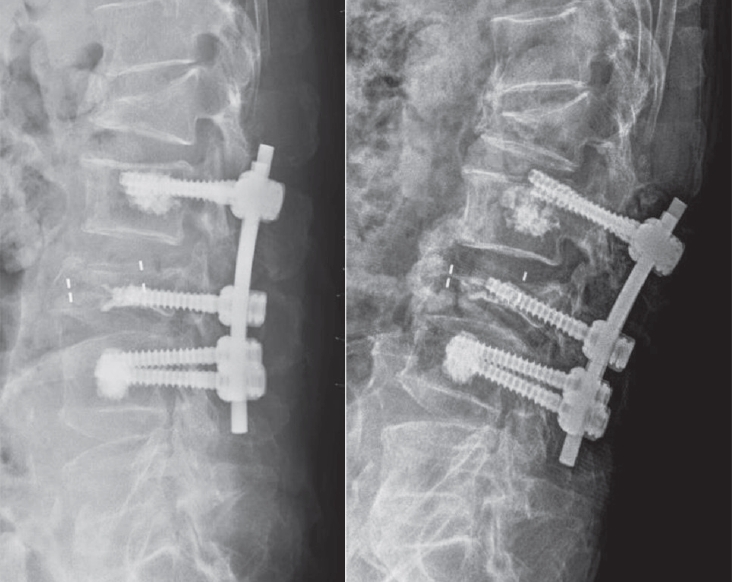
Objective This study aimed to evaluate the stability of cement-augmented pedicle screws in patients with osteoporosis of the thoracolumbar spine, with a focus on reducing mechanical failures compared with non-augmented screws.
Methods A retrospective analysis was conducted on 119 patients who underwent thoracolumbar fusion surgery between 2011 and 2022. The incidence of mechanical failures—including pull-out, screw loosening, and cage protrusion—was compared between patients treated with cement-augmented pedicle screws and those without augmentation.
Results Cement augmentation was associated with a significant reduction in overall mechanical failures. The incidence of mechanical failure was significantly lower in the cement-augmented group compared with the non-augmented group (20.4% vs. 41.4%, p=0.018). Although individual complications such as pull-out, cage protrusion, and screw loosening were less frequent in the cement-augmented group, these differences were not statistically significant. However, the overall reduction in mechanical failures was statistically significant. Fusion rates were higher in the cement-augmented group than in the non-augmented group, although the difference was not significant (79.6% vs. 70.0%, p=0.337). Importantly, patients without mechanical failures had significantly higher fusion rates than those with failures (82.5% vs. 56.41%, p=0.0048).
Conclusions Cement-augmented pedicle screws significantly reduce the risk of mechanical failures in thoracolumbar fusion surgery for patients with osteoporosis. Mechanical stability strongly influences fusion success, highlighting the importance of preventing mechanical failure to optimize surgical outcomes. These findings support cement augmentation as an effective strategy to enhance the durability of pedicle screw fixation and should be considered in surgical planning for patients with osteoporosis.
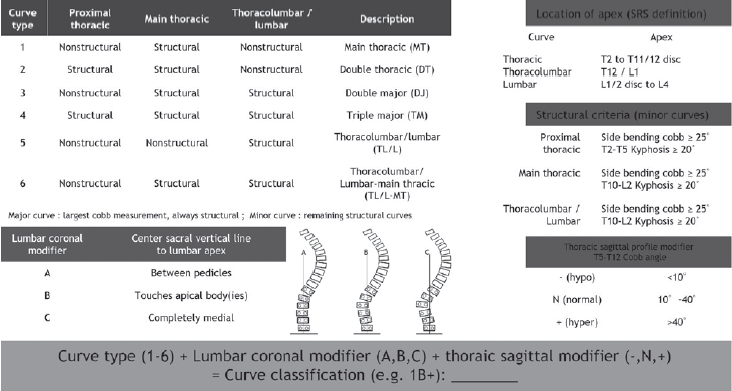
Adolescent idiopathic scoliosis refers to spinal deformity that develops from just before the onset of puberty until the completion of skeletal growth, and the primary goal of treatment is to achieve a well-balanced spine. In the late 1990s, advances in the anatomical understanding of the spine and the development of fixation instruments made posterior pedicle screw insertion feasible, thereby enabling the transmission of powerful corrective forces for deformity correction. Over the subsequent decades, accumulated clinical experience and outcomes have provided a deeper understanding of scoliotic curves and led to the establishment of effective principles for determining the extent of spinal fusion. However, these treatment principles are based on the unique biomechanics and procedural characteristics of scoliosis correction surgery, which can make them difficult to understand without sufficient explanation. In this review, we aim to describe these established treatment principles and surgical processes in detail using schematic illustrations and images. Although these principles will continue to undergo new challenges and validation over time, they will remain a meaningful reference point for those exploring alternative strategies.
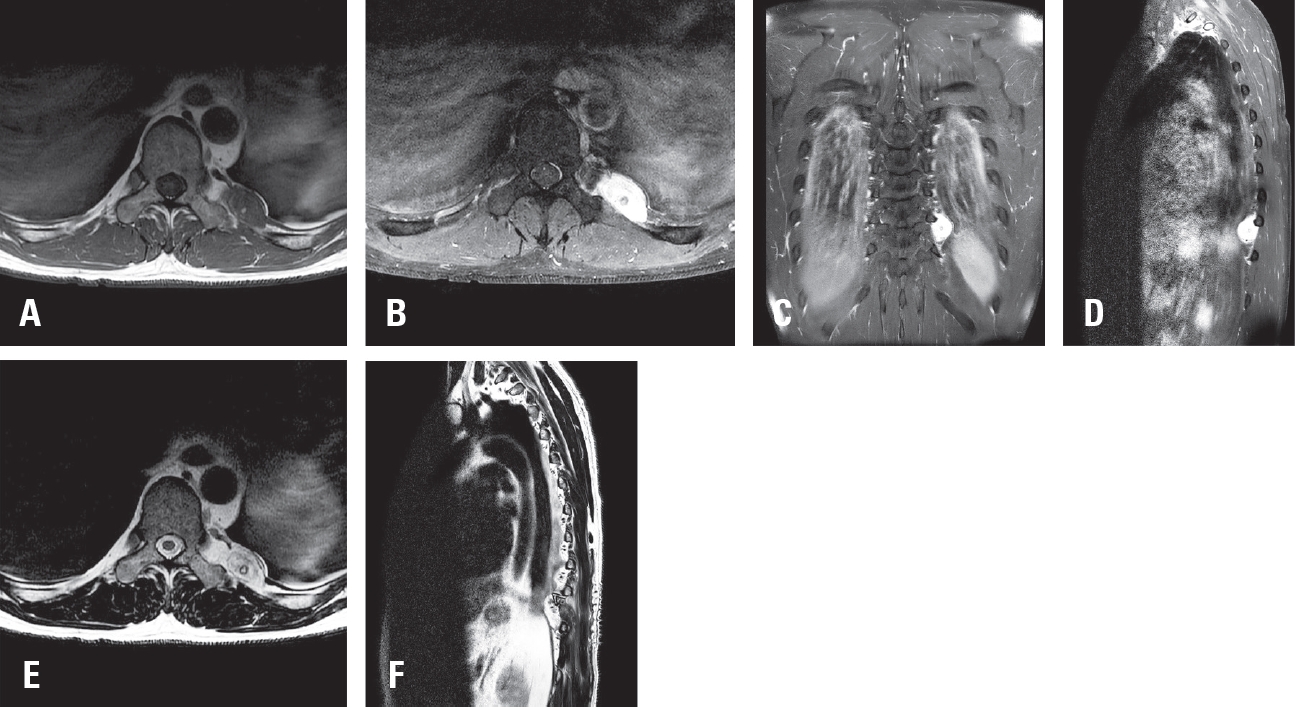
Purpose Glomangiomas of the spine are exceptionally rare benign vascular tumors, frequently misdiagnosed as more common lesions such as schwannomas or meningiomas. Although most spinal glomangiomas exhibit benign behavior, the presence of a BRAF V600E mutations may indicate uncertain malignant potential. Accurate diagnosis and complete surgical excision are essential for favorable outcomes.
Methods A 43-year-old male with left flank pain was evaluated with thoracic MRI and underwent surgical resection. Histopathological and molecular analyses were performed.
Results Thoracic magnetic resonance imaging (MRI) revealed a 2.8 cm ovoid, hypervascular mass adjacent to left T10 transverse process, extending to the posterior hemithorax. Surgical resection was performed, and histopathological examination confirmed a glomangioma with positive smooth muscle actin (SMA) expression and a BRAF V600E mutation.
Conclusions This case highlights the diagnostic challenge posed by paraspinal glomangiomas and emphasizes the importance of histopathological and molecular analysis in establishing the correct diagnosis. A review of the literature demonstrates that complete surgical excision remains the treatment of choice, with excellent prognosis. The identification of BRAF mutations may warrant closer follow up.
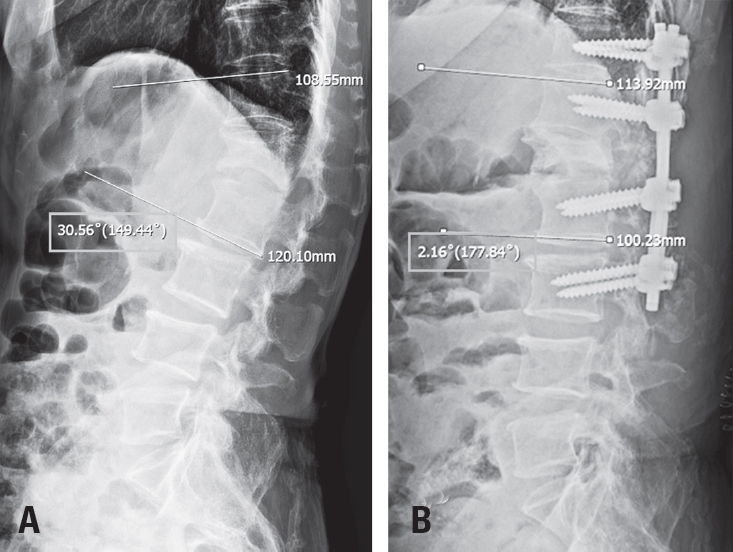
Tethered cord syndrome (TCS) is a condition in which the spinal cord becomes pathologically stretched due to various congenital or acquired etiologies, leading to progressive neurological symptoms. While surgical detethering is the gold standard for pediatric patients, adult-onset recurrent TCS presents a significant surgical challenge. Reoperation carries substantial risks—including spinal cord injury, cerebrospinal fluid leakage, and a high rate of retethering—often resulting in suboptimal long-term outcomes. Recently, spine-shortening osteotomy (SSO) has emerged as an alternative technique to reduce spinal cord tension without direct manipulation of the neural elements. Here, we report a case of recurrent adult TCS associated with a lipomyelomeningocele, which was exacerbated by post-traumatic kyphosis from an L1 compression fracture. The patient was successfully treated with SSO at the L1 level. This case highlights the utility of SSO as a safe and effective alternative to conventional revision detethering, particularly in complex cases involving spinal deformity.
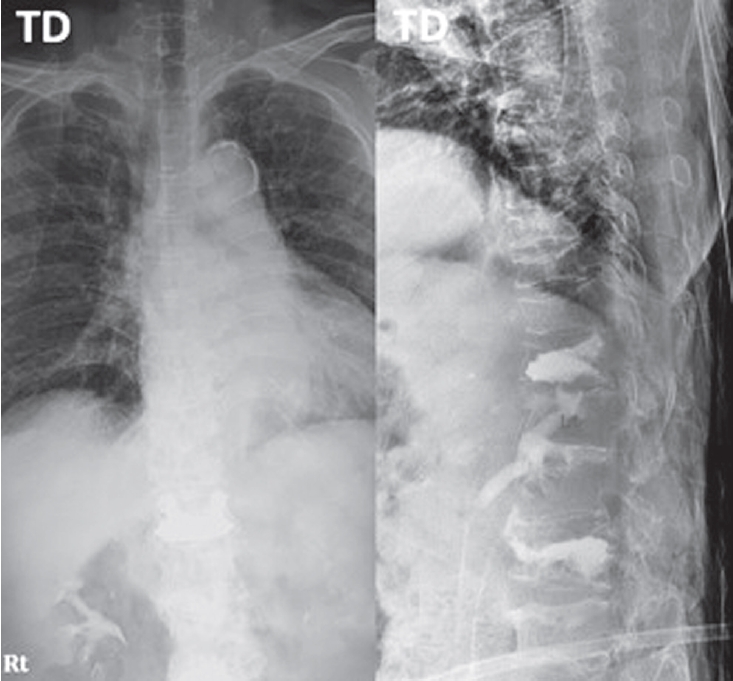
Purpose To evaluate the clinical and radiologic effects of switching from long-term bisphosphonate therapy to romosozumab in an elderly patient with severe osteoporosis and vertebra plana–type severe osteoporotic vertebral collapse, followed by transition to denosumab maintenance therapy.
Methods An 85-year-old woman with a history of osteoporotic fractures and prolonged intravenous bisphosphonate therapy presented with an acute L2 compression fracture. Conservative management with a body cast was initiated, and romosozumab was introduced as a switching therapy when anabolic treatment was indicated. Thoracolumbar spine radiographs were obtained at presentation and at 1, 3, 7, and 12 months after injury. Computed tomography was performed at presentation and again at 7 and 12 months to assess fracture consolidation. Bone mineral density (BMD) was measured beginning at 18 months after injury and annually thereafter. Functional assessments were recorded throughout a 30-month follow-up period.
Results During romosozumab therapy, the L2 vertebra plana–type severe osteoporotic vertebral collapse showed marked radiologic improvement, characterized by progressive intravertebral bone fill-in and gradual restoration of trabecular continuity without further loss of height. Serial follow-up CT and MRI demonstrated consolidation of the previously cavitated vertebral body, indicating substantial structural recovery rather than simple stabilization. Clinically, the patient experienced steady improvement in pain and ambulatory capacity. After completing six monthly doses of romosozumab, therapy was transitioned to denosumab. L2 bone mineral density improved from a T-score of –1.7 to –0.9, accompanied by gains in femoral BMD. No additional fragility fractures occurred throughout the follow-up period.
Conclusions Switching from long-term bisphosphonate therapy to romosozumab resulted in improved BMD, progressive vertebral bone fill-in, and stabilization without further collapse in this elderly patient with severe osteoporosis. Although not established as a fracture-healing agent, romosozumab may serve as a practical anabolic option in selected cases, with denosumab maintenance ensuring ongoing skeletal protection.
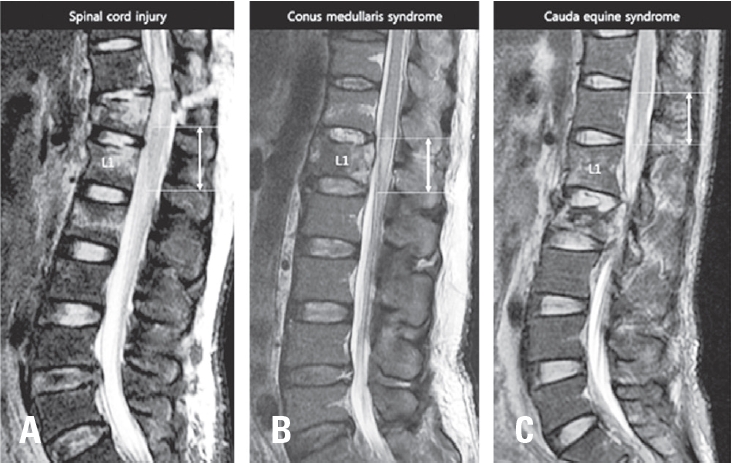
Background Neurogenic bladder dysfunction is a common and serious consequence of traumatic conus medullaris syndrome (T-CMS). Despite its clinical importance, predictive data for bladder outcomes after T-CMS remain limited. This study aimed to identify predictors of neurogenic bladder dysfunction at ≥2 years post-injury.
Methods We retrospectively reviewed 39 patients with acute T-CMS treated at a single level I trauma center from 2004–2017 who underwent spinal surgery and had ≥2 years of follow-up. Bladder function at 2 years was categorized as complete dysfunction, incomplete dysfunction, or normal. Potential predictors included demographic factors, injury mechanisms, ASIA Impairment Scale grades, MRI timing, fracture level and type, canal diameter, occupying ratio, conus signal change (normal, edema, or edema with hemorrhage), edema length, time to surgery, and surgical approach. Univariate and multivariate analyses were performed.
Results At final follow-up, 14 patients (35.9%) had complete bladder dysfunction, 12 (30.8%) had incomplete dysfunction, and 13 (33.3%) had normal function. Multivariate analysis identified edema with hemorrhage in the conus medullaris as the only independent predictor of bladder dysfunction.
Conclusions Bladder dysfunction is highly prevalent after T-CMS. Hemorrhagic edema in the conus medullaris significantly increases the risk of long-term neurogenic bladder dysfunction.
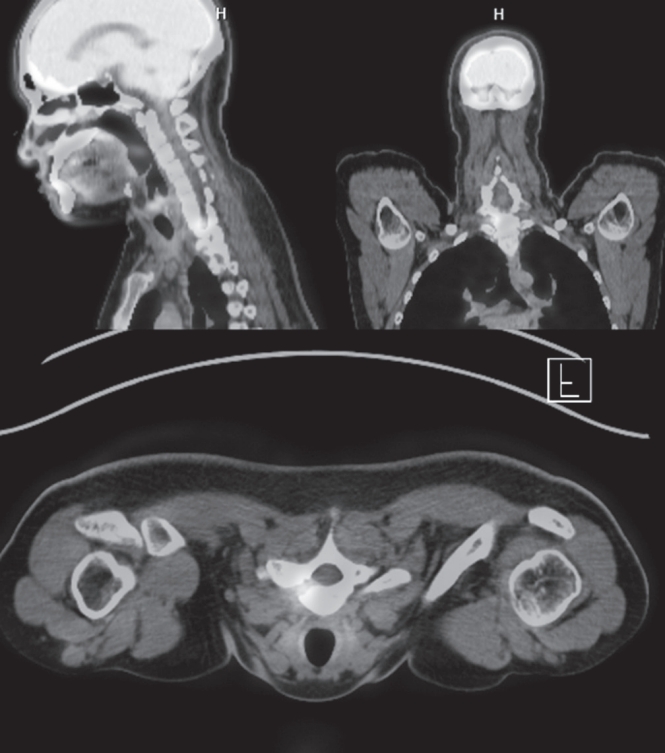
Osteoid osteoma is a benign bone-forming tumor that commonly affects young adults and often presents with severe nocturnal pain responsive to NSAIDs. While surgical resection is curative, lesions located in the spine, particularly near critical structures such as the vertebral artery and spinal cord, pose substantial diagnostic and surgical challenges. We report a case of a 24-year-old male with intractable night pain caused by an osteoid osteoma located at the superior margin of the right T1 pedicle. Despite extended NSAID therapy, the patient’s symptoms persisted. Multimodal imaging including MRI, CT, and PET-CT confirmed the diagnosis and revealed the lesion’s proximity to vital neurovascular structures. To minimize morbidity, we employed intraoperative O-arm navigation integrated with preoperative imaging to achieve precise localization and targeted resection through a limited posterior approach. The nidus was successfully excised en bloc without complications. Postoperatively, the patient experienced immediate pain relief and returned to normal activities within days. This case highlights the utility of real-time 3D navigation in managing spinal osteoid osteomas and supports its use as a safe, effective alternative to traditional wide exposure techniques, particularly in anatomically constrained regions of the spine.
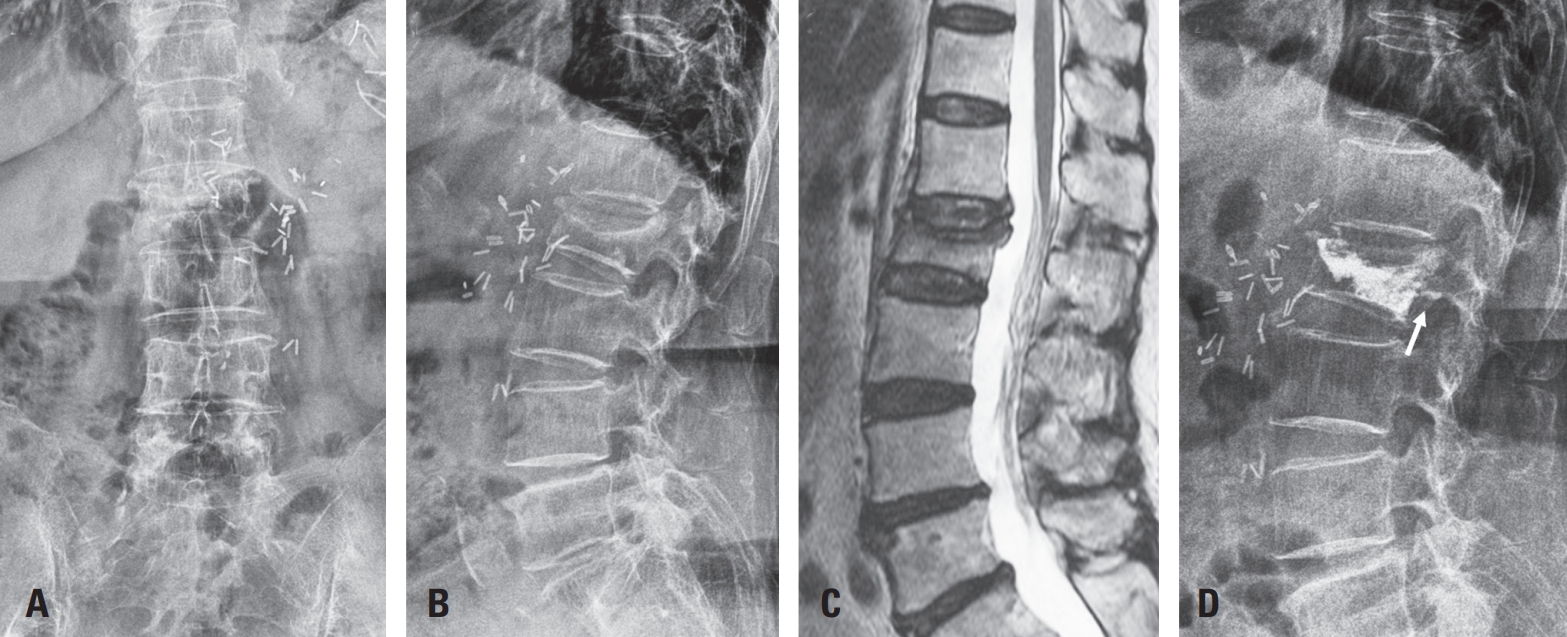
Vertebroplasty or kyphoplasty is a widely accepted minimally invasive procedure for treating painful vertebral compression fractures. Although considered safe, rare but serious complications such as spinal subdural hematoma (SDH) can occur, particularly in patients receiving long-term anticoagulation therapy. We present a rare case of spinal SDH following kyphoplasty in a 78-year-old woman with a mechanical aortic valve on chronic warfarin therapy. Anticoagulation was managed perioperatively with warfarin discontinuation and bridging enoxaparin. Postoperative X-ray showed subtle posterior cement leakage. MRI on postoperative day 1 revealed lumbar SDH, which progressed cranially by day 2. The patient remained neurologically intact and was treated conservatively with corticosteroids and temporary suspension of anticoagulation. Follow-up imaging showed gradual hematoma resolution, and she was discharged without deficits. This case suggests the importance of maintaining a high index of suspicion for spinal hematoma in anticoagulated patients, especially when new symptoms or even minor cement leakage are present. Careful perioperative planning, including early imaging and multidisciplinary management, is crucial in such high-risk patients.
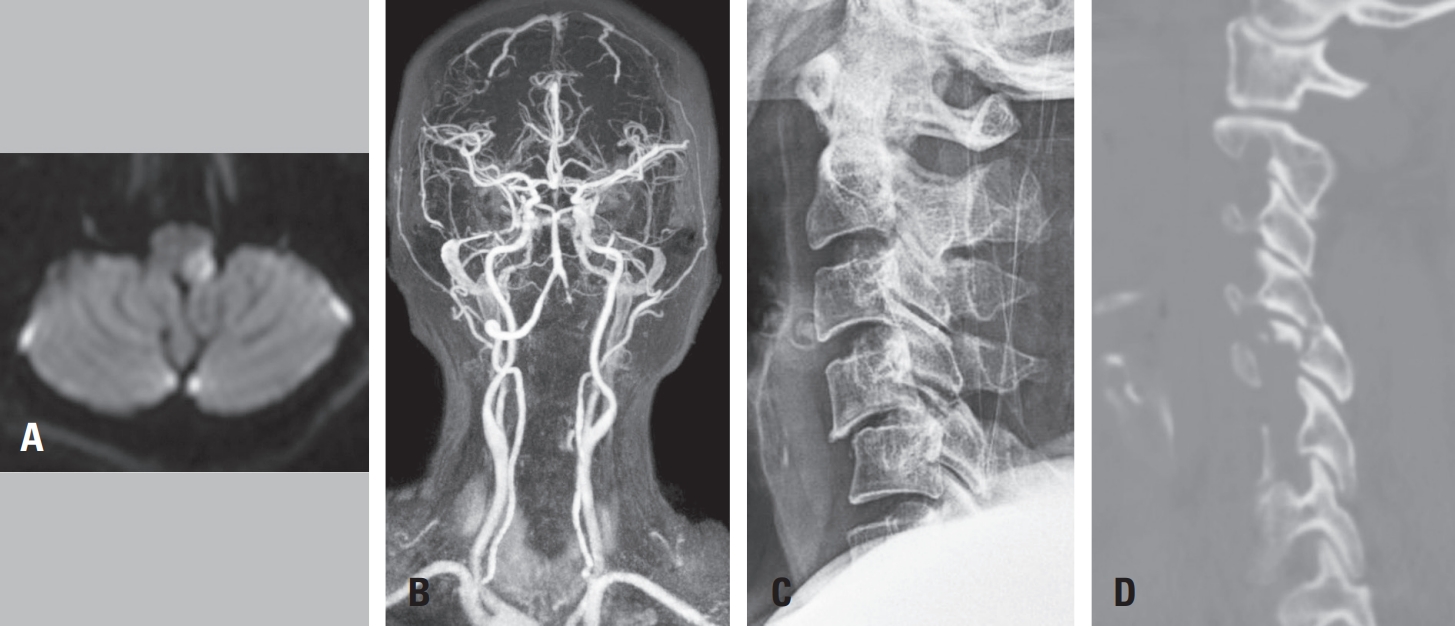
Purpose To report an uncommon case of Opalski syndrome following traumatic C4–C5 facet dislocation with vertebral artery dissection, and to discuss its diagnostic and therapeutic implications.
Materials and Methods A 60-year-old woman presented after a motor vehicle collision with bilateral upper limb weakness. Cervical X-ray, CT, MRI, and CT angiography revealed C4–C5 facet dislocation and left vertebral artery occlusion. Urgent anterior cervical discectomy and fusion were performed, and the postoperative course was monitored.
Results Immediate postoperative improvement to 4/5 strength in both arms was noted; however, new left facial numbness appeared at 12 hours and left lower limb weakness with gait ataxia at 48 hours. Brain MRI confirmed left lateral medullary infarction, and aspirin therapy was initiated. At one month, left arm strength recovered to 4/5, but ataxia persisted.
Conclusions In cervical trauma patients with C4–C5 facet dislocation and vertebral artery injury on initial imaging, the possibility of delayed lateral medullary infarction—particularly Opalski syndrome—should be considered. Prompt brainstem imaging and tailored antithrombotic therapy are essential when new neurologic deficits arise.
Study Design Retrospective comparative study.
Purpose To evaluate and compare the clinical outcomes and complication profiles of decompression alone versus decompression with instrumented fusion in elderly patients aged 75 and older with lumbar spinal stenosis. Overview of Literature: Lumbar spinal stenosis is a common cause of disability in elderly patients. The decision between decompression alone and fusion surgery in the geriatric population remains controversial due to surgical risks and comorbidities.
Methods A retrospective analysis of 121 patients aged ≥75 years treated either with laminectomy alone (n=60) or with posterior lumbar interbody fusion (PLIF, n=61) from April 2016 to December 2022. Baseline characteristics, perioperative parameters, and postoperative outcomes were compared.
Results There were no significant differences in baseline characteristics. The PLIF group showed longer operative times, greater blood loss, and longer hospital stay, but similar complication rates. Both groups showed significant postoperative improvement in VAS, ODI, and EQ-5D scores.
Conclusions Decompression alone and fusion surgery both provide substantial clinical benefit in elderly patients with spinal stenosis. With careful selection, fusion may be safely considered even in the elderly.
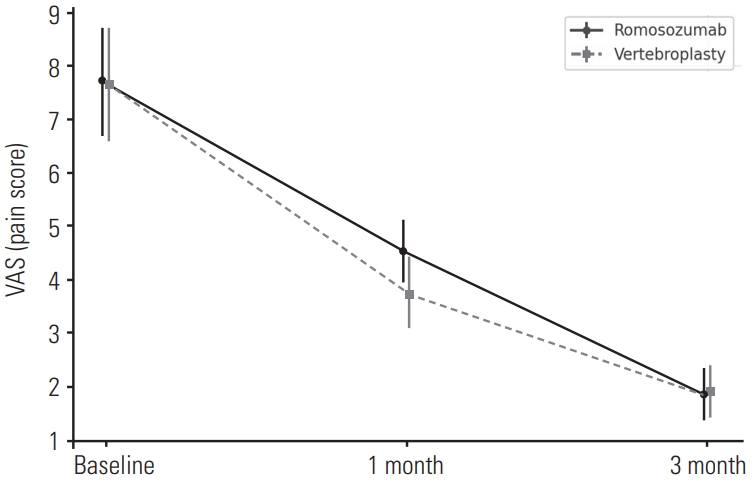
Purpose To compare the 3-month outcomes of romosozumab and percutaneous vertebroplasty in patients with acute osteoporotic vertebral compression fractures (OVCFs).
Background Vertebroplasty provides rapid pain relief in acute OVCFs but carries risks such as cement leakage and adjacent fractures. Romosozumab, an anti-sclerostin monoclonal antibody, promotes bone formation and reduces fracture risk; however, its effectiveness in acute OVCFs remains unclear.
Material and Methods: This retrospective study included 84 patients with MRI-confirmed acute OVCFs treated between January 2022 and December 2024. Patients received either monthly subcutaneous romosozumab injections (n=52) or vertebroplasty followed by weekly oral alendronate (n=32). All received daily calcium (500 mg) and vitamin D₃ (1,000 IU). Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI), and radiographic changes were evaluated based on anterior vertebral body height at baseline, 1 month, and 3 months.
Results Both groups showed significant improvements in VAS and ODI scores at 1 and 3 months, with no significant differences between them. Vertebral height changes were also comparable.
Conclusions Romosozumab-based conservative therapy may be a viable non-invasive alternative to vertebroplasty in treating acute OVCFs, offering similar short-term clinical and radiographic outcomes.

 First
First Prev
Prev

